


Introduction
Gaining vascular access is essential in the resuscitation of critically ill patients. Intravenous (IV) access is the first-choice vascular access for adult emergencies.Reference Lamhaut, Dagron and Apriotesei 1 Intraosseous (IO) placement is a primary alternative to IV access in conditions where IV access delays resuscitation or is not possible.Reference Lamhaut, Dagron and Apriotesei 1 - 3 Additionally, IO access is the first-line vascular access for pediatric emergencies.Reference Lamhaut, Dagron and Apriotesei 1 , Reference Biarent, Bingham and Richmond 4 - 6 This report presents a case of prehospital misplacement of an IO catheter into the intra-articular space of the knee joint when access was attempted in the field. To the authors’ knowledge, this complication has not been reported previously in the literature.
Report
A 42-year-old male bicyclist presented to the emergency department (ED) via Emergency Medical Services (EMS) after being struck by a motor vehicle. The patient was wearing a helmet and did not lose consciousness. Per EMS, the patient complained of abdominal pain and shortness of breath, and his systolic blood pressure was in the 80s in the field. Emergency Medical Services attempted IO line placement in the right proximal tibia, and IV fluids were administered prior to arriving in the ED.
At presentation to the ED, the patient was in no acute distress. The patient's vital signs had improved to a blood pressure of 124/74 with a heart rate of 85 beats/minute. His respiratory rate was 20, and his oxygen saturation was 100%. His physical exam was significant for epigastric tenderness without guarding and abrasions over the left flank, left thigh, left knee, and bilateral ankles. An IO line was noted in the right proximal tibia by the emergency physician. The catheter appeared to be very close to the joint line (Figure 1).

Figure 1 Clinical Photograph of Intraosseous Catheter Placed in Right Knee.
X-rays of the chest and pelvis and computed tomography scans of the abdomen, pelvis, and lumbosacral spine were unremarkable. Radiographs of the right knee and right tibia and fibula were performed to assess IO placement. Anteroposterior (AP) and lateral X-rays of the right knee revealed intra-articular placement of the IO catheter (Figure 2).

Figure 2 Anteroposterior (A) and Lateral (B) Radiographs of Right Knee Revealing Intraosseous Needle in Intra-articular Space.
The orthopaedic surgery service was consulted for management. After sterile preparation of the skin, an additional 18-gauge angiocatheter needle was placed into the superolateral portal of the knee joint. One liter of sterile saline was lavaged through the knee (Figure 3). Both needles were removed, and a sterile dressing was applied. Anteroposterior and lateral radiographs, as well as a photograph of the right knee, were obtained after removal of the IO catheter. The patient was allowed to bear weight as tolerated through his knee, and he recovered without complication.

Figure 3 Clinical Photograph of Right Knee During Lavage.
Discussion
This case of IO catheter placement into the knee joint was managed with joint lavage and catheter removal. Although IO vascular access is generally a safe and effective resuscitation technique, IO lines placed incorrectly can have devastating effects, including compartment syndrome, muscle necrosis, major bleeding, and infection.Reference Lamhaut, Dagron and Apriotesei 1 , Reference LaRocco and Wang 7 - Reference Buck, Wiggins and Sesler 10
The most common IO insertion site in children and adults is the proximal tibia. Other common sites include the lateral aspect of the humeral head and the sternum.Reference Paxton 11 Reades et al demonstrated that the first-attempt success rate of IO insertion into the proximal tibia was greater than into the proximal humerus during resuscitation of cardiac arrest patients.Reference Reades, Studnek, Garrett, Vandeventer and Blackwell 12 For proper proximal tibial insertion, the IO catheter should be inserted into the anteromedial proximal tibia distal to the level of the tibial tubercle.Reference Cooper, Mahoney, Hodgetts and Mellor 13 More proximal placement should be avoided due to the fact that the knee capsule inserts on the tibia 14 mm distal to the articular surface of the tibial plateau, and intracapsular insertion places the joint at risk for infection.Reference Decoster, Crawford and Kraut 14 Figure 4 illustrates the proper IO catheter insertion point in the proximal tibia. Placement of the IO catheter may be more challenging in emergent conditions and when external landmarks are more difficult to identify, such as in obese patients or patients with variant anatomy.
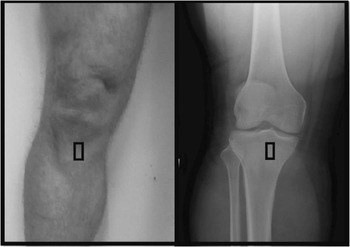
Figure 4 Clinical Photograph and AP Radiograph of Right Knee: Black Box Indicates Proper IO Catheter Insertion Point in the Anteromedial Proximal Tibia.
Abbreviations: AP, anteroposterior; IO, intraosseous.
There are few absolute contraindications to IO line placement. They include fracture or osteotomy of the bone, the presence of a prosthetic bone or joint, active infection at insertion site, recent IO access attempts in the same bone, and inability to identify external landmarks at insertion site.Reference Paxton 11
Several complications of IO vascular access have been documented. The most common complication is fluid extravasation, which can cause compartment syndrome and muscle necrosis. Other previously identified complications of IO placement include osteomyelitis, soft-tissue infection, breaking or bending of the IO needle, and air or fat emboli.Reference Paxton 11 , Reference Fenton, Bali, Sargeant and Jeffrey 15
As this case demonstrates, insertion of the IO needle into the intra-articular space is an additional complication of IO vascular placement. Intra-articular placement of the IO needle would not allow for effective resuscitation and could be catastrophic to a patient who needs immediate IV fluids or drugs. Furthermore, infusion of large amounts of fluid into the joint space could damage to the joint capsule and could lead to septic arthritis if a meticulous sterile technique is not utilized.
Conclusion
Civilian and military first responders, as well as emergency physicians, should be aware of intra-articular IO line placement as a potential complication of IO vascular access. Radiographs of the affected insertion site should be performed to assess IO line placement before removal of the IO needle. Patients who present with intra-articular placement of IO line should be evaluated and followed for the development of septic arthritis.




