


Introduction
Executive functioning (EF) is a broad term encompassing domains such as volition, planning and decision-making, purposive action, self-regulation, and effective performance (Lezak, Howieson, Bigler, & Tranel, Reference Lezak, Howieson, Bigler and Tranel2012). Although a diverse set of brain regions are involved in executive functioning, the frontal lobes are considered to provide the principal neural substrate (e.g., Stuss, Reference Stuss2011; Stuss & Knight, Reference Stuss and Knight2002). Within the frontal lobes, the division between the dorsolateral prefrontal cortex (dlPFC) and the ventromedial prefrontal cortex (vmPFC) is critical in understanding two distinct types of abilities subsumed under the term executive functioning: “metacognitive executive functions” and “emotional/motivational executive functions,” respectively (Ardila, Reference Ardila2008; Stuss, Reference Stuss2011).
Metacognitive executive functions are those which organize and monitor goal-directed behavior. These functions include abilities assessed by traditional clinical and laboratory measures of executive functioning (e.g., planning, response inhibition, working memory) (Ardila, Reference Ardila2008). Various structural models of these metacognitive functions have been proposed in the literature. For example, Latzman and Markon (Reference Latzman and Markon2010) identified a three factor structure (“conceptual flexibility,” “monitoring,” “inhibition”) for scores on the Delis-Kaplan Executive Function System (D-KEFS). This structure is similar to a three-factor model (“shifting,” “updating,” “inhibition”) found using a different set of executive functioning measures (Miyake et al., Reference Miyake, Friedman, Emerson, Witzki, Howerter and Wager2000).
In a lesion study of popular neuropsychological measures of these “metacognitive” types of executive functions (e.g., Wisconsin Card Sorting Test, Controlled Oral Word Association Test), a relationship between deficits in these functions and damage to the dlPFC and anterior cingulate was found (Gläscher et al., Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012). This is consistent with a large body of literature that has suggested a relationship between cognitive components of executive functioning and the dlPFC and anterior cingulate (for reviews, see Lezak et al., Reference Lezak, Howieson, Bigler and Tranel2012; Stuss & Levine, Reference Stuss and Levine2002). Moreover, in a meta-analysis of functional neuroimaging studies of cognitive measures of executive functioning, the dlPFC and anterior cingulate were found to be the “critical nodes” activated in both healthy adults and patients with schizophrenia (Minzenberg, Laird, Thelen, Carter, & Glahn, Reference Minzenberg, Laird, Thelen, Carter and Glahn2009).
Emotional and motivational executive functions involve “coordinating cognition and emotion” (Ardila, Reference Ardila2008). These functions are related to the vmPFC (Lezak et al., Reference Lezak, Howieson, Bigler and Tranel2012; Stuss et al., 2002). Although patients with vmPFC damage maintain their formal knowledge of social norms—that is, they can “talk a good game” and give appropriate verbal responses to social hypotheticals (e.g., Beer, John, Scabini, & Knight, Reference Beer, John, Scabini and Knight2006; Saver & Damasio Reference Saver and Damasio1991), they fail to process emotional information normally, and as a consequence have impairments in affective and social decision-making, that is, implementing social knowledge in the real world, in real time, and “on line” (Bechara, Reference Bechara2004; Beer et al., Reference Beer, John, Scabini and Knight2006). As a result of vmPFC damage, patients experience significant changes in emotional (e.g., blunted affect) and social (e.g., increases in inappropriate social behavior) aspects of personality functioning (Barrash, Tranel, & Anderson, Reference Barrash, Tranel and Anderson2000; Barrash et al., Reference Barrash, Asp, Markon, Manzel, Anderson and Tranel2011). Atrophy of the vmPFC has been linked to increases in disinhibited behavior that occur in patients with frontotemporal dementia (Hornberger, Geng, & Hodges, Reference Hornberger, Geng and Hodges2011; Massimo et al., Reference Massimo, Powers, Moore, Vesely, Avants, Gee and Grossman2009).
VmPFC patients make decisions that show “myopia for the future” (Bechara, Damasio, & Damasio, Reference Bechara, Damasio and Damasio2000), and the patients manifest an inability to forego choices with immediate positive consequences (and negative long-term consequences) for those with better long-term outcomes (but less appealing immediate consequences). This decision-making impairment is well quantified by the Iowa Gambling Task (IGT), a value-based decision-making task that factors together immediate and delayed rewards and punishments, along with a degree of uncertainty. The association of vmPFC damage and impaired IGT performance was recently confirmed in a large-scale analysis of neurological patients with focal brain lesions (Gläscher et al., Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012). According to the somatic marker hypothesis (Damasio, Reference Damasio1994), the role of the vmPFC in executive functioning can be explained through its role as a critical region for processing emotional information important for many aspects of decision-making, especially in social contexts and under conditions of uncertainty, ambiguity, and conflict (Bechara et al., Reference Bechara, Damasio and Damasio2000). Functional neuroimaging approaches using the IGT in healthy participants have also supported a role for the vmPFC in value-based decision-making (Li, Lu, D'Argembeau, Ng, & Bechara, Reference Li, Lu, D'Argembeau, Ng and Bechara2010; Northoff et al., Reference Northoff, Grimm, Boeker, Schmidt, Bermpohl, Heinzel and Boesiger2006). Similar findings have been obtained with a variety of reinforcement and reward-learning paradigms in the functional neuroimaging literature (see reviews by O'Doherty, Reference O'Doherty2004; Wallis, Reference Wallis2007).
The ability to pursue goal-directed behavior depends on intact knowledge of one's cognitive and behavioral abilities. Therefore, insight can also be considered to be an aspect of executive functioning (cf., Tranel, Anderson, & Benton, Reference Tranel, Anderson and Benton1994). VmPFC damage is associated with a lack of insight into cognitive and behavior changes (Barrash et al., Reference Barrash, Tranel and Anderson2000). In one social interaction task, vmPFC patients made inappropriate self-disclosures to strangers, but lacked insight into their inappropriate behavior (Beer et al., Reference Beer, John, Scabini and Knight2006). Atrophy of the vmPFC is associated with impaired insight regarding cognitive deficits that occur in neurodegenerative diseases (Rosen et al., Reference Rosen, Alcantar, Rothlind, Sturm, Kramer, Weiner and Miller2010), including in patients with frontotemporal dementia (Massimo et al., Reference Massimo, Libon, Chandrasekaran, Dreyfuss, McMillan, Rascovsky and Grossman2013). Insight, and self-awareness more generally, has been consistently linked to the prefrontal cortices, especially the medial sector, in functional imaging work (e.g., Kelley et al., Reference Kelley, Macrae, Wyland, Caglar, Inati and Heatherton2002; see Philippi, Duff, Denburg, Tranel, & Rudrauf, Reference Philippi, Duff, Denburg, Tranel and Rudrauf2012, for a lesion study confirming these findings).
Some aspects of executive functioning rely on both the dlPFC and vmPFC. For example, apathy, which includes symptoms of diminished interest and motivation, is associated with atrophy in both the dlPFC and vmPFC in patients with amyotrophic lateral sclerosis (Tsujimoto et al., Reference Tsujimoto, Senda, Ishihara, Niimi, Kawai, Atsuta and Sobue2011) and frontotemporal dementia (Zamboni, Huey, Krueger, Nichelli, & Grafman, Reference Zamboni, Huey, Krueger, Nichelli and Grafman2008). While impairments in both cognitive empathy (the ability to take the perspective of another person) and emotional empathy (the ability to personally experience emotions related to another person's circumstances) are associated with vmPFC damage, dlPFC damage has also been associated with impaired cognitive empathy (Eslinger, Reference Eslinger1998; Eslinger, Moore, Anderson, & Grossman, Reference Eslinger, Moore, Anderson and Grossman2011).
It should be noted that while the dlPFC and vmPFC are critical regions for a variety of executive abilities, other brain regions clearly play a role in executive functioning. For example, the anterior temporal lobes have been liked to both inhibition (Hornberger et al., Reference Hornberger, Geng and Hodges2011) and empathy (Eslinger et al., Reference Eslinger, Moore, Anderson and Grossman2011). Regions in the parietal lobe, including the superior parietal lobule and intraparietal sulcus, have been related to cognitive components of executive functioning (Collette et al., Reference Collette, Van der Linden, Laureys, Delfiore, Degueldre, Luxen and Salmon2005; Koenigs, Barbey, Postle, & Grafman, Reference Koenigs, Barbey, Postle and Grafman2009).
In the current study, we aimed to explore the neural basis of cognitive, social/emotional, and insight components of executive functioning by using voxel-based lesion-symptom mapping (VLSM) in a sample of patients with focal brain damage. This study represents a replication and extension of a recent VLSM study by Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012), using a different and expanded set of EF tests (those from the EXAMINER battery, see below). We sought to replicate findings from Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012) involving cognitive measures of executive functioning and value-based decision-making, and to extend the analysis to include measures of social/emotional functioning and insight. We hypothesized that cognitive EF measures would primarily be associated with dlPFC and anterior cingulate, while social/emotional and insight EF measures would primarily be associated with vmPFC. This study took place as part of the Executive Abilities: Measures and Instruments for Neurobehavior Evaluation and Research (EXAMINER) project, which aimed to develop and validate a new omnibus measure of executive functioning which could be used in clinical research across a range of ages and clinical diagnoses (Kramer, 2011; www.examiner.ucsf.edu). Extensive data regarding the reliability (e.g., test–retest, interrater, internal consistency) and validity (e.g., convergent, discriminant) of the EXAMINER tests can be found in the EXAMINER manual. In general, the available psychometric evidence supports the use of the EXAMINER as a measure of executive functioning.
Methods
Participants
Neurological patients with focal brain lesions (n = 62) were recruited from the Iowa Neurological Patient Registry in the Division of Behavioral Neurology and Cognitive Neuroscience at the University of Iowa. These patients all had stable, focal brain lesions due to subarachnoid hemorrhage (n = 7), surgical intervention (n = 20), ischemic stroke (n = 29), encephalitis (n = 2), traumatic brain injury (n = 3), and intracerebral hemorrhage (n = 1). The majority of patients (n = 37) had focal damage to the prefrontal cortex: 23 had damage which included regions of the ventromedial prefrontal cortex (vmPFC) and 14 had damage which included regions of the dorsolateral prefrontal cortex (dlPFC). In some cases, the area of damage extended outside of the vmPFC or dlPFC. The remainder (n = 25) had damage to other brain regions outside the frontal lobes. All patients were tested in the chronic epoch of recovery, 3 or more months after lesion onset, and the neuropsychological and neuroimaging data were generally collected contemporaneously. The average age at time of testing for all participants in this study was 59 years (SD = 10.5; range: 37 to 82 years). The average level of education of the sample was 14 years (SD = 2.6; range, 12–20 years). A total of 40% of the sample was female (n = 25). Most of the participants (58) were right-handed; 3 were left-handed, and 1 had mixed-handedness. The sample was 90% European-American (white). For most of the patients, collaterals (e.g., spouses or adult children) were available to complete informant questionnaires about the patient's behavior. The sample sizes for each individual measure can be found in Figure 1. A subset of these patients (n = 27) were also participants in the study by Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012). The current study was approved by the University of Iowa Institutional Review Board.
Measures
All participants were administered the entire EXAMINER battery by a researcher in the Department of Neurology at the University of Iowa Hospitals and Clinics. The EXAMINER battery is comprised by both traditional cognitive tests of executive functioning (e.g., verbal fluency) and measures designed to assess social/emotional and metacognitive aspects of executive functioning (e.g., insight) (Kramer, 2011). These measures are listed in Table 1, and are briefly described below. A full description of the tasks can be found in the EXAMINER manual (Kramer, 2011). Some measures are completed by an informant who knows the patient; for these measures, data were available for only a subset of patients (see Figures 1 and 2 for the sample sizes for individual measures).
Table 1 EXAMINER tasks by executive domain
*Tests included in these composite measures are listed in the Methods section under Cognitive Measures.
FrSBe = Frontal Systems Behavior Scale. IRI = Interpersonal Reactivity Index.

Fig. 1 Statistical power maps for the measures included in this study. Red and yellow identify areas with sufficient lesion coverage to detect statistical significance at p < .05. Red is used to indicate areas in which we had sufficient power to detect a finding but did not obtain a significant result; yellow is used to indicate areas in which we had sufficient power and did obtain a significant result. Both green and gray identify areas without sufficient power. Green is used to indicate areas in which we did not have sufficient power to detect a finding but did obtain a significant result; gray is used to indicate areas in which we did not have sufficient power and did not obtain a significant result. (A) Cognitive Measures. (B) Social/Emotional Measures. (C) Insight Measures.

Fig 1 continued
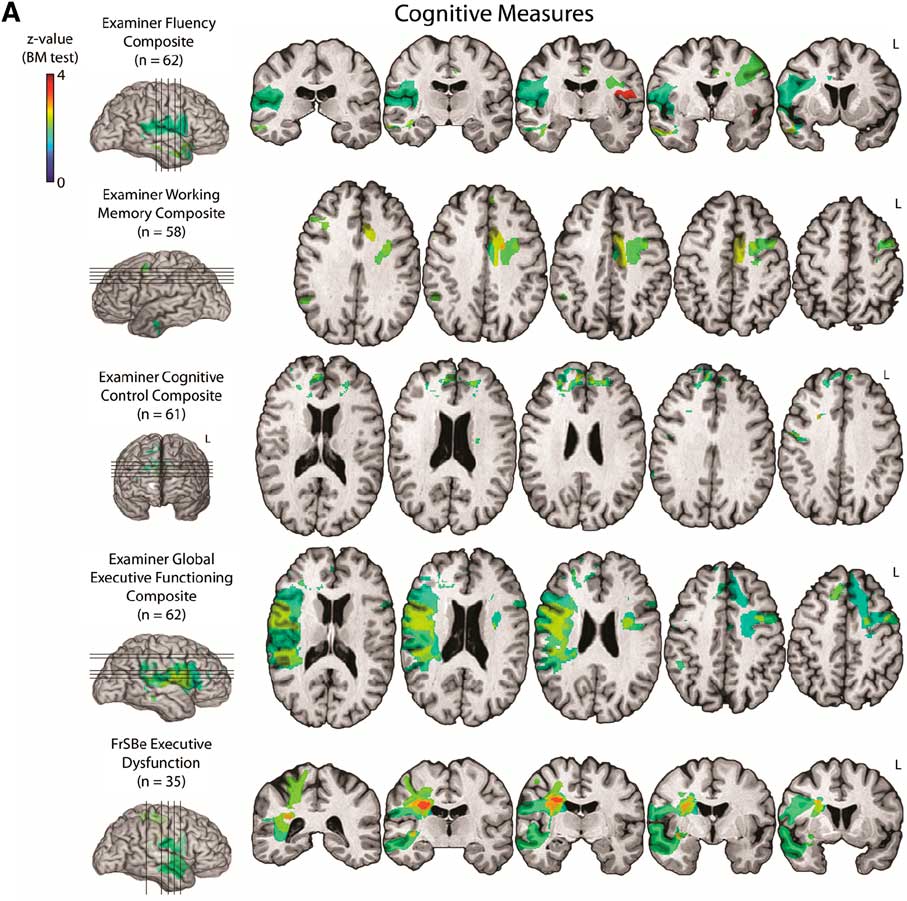
Fig. 2 Results of the VLSM for the various measures included in this study are displayed on a template brain according to standard radiological convention (left hemisphere on the right). Statistical significance (p < .05) was determined by the Brunner-Munzel test. Significant findings are identified by colors corresponding to the Z-score bar to the right of each score. (A) Cognitive Measures. (B) Social/Emotional Measures. (C) Insight Measures.

Fig 2 continued
Cognitive measures
The cognitive tests of the EXAMINER battery are refinements of popular clinical and experimental tasks of executive functioning. Scores from various tests are best represented by a three-factor model of cognitive executive functioning, made up of (1) verbal fluency (scores from category and phonemic fluency tasks), (2) working memory (scores from N-back and Dot Counting tasks), and (3) cognitive control (scores from anti-saccade, flanker, set shifting tasks, and failures of inhibition across several tasks). In addition, a bifactor analysis found support for a global factor of general executive functioning comprised of scores from of all the cognitive measures (Kramer, 2011). Based on these models, composite scores (viz., verbal fluency, working memory, cognitive control, and general executive functioning) were generated using a computer scoring program (Kramer, 2011; see Table 1).
As part of the EXAMINER-related assessment of the patients, the Frontal Systems Behavior Scale (FrSBe) was administered. This informant-report measure of a participant's behavior contains three subscales (apathy, disinhibition, executive dysfunction) (Grace & Malloy, Reference Grace and Malloy2001). The executive dysfunction subscale, which includes items assessing behaviors such as perseveration, disorganization, and poor judgment, can be considered an index of the patient's real-world cognitive executive functioning, and we included that measure under our Cognitive Measures domain. The apathy and disinhibition FrSBe subscales were included under Social/Emotional measures, as below. For all FrSBe scales, the standardized t scores provided in the manual were used in the VLSM analyses.
Social/emotional measures
The EXAMINER battery contains measures of social and emotional components of executive functioning. The Unstructured Task measures strategic planning and value-based decision-making, based on the Six-Elements Test (Shallice & Burgess, Reference Shallice and Burgess1991). For the purposes of the VLSM analysis, this score was converted to an age-adjusted Z-score (Van Breukelen & Vlaeyen, Reference Van Breukelen and Vlaeyen2005). The Social Norms Questionnaire is a measure of social knowledge in which the participant must decide whether or not a behavior is socially appropriate. The score used in the VLSM analysis was a Z-score based on the performance of neurologically healthy adults (see below). As part of the EXAMINER assessment, several other measures of a participant's social and emotional functioning were administered to informants who knew the participant well. The perspective-taking and empathic concern subscales of the Interpersonal Reactivity Index (IRI; Davis, Reference Davis1983) were used as measures of cognitive and emotional empathy, respectively. The Revised Self-Monitoring Scale (RSMS; Lennox & Wolfe, Reference Lennox and Wolfe1984) measures a participant's ability to perceive the effect of their actions on another person and adjust their behavior accordingly. Sex-adjusted Z-scores of the empathy (the two IRI subscales) and self-monitoring scores were used in the VLSM analyses. The FrSBe apathy subscale, which measures a loss of motivation and engagement in activities, and disinhibition subscale, which measures impulsive and socially inappropriate behavior, were considered additional measures of social and emotional functioning.
Insight measures
Measures of insight into cognitive functioning were administered to participants after they completed their first trials of phonemic and category fluency. Participants were asked to evaluate their performance relative to a hypothetical sample of 100 people who are similar to them in age and educational background. Participants were presented with an illustration of a normal distribution which included percentiles and written descriptions of how to interpret them, and asked to identify their level of performance. The score used in the VLSM analysis was a sum of two Z-scores reflecting the difference between the patient's actual and estimated performance for both category and letter fluency. The Revised Self-Monitoring Scale mentioned previously as an informant-report measure was also used as a self-report measure of a participant's behavior. A difference score comparing the patient's self-report to the informant's report was used in the VLSM analysis.
Data Analysis
Neuropsychological data
The scores used in each individual analysis were coded so that lower scores would be associated with greater dysfunction and/or impairment. For insight, greater dysfunction/impairment was conceptualized as a participant overestimating his or her cognitive or self-monitoring abilities. Before using the EXAMINER composite scores, a confirmatory factor analysis (CFA) of the cognitive tests in the EXAMINER battery was performed to determine whether the factor structure identified in the EXAMINER manual applied to our dataset from patients with focal brain damage. As the verbal fluency composite is composed of two trials of letter fluency and two trials of category fluency, correlated residuals of the same type of trial were included in the CFA. The bifactor model allowing tests to load on both a global composite of executive functioning and specific factors was not tested due to our small sample size for that type of analysis.
To calculate Z-scores for many of the neuropsychological measures, we used a normative comparison group based upon a larger subset of neurologically healthy adults who completed the EXAMINER battery at multiple study sites (Kramer, 2011).
Statistical lesion analysis
Lesions were analyzed from MRI scans (or, in a few cases where MRI was contraindicated, from CT scans). Individual lesions were manually traced and transferred onto a standardized brain using MAP-3; therefore, automatic image registration was not necessary (Fiez, Damasio, & Grabowski, Reference Fiez, Damasio and Grabowski2000; Frank, Damasio, & Grabowski, Reference Frank, Damasio and Grabowski1997). This study used a non-parametric (Rorden, Karnath, & Bonilha, Reference Rorden, Karnath and Bonilha2007) voxel-based lesion symptom mapping (VLSM) approach (Bates et al., Reference Bates, Wilson, Saygin, Dick, Sereno, Knight and Dronkers2003) to identify significant lesion-deficit relationships. In contrast to other lesion approaches, which often require continuous behavioral data to be dichotomized into “impaired” or “unimpaired” categories, or predefined anatomical groups to be created for comparison (e.g., vmPFC patients vs. nonfrontal patients), a VLSM approach allows for the analysis of continuous behavioral data across the voxels of the brain. In this way, it is similar to mass-univariate approaches to analyzing functional neuroimaging data (e.g., Friston, Ashburner, Kiebel, Nichols, & Penny, 2007). Comparisons between voxels were performed using the Brunner-Munzel test (Brunner & Munzel, Reference Brunner and Munzel2000) in MRIcron using the “Nonparametric Mapping” function (Rorden et al., Reference Rorden, Karnath and Bonilha2007). At each voxel, this test compares the scores of patients with and without a lesion. Significant voxels (p < .05) are those in which patients with damage at that voxel scored significantly lower than patients without damage at that voxel, using the BM statistic. All brain voxels were included in the analysis. Statistical power maps were computed in the “Nonparametric Mapping” function, using the nonparametric Wilcoxon–Mann–Whitney probability to estimate a power threshold.
Results
Power Maps
Power maps for each test score included in the study are depicted in Figure 1. Both red and yellow areas are regions in which we had sufficient power to detect a finding. Red is used to indicate areas in which we had sufficient power to detect a finding but did not obtain a significant result; yellow is used to indicate areas in which we had sufficient power and did obtain a significant result. In general, power was sufficient in most regions of the brain, including the prefrontal cortex.
Cognitive Measures
The three-factor model of cognitive measures of executive functioning identified in the EXAMINER manual fit adequately in the present sample of patients with focal brain damage (CFA = 0.932; TLI = 0.904; RMSEA = 0.072; SRMR = 0.087). Therefore, the VLSM was carried out using the three composite scores generated by that model, namely, verbal fluency, working memory, and cognitive control (Figure 2A). The fluency composite was related to damage in the right dorsolateral region and the right superior temporal and middle temporal regions, as well as to left insula damage. The working memory composite was related to both frontal (i.e., the bilateral dlPFC and left mesial frontal cortex) and nonfrontal (i.e., left anterior temporal lobe and right angular gyrus) damage. The cognitive control composite was related to bilateral superior frontal damage, damage to the right anterior cingulate, and to a small area of right dlPFC damage. The general, global executive functioning composite was associated with damage to the bilateral dlPFC, bilateral superior mesial frontal region, right supramarginal gyrus, and right superior and middle temporal gyri. The FrSBe executive dysfunction score was predominately associated with right-hemisphere lesions in gray matter and underlying white matter of the dorsolateral cortex, anterior temporal lobe, and superior parietal lobule.
Social/Emotional Measures
VLSM results for the social/emotional measures are displayed in Figure 2B. The Unstructured Task was predominately associated with left-hemisphere lesions, including damage to the left vmPFC, left superior frontal gyrus, and left superior parietal lobule. Lower scores on the EXAMINER Social Norms Questionnaire were associated with bilateral superior frontal cortex damage and mesial temporal lobe damage. Emotional empathy (IRI-Empathic Concern) was predominately associated with right hemisphere damage (including dorsolateral regions and underlying white matter and the cingulate) and small areas of the bilateral orbitofrontal damage. Cognitive empathy (IRI-Perspective Taking) was most strongly associated with bilateral anterior temporal lobe damage, bilateral vmPFC and orbitofrontal damage, and damage to white matter underlying the right inferior parietal lobule. Poor self-monitoring (Revised Self-Monitoring Scale) was associated with damage to the bilateral vmPFC/orbitofrontal region, right dlPFC, and right anterior temporal lobe. The FrSBe apathy score was associated with bilateral vmPFC/orbitofrontal damage and right dlPFC and superior parietal lobule damage. The FrSBE disinhibition score was associated with bilateral vmPFC/orbitofrontal damage, as well as right anterior temporal lobe damage.
Insight Measures
VLSM results for the insight measures are displayed in Figure 2C. Overestimation of cognitive performance on verbal fluency measures was significantly associated with damage to the right parahippocampal gyrus and inferotemporal region, as well as bilateral areas of the orbitofrontal cortex and superior mesial frontal region. Overestimation of self-monitoring abilities was associated with left vmPFC/orbitofrontal damage and right insula, dorsolateral cortex, and anterior temporal lobe damage.
Discussion
Results from the VLSM analyses of the EXAMINER cognitive measures, which generally showed a relationship between dorsolateral prefrontal damage and lower test performance, were largely consistent with our hypothesis, and they provide an important replication of the findings reported by Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012) regarding the relationship between cognitive measures of executive functioning and both dlPFC and anterior cingulate damage. There are some differences in the results of the two studies regarding cognitive measures, which appear to be largely due to differences in methodology. For example, Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012) used a measure of letter fluency while the current study used a composite measure of both letter and category fluency. Given that previous research has shown that lesions in the right dlPFC are significantly associated with impairments in semantic fluency, but not letter fluency (Stuss et al., Reference Stuss, Alexander, Hamer, Palumbo, Dempster, Binns and Izukawa1998), the inclusion of semantic fluency may explain why our findings for verbal fluency differed somewhat from those reported by Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012). The current study is also consistent with another recent lesion study that showed a relationship between executive functioning and the dorsolateral prefrontal regions (Barbey, Colom, & Grafman, Reference Barbey, Colom and Grafman2012).
Of interest, an informant report measure of primarily cognitive aspects of executive functioning (FrSBe Executive Dysfunction) overlapped with the EXAMINER cognitive measures in its relationship to damage in regions such as the dlPFC. Previous studies showing significant correlations between the FrSBe Executive Dysfunction subscale and traditional clinical measures of executive functioning have suggested both types of measures relate to shared neural substrates (e.g., Chiaravalloti & DeLuca, Reference Chiaravalloti and DeLuca2003). The current study supports this idea.
The Unstructured Task, a measure that involves both planning and value-based decision-making, was most strongly associated with damage in the vmPFC. This test is a modification of the Six-Element Test (Shallice & Burgess, Reference Shallice and Burgess1991), previously shown to be sensitive to vmPFC damage (Levine et al., Reference Levine, Stuss, Milberg, Alexander, Schwartz and Macdonald1998). The current study provides additional evidence for the conclusion made by Gläscher et al. (Reference Gläscher, Adolphs, Damasio, Bechara, Rudrauf, Calamia and Tranel2012) that the vmPFC is critical for value-based decision-making. Another important finding was that damage to the vmPFC was not associated with impairments in off-line, verbally based social knowledge and reasoning (the Social Norms Questionnaire), which is consistent with previous studies (e.g., Beer et al., Reference Beer, John, Scabini and Knight2006; Saver & Damasio, Reference Saver and Damasio1991). Of interest, damage to the superior mesial prefrontal cortex was found to be associated with lower scores on this measure, which could suggest a role for the superior mesial frontal sector in storing declarative types of social knowledge. Previous fMRI studies have suggested that this region plays a role in processing social rule violations (e.g., Berthoz, Armony, Blair, & Dolan, Reference Berthoz, Armony, Blair and Dolan2002; Fiddick, Spampinato, & Grafman, Reference Fiddick, Spampinato and Grafman2005).
The current study also extends previous findings linking cognitive empathy to the vmPFC (Ames, Jenkins, Banaji, & Mitchell, Reference Ames, Jenkins, Banaji and Mitchell2008; Shamay-Tsoory, Aharon-Peretz, & Perry, Reference Shamay-Tsoory, Aharon-Peretz and Perry2009). In contrast, although emotional empathy has been shown to be related to vmPFC damage in previous studies (e.g., Shamay-Tsoory, Tomer, Goldsher, Berger, & Aharon-Peretz, Reference Shamay-Tsoory, Tomer, Goldsher, Berger and Aharon-Peretz2004), such a relationship was not found in the current study. However, outside of the frontal lobe, the predominately right-lateralized results for emotional empathy are consistent with literature showing greater deficits in empathy with right hemisphere lesions (e.g., Shamay-Tsorry, Tomer, Berger, & Aharon-Peretz, Reference Shamay-Tsoory, Tomer, Berger and Aharon-Peretz2003). This may be due to impairments in emotion recognition following right hemisphere damage (e.g., Adolphs, Damasio, Tranel, & Damasio, Reference Adolphs, Damasio, Tranel and Damasio1996). The relationship found between damage in non-frontal right hemisphere regions and self-monitoring may also be related to impairments in emotion recognition. In contrast, the relationship between vmPFC damage and self-monitoring may be related to deficits in other aspects of emotional processing (Beer et al., Reference Beer, John, Scabini and Knight2006).
Also consistent with previous work (Zamboni et al., Reference Zamboni, Huey, Krueger, Nichelli and Grafman2008), we found a relationship between apathy and both vmPFC and dlPFC damage. It has been suggested that apathy can result from either deficits in planning (i.e., dlPFC-type dysfunction) or deficits in emotional processing (i.e., vmPFC-type dysfunction) (Levy & Dubois, Reference Levy and Dubois2006). Our study also found relationships between disinhibition and both the vmPFC and anterior temporal lobe that parallel findings found for disinhibition and atrophy in these regions in patients with frontotemporal dementia (Hornberger et al., Reference Hornberger, Geng and Hodges2011). A previous lesion study of the FrSBe showed that the measure could distinguish between frontal and non-frontal brain damage (Grace, Stout, & Malloy, Reference Grace, Stout and Malloy1999). The current study extends those findings and provides additional evidence in support of the FrSBe as a measure of executive functioning.
Informants of vmPFC patients have frequently described them as lacking insight into the cognitive and behavior changes they have experienced as a result of brain damage (e.g., Barrash et al., Reference Barrash, Tranel and Anderson2000). The current study provides additional evidence to support that idea. Both poor cognitive insight (i.e., an overestimation of verbal fluency performance) and poor behavioral insight (i.e., an overestimation of self-monitoring abilities) were associated with vmPFC damage. A lack of behavioral insight was also related to damage in the right insula, a region that has been linked to self-awareness (Craig, Reference Craig2011; but see Damasio, Damasio, & Tranel, Reference Damasio, Damasio and Tranel2013, and Philippi, Felinstein, et al., Reference Philippi, Feinstein, Khalsa, Damasio, Tranel, Landini and Rudrauf2012, for other perspectives on this issue).
Although the sample size used in this study is comparable to that of many other published VLSM analyses (e.g., Arévalo, Baldo, & Dronkers, Reference Arévalo, Baldo and Dronkers2012; Saygin, Reference Saygin2007), the distribution of lesions was such that the majority of patients had damage to the PFC. This was done intentionally, so as to increase power to detect significant relationships between PFC damage and executive functioning. Also, to maximize our ability to detect relationships throughout the brain, all lesioned voxels were analyzed. We chose this approach to maximize the utility of our data, given the rarity of well-studied neurological patients with focal brain lesions. As a result of this approach, while findings in the PFC are based on multiple patients with damage in that region, significant findings in regions outside of the PFC may be based on damage that occurred in only one or two patients. Therefore, we wish to highlight the need to replicate our findings regarding non-PFC regions in other studies with larger samples. Nonetheless, most of our results have a convincing parallel with previous work, and make good sense in the context of what is generally known about the functions of the frontal lobes (e.g., Lezak et al., Reference Lezak, Howieson, Bigler and Tranel2012).
Two additional limitations of our study should be noted. First, due to our sample size, we were unable to examine the effects of individual differences such as gender on our results. Second, while the cognitive components of executive functioning was measured with multiple test scores organized into factors, the social/emotional components were measured with one or two individual test scores. A more comprehensive set of social/emotional measures could be used in future studies to shore up the reliability and validity of measuring those constructs.
In summary, in support of neuroanatomical theories of the role of the PFC in executive functioning (Ardila, Reference Ardila2008; Stuss, Reference Stuss2011), the results of our VLSM analyses showed that lesions to the vmPFC were related to impairments in various social and emotional components of executive functioning, whereas lesions to the dlPFC and anterior cingulate were related to impairments in cognitive components of executive functioning. Our results also provide additional evidence for the validity of the EXAMINER as a measure of executive functioning.
Acknowledgments
This work was supported by NINDS P50 NS19632 (DT), NINDS HHS99271200623661 (DT), and a grant by the German Ministry of Education and Research (01GQ1006; JG). The authors acknowledge that the information contained within this manuscript and the manuscript itself has never before been published in print or electronically. None of the authors has a conflict of interest. Heather Robinson and Matthew Calamia contributed equally to this work.





