



Heart transplantation has been an option for end-stage heart disease in children since the 1980s, and has become possible thanks to the development of immunosuppressive treatment; however, the treatment itself increases the risk for developing malignancies, predominantly post-transplant lymphoproliferative disorders.Reference Dipchand, Edwards and Kucheryavaya 1 – Reference Manlhiot, Pollock-Barziv and Holmes 5 This is frequently of B-cell origin, in which viruses such as Epstein–Barr virus typically drive malignant transformation. Approximately 95% of adults in the community are infected with Epstein–Barr virus. Upon infection, the virus incorporates itself in the B-cells, where it establishes by transforming the lymphocytes to perpetual lymphoblasts. If the natural protection of T-cell origin is hampered, Epstein–Barr virus infection induces a change in the growth pattern in the B-cells and neoplasms such as B-cell lymphoma, Burkitt’s lymphoma, nasopharyngeal carcinoma, or Hodgkin’s disease can develop. The thymus is of crucial importance for the development and maintenance of T-cell function. Most children who undergo heart surgery including sternotomy during infancy have their thymus partly or totally removed. There has been a tremendous development in surgical methods, anaesthesia, medication, and immunosuppressive treatment, and the overall morbidity and mortality for children undergoing transplantation has decreased.Reference Vanderlaan, Manlhiot, Edwards, Conway, McCrindle and Dipchand 6 In spite of this development, our unit witnessed an increase in post-transplant lymphoproliferative disorder cases during recent years. The objective of this study was to analyse the prevalence of post-transplant lymphoproliferative disorder among children undergoing heart transplantation in Gothenburg, in order to identify possible risk factors in this population.
Material and methods
Paediatric heart transplantation has been available in Sweden since 1989 and the coordination of listing, transplantation, and organ procurement is carried out within the framework of the Scandiatransplant organisation (Aarhus, Denmark). It is centralised to two centres, Gothenburg and Lund.Reference Gilljam, Higgins, Bennhagen and Wåhlander 7 The protocol for immunosuppression has undergone development over time; in 2007, our unit switched antithymocyte globulin preparation from Thymoglobulin (Sanofi Genzyme, Cambridge, United Kingdom) to ATG-Fresenius (Fresenius Kabi, Uppsala, Sweden). There has been a gradual shift in triple immunosuppression therapy, from ciclosporine, azathioprine, and prednisone towards a tacrolimus-based regimen, including mycophenolate mofetil. Steroids were regularly weaned after 6 months. In children undergoing transplantation as toddlers with a benign rejection history, mycophenolate was usually weaned after 2 years. In older children, mycophenolate dosage was not increased with growth, leading to an effective reduction in dosage. The target level for tacrolimus was reduced over time to reach 6 µg/L by 2 years or earlier in younger children. Prophylactic treatment with antivirals such as valganciclovir is used when there is a mismatch concerning cytomegalovirus.
The protocol for follow-up has undergone minor changes during this 25-year period, including fewer endomyocardial biopsies and the possibility to obtain real-time viral load with polymerase chain reaction, which is especially useful for obtaining viraemia of Epstein–Barr virus infection and cytomegalovirus.
Serostatus and degree of viraemia of Epstein–Barr virus and cytomegalovirus is obtained at every biopsy, which is carried out eight times during the 1st year after transplantation, and once yearly thereafter. Surveillance includes physical examination at check-up every 3 months. When viraemia levels are rising or above log 4–5 copies/ml, the immunosuppression is lowered and a CT scan of the chest and stomach is performed. Treatment with Rituximab is considered.
As the exact radiation exposure was impossible to obtain, the number of X-ray scans, angiographies and CT scans were counted, comparing patients developing lymphoma with those not developing lymphoma, exposed during the same time period.
Data collection procedures and variables
This report is based on a retrospective analysis of all subjects below 18 years of age who underwent heart transplantation in Gothenburg between January, 1989 and December, 2014.
Medical reports were reviewed, focussing on gender, age at transplantation, listing diagnosis, recipient’s Epstein–Barr virus serostatus at the time of transplantation, induction treatment, immunosuppressive treatment, development of malignancy, and mortality. Heart defects were classified according to the systemic ventricle in biventricular defects and according to the hypoplastic ventricle in defects palliated with univentricular palliation. Type of surgery was classified as sternotomy or no sternotomy, focussing on the subject’s 1st year of life. Sternotomy includes total or partial thymectomy. Lymphoma was defined as post-transplant lymphoproliferative disorder, verified by histologic examination in a biopsy.
Statistical methods
Continuous data are presented as mean, SD, median, minimum, and maximum, and categorical data are presented as counts and percentage of total. To describe time-to-event rates the Kaplan–Meier plot was used. For comparison of time-to-event among groups the log-rank test was used for dichotomous variables and log-rank test for ordered categorical variables. As the numbers of events described as post-transplant lymphoproliferative disease were only 11, only univariable Cox proportional hazards regression analyses was performed. Hazard ratios with 95% confidence intervals were calculated using Cox models. The proportional hazard assumption was verified by review of log (−log survival) versus log (time). All statistical analyses were two-sided and conducted at the 5% significance level. All statistical analyses were performed with SAS Software Version 9.3; SAS Institute Inc., Cary, North Carolina, United States of America.
Results
A total of 71 children between 3 weeks and 18 years of age underwent heart transplantation in Gothenburg between 1 January, 1989 and 31 December, 2014. The overall incidence of post-transplant lymphoproliferative disorder was 14% (10/71). See Figure 1; however, this varied over time: 11% (4/35) of those who had undergone heart transplantation before 2007 developed malignancy, compared with 17% (6/36) of those who had undergone heart transplantation in the later period (p=0.85).
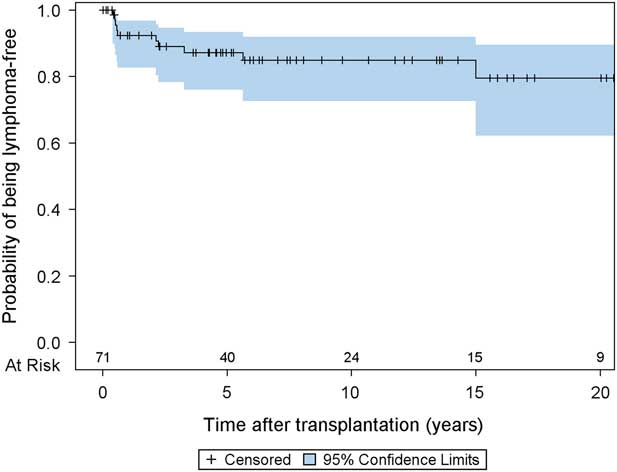
Figure 1 Kaplan-Meier graph for time to lymphoma.
Descriptive data of children with and without lymphoma are summarised in Table 1. Univariable Cox proportional hazards regression analyses of time to lymphoma are presented in Table 2. Age at transplantation did not turn out to be a risk factor for lymphoma. There was a difference in listing diagnosis, as not a single case with post-transplant lymphoproliferative disorder was found among those with cardiomyopathy (p=0.0003).
Table 1 Descriptive data for all patients, including a comparison between patients with and without lymphoma.

EBV d/r neg/pos=Epstein–Barr virus donor/recipient positive/negative.
For categorical variables n (%) is presented.
For continuous variables mean (SD)/median (min; max)/n is presented.
4 June, 2017 analysis (SAS).
Table 2 Univariable Cox proportional hazards regression analyses of time to lymphoma

CI=confidence intervals; HR=hazard ratios; Non-est=non-estimable.
For dichotomous variables p-values are obtained from the log-rank test. For the continuous and ordered categorical variables p-values are obtained from the Cox regression analysis.
4 June, 2017 analysis (SAS).
Among the patients developing lymphoma, nine had left ventricular hypoplasia (p⩽0.0001), Table 1. One child with biventricular defect and aortic stenosis, developed post-transplant lymphoproliferative disorder. For a detailed report on the type of CHD as an indication for transplantation, see Table 3. There was a trend for CHD to become more common during the observed time period, 42% in 1989–2006 compared with 56% in 2007–2014 (p=0.55), and there was a shift in heart defects as listing diagnosis; biventricular circulation constituted 22% of listing diagnoses before 2007 compared with 8% after this date, whereas univentricular palliation tripled from 14% (5/35) in the earlier period to 47% (17/36) in the later period.
Table 3 Type of heart defects among children who had undergone transplantation because of structural heart defects: comparison of development or absence of post-transplant lymphoproliferative disorder.

The majority of the children who developed post-transplant lymphoproliferative disorder had undergone at least one sternotomy during the 1st year of life, before heart transplantation, most commonly during the first 2 weeks after birth. About one-third – that is, 9 of 30 – who underwent sternotomy as infants developed lymphoma (p⩽0.0001; Fig 2).
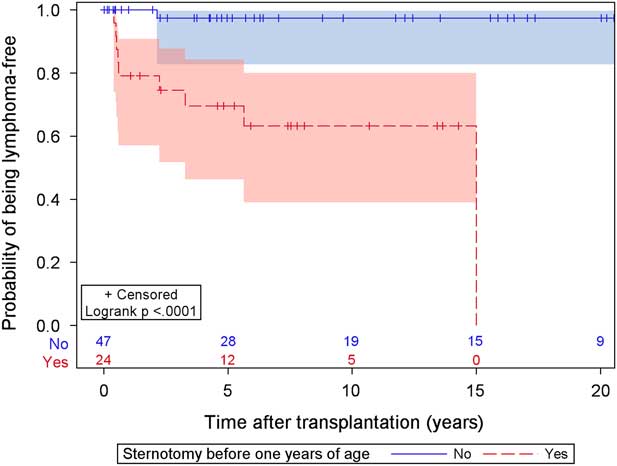
Figure 2 Kaplan-Meier graph for time to lymphoma by Sternotomy before one year of age.
Number of surgical events turned out to be a risk factor for development of post-transplant lymphoproliferative disorder (p=0.0001), Figure 3. Overall, 35 of 71 children with heart transplants had undergone surgery before transplantation, 91% (32/35) for CHD and 8% (3/36) for cardiomyopathies. Among the three children with cardiomyopathies and surgery, two had undergone surgery in infancy, one for aortic coarctation and one for an atrial septal defect, and the third one had undergone surgery in childhood for aortic coarctation. Of the children, three with CHD had not undergone surgery before transplantation: one had Ebstein anomaly, one had hypoplastic left heart syndrome and received the allograft in the United States of America, and one was born with a hypoplastic right ventricle, pulmonary stenosis, and a ventricular septal defect; she received a heart transplant at 3 years of age.
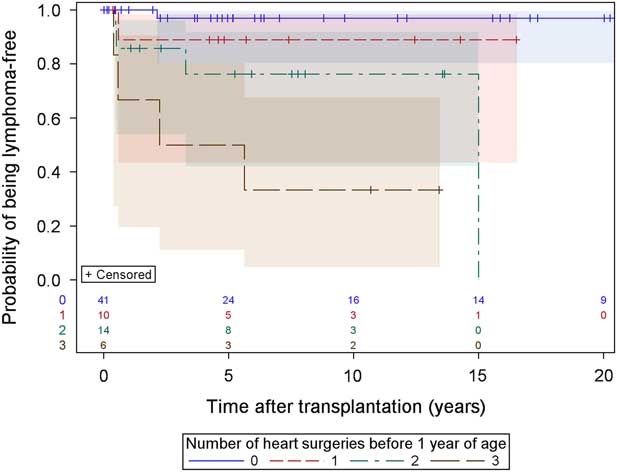
Figure 3 Kaplan-Meier graph for time to lymphoma by Number of heart surgeries before 1 year of age.
Extracorporeal membrane oxygenation was used in 14 subjects, seven with cardiomyopathies and seven with CHD, at a median time of 6.5 days (1–58) before transplantation. At the time of transplantation, 12 children were on ventricular assist device support as bridge therapy.
A mismatch concerning Epsten–Barr virus, with a seropositive donor and a seronegative recipient, turned out to be a significant risk factor for development of post-transplant lymphoproliferative disorder (p=0.0001).
Thymoglobulin was consistently used as induction treatment during the first 18 years, and then gradually changed to ATG-Fresenius, without statistical connection to lymphoma (p=0.061).
Immunosuppressive treatment with tacrolimus was a risk factor for lymphoma compared with ciclosporine (p=0.028); however, the shift in treatment from ciclosporine in the first time period to tacrolimus in the later period coincides with other changes: for example, the shift to univentricular circulation as listing diagnosis.
Overall, 20 subjects succumbed and the causes of death were lymphoma in four, rejection in five, graft dysfunction in three patients, and Kaposi’s sarcoma, renal failure, aplastic anaemia, pulmonary hypertension, myocarditis, hypertrophic cardiomyopathy in the donor, immune deficiency, and an accident in one patient each. Standardised mortality ratio was 97.8 for the whole group of children with heart transplants.
Post-transplant lymphoproliferative disorder
Patient characteristics for children diagnosed with post-transplant lymphoproliferative disorder are summarised in Table 4. The mean duration between transplantation and diagnosis was 2.6 years (range 5 months to 15 years). The majority developed lymphoma within 2 years of transplantation. The majority had diffuse large B-cell lymphoma with a survival rate of 5/8; one survivor had Burkitt’s lymphoma, whereas the child with polymorphic lymphoma has succumbed. All subjects with post-transplant lymphoproliferative disorder had CHD, all receiving sternotomy as the surgical intervention up to seven times before heart transplantation; all but one had left ventricular hypoplasia and none was known to be positive for Epstein–Barr virus infection at the time of transplantation.
Table 4 Patient characteristics of the children who developed post-transplant lymphoproliferative disorder after heart transplantation

EBV=Epstein–Barr virus; F=female; HTX=heart transplantation; M=male.
Radiation exposure
In nine of 10 children diagnosed with post-transplant lymphoproliferative disorder the number of X-ray scans, CT scans, and angiographies could be compared with 13 patients without development of malignancy: the number of X-rays were 117/person compared with 109/person (p=0.083), CT scans were 3.8/person compared with 5/person (p=0.97), and angiographies were 17/person compared with 23 (p=0.76).
Syndromes and genetic abnormalities
Among the children with CHD, three were diagnosed with genetic syndromes: one girl had Turner syndrome and unbalanced atrioventricular septal defect with aortic atresia, one girl had left ventricular hypoplasia, and one boy had Noonan syndrome and aortic atresia with a ventricular septal defect. One boy with dilated cardiomyopathy had Becker’s disease and two girls with hypertrophic cardiomyopathy had Danon’s disease.
Comorbidity
In all, four children with CHD had protein-losing enteropathy before transplantation; two of them developed lymphoma. One girl had undergone liver transplantation 2 years before heart transplantation. Among children with cardiomyopathy, three had undergone previous treatment for malignancies, including anthracyclines for all three and radiation to the thoracic region including the heart for one. Another child was born with a severe congenital immune deficiency, treated twice with bone marrow transplantation as an infant. A single boy developed a rare form of cancer, Kaposi’s sarcoma, leading to death at 14 months post-transplantation.
Discussion
This study has three major findings. First, post-transplant lymphoproliferative disorder only developed in subjects born with CHD. Second, all subjects developing lymphoma had undergone sternotomy as infants. Third, the number of surgical events carried a higher risk for development of lymphoma.
CHD
In the present study, CHD was a risk factor for development of post-transplant lymphoproliferative disorder, as no subject with cardiomyopathy developed the malignancy. To our knowledge, this has not been reported before; however, the data concerning malignancy in the largest international registry are limited.Reference Dipchand, Edwards and Kucheryavaya 1 Large international studies indicate that palliated CHD is a significant risk factor for death.Reference Dipchand, Edwards and Kucheryavaya 1 , Reference Hetzer, Weng and Walter 8 In contrast, in several studies, including those based on large multicentre registries, the long-term outcome is reported to be similar for subjects with transplants for CHD and for those with cardiomyopathy.Reference Manlhiot, Pollock-Barziv and Holmes 5 , Reference Hetzer, Weng and Walter 8 , Reference Greutmann, Pretre and Furrer 9 In our cohort, children with different forms of left ventricular hypoplasia constituted an especially vulnerable group, as 9/10 children with post-transplant lymphoproliferative disorder belonged to this group. Nearly half of the children transplanted for left ventricular hypoplasia developed lymphoma (9/21). Newborns with hypoplastic left heart syndrome have been reported to have a high mortality during surgery, with the exception of heart transplantation as an alternative to palliative surgery.Reference Dipchand, Edwards and Kucheryavaya 1 , Reference Hetzer, Weng and Walter 8 , Reference Chinnock and Bailey 10 , Reference Voeller, Epstein, Guthrie, Gandhi, Canter and Huddleston 11 An associated congenital immune defect could be an explanation for this increased risk for post-transplant lymphoproliferative disorder. Children born with CHD sometimes have an impaired immune system, as in Down syndrome and DiGeorge syndrome; however, there were no children with these syndromes in our cohort. Hypoplastic left heart syndrome is associated with Turner syndrome and Noonan syndrome, without associated immune deficiency.
Surgery
All subjects developing post-transplant lymphoproliferative disorder had undergone heart surgery, including sternotomy and cardiopulmonary bypass one to seven times before transplantation (median 3 times). Extracorporeal circulation activates the acute inflammatory response with raised serum levels of cytokines such as interleukin 6, 8, and 10.Reference Finn, Naik, Klein, Levinsky, Strobel and Elliott 12 – Reference Adrian, Skogby, Gatzinsky, Friberg and Mellgren 14 An activated inflammatory response might theoretically increase the risk for lymphoma and in the present study the risk was significantly increased with the number of surgical events. In our cohort, three of 14 treated with extracorporeal membrane oxygenation developed post-transplant lymphoproliferative disorder; in spite of the fact that seven of the subjects had cardiomyopathies, none of them developed lymphoma. In contrast, all those who developed lymphoma had undergone extracorporeal circulation interventions during infancy.
As the large size of the thymus hampers surgical access to the heart, some form of thymectomy is necessary in most surgeries performed for CHD during infancy. The consequences of thymectomy in infants are controversial, but the procedure does result in some degree of immunodeficiency.Reference Halnon, Jamieson, Plunkett, Kitchen, Pham and Krogstad 15 – Reference Gudmundsdottir, Oskarsdottir and Skogberg 17 Long-term studies report persistent lymphopaenia and low signal joint T-cell receptor circle levels during the first 5 to 10 years after surgery, but 20–30 years later there is a trend toward a normalised immune system.Reference Ferrnado-Martinez, Munoz-Fernandes and Leal 18 This cohort of subjects, subjected to thymectomy as infants, immunosuppresion at heart transplantation, and an iatrogenic lifelong suppression of the T-cell system might be vulnerable, especially during the first 10 years after transplantation. The incidence of post-transplant lymphoproliferative disorder was 32% (10/31) among those who had undergone sternotomy before transplantation in our cohort of patients.
The overall incidence of lymphoma during the observed period, 10% during the first time period and 17% during the later period, was within the reported rate of 1–28%.Reference Gajarski, Blume and Urschel 2 , Reference Manlhiot, Pollock-Barziv and Holmes 5 , Reference Chinnock and Bailey 10 , Reference Benden, Aurora and Burch 19 – Reference Kumarasinghe, Lavee and Parker 21 We found an increased incidence of early-onset post-transplant lymphoproliferative disorder, in contrast to other reports.Reference Chinnock, Webber, Dipchand, Brown and George 22 The fact that the listing diagnosis shifted from a dominance of cardiomyopathy during the early years in favour of CHD with univentricular palliation could at least partly explain this increased incidence of lymphoma.
Epstein–Barr virus infection
The strongest risk factor for the development of post-transplant lymphoproliferative disorder is considered to be primary infection with Epstein–Barr virus after transplantation, especially when the donor is seropositive.Reference Gajarski, Blume and Urschel 2 , Reference Webber, Naftel and Fricker 4 , Reference Kumarasinghe, Lavee and Parker 21 , Reference Allen and Preiksaitis 23 – Reference Schubert, Abdul-Khaliq and Lehmkuhl 26 Not unexpectedly, the vast majority of subjects in the present study who developed post-transplant lymphoproliferative disorder were seronegative before transplantation, and seven of them received a seropositive heart. There is an increasing interest in trying to prevent Epstein–Barr virus disease, by developing a vaccine and conducting trials with the infusion of intravenous immunoglobulin, but, so far, there are no such options for effective treatment of the disease.Reference Green and Michaels 24 The group of infants with hypoplastic left heart syndrome, a severe CHD, might not be exposed to community infections to the same extent as healthy children, further increasing the risk for being seronegative at the time of transplantation.
Induction therapy and immunosuppressive treatment
The protocol for immunosuppression changed during this study, as described above; nonetheless, it is unlikely that the protocol was a risk factor for developing lymphoma, as no individual with cardiomyopathy developed lymphoma. Even if there was an increased incidence of lymphoma after the change from Thymoglobulin to ATG-Fresenius, we did not find a statistical connection to lymphoma. This is consistent with the report from the Pediatric Heart Transplant Study, in which the incidence of post-transplant lymphoproliferative disorder was comparable for children treated with ATG-Fresenius and those treated with Thymoglobulin.Reference Gajarski, Blume and Urschel 2 Although there might have been some small individual deviations, all subjects were treated according to the same protocol; moreover, large studies have not reported an increased incidence of lymphoma related to choice of induction therapy.Reference Gajarski, Blume and Urschel 2 , Reference Hayes, Breuer, Horwitz, Yates, Tobias and Shinoka 20 , Reference Kumarasinghe, Lavee and Parker 21 , Reference Schubert, Abdul-Khaliq and Lehmkuhl 26 , Reference Gao, Chaparro and Perlroth 27 Mortality rate and causes of death are similar to those reported in other studies.Reference Dipchand, Edwards and Kucheryavaya 1 , Reference Hetzer, Weng and Walter 8 , Reference Chinnock and Bailey 10
Radiation exposure
In the present study, there was no evidence supporting increased radiation exposure in the cohort that developed post-transplant lymphoproliferative disorder, as reported in a study from Canada.Reference Seal, Hawkes and Bhargava 28 It is generally accepted that there is a dose-response relation between radiation and lymphoma; however, large studies show a protracted induction and a latency period for decades.Reference Richardson, Sugiyama and Wing 29
In the cohort of children undergoing heart transplantation in Gothenburg during a period of 25 years, all 10 of the 71 subjects developing post-transplant lymphoproliferative disorder had CHD, the majority had a hypoplastic left ventricle, all had undergone sternotomy, and the majority had undergone repeated surgery before transplantation. Thus, these can be seen as potential risk factors for post-transplant lymphoproliferative disease.
Limitations of the study
Our cohort remains small, nonetheless, we have the advantage of Sweden’s a comprehensive health care system, allowing access to reliable data and with few patients lost to follow-up.
Acknowledgements
The authors thank Aldina Pivodic and Statistiska Konsultgruppen.
Financial Support
Financial support was provided through the regional agreement on medical training and clinical research (ALF) between Gothenburg County Council and Gothenburg University and the Queen Silvia Children’s Hospital Foundation and from the Mary Beve’s foundation.
Conflicts of Interest
None.
Ethical Standards
The study was approved by the Central Ethical Review Board at Gothenburg University, Gothenburg.







