



With the highest rate of childhood poverty among all economically developed nations, nearly one in four children in the United States are born into poverty (National Center for Children in Poverty, 2018). Tragically, detriments of growing up in poverty are not limited to childhood: the long arm of childhood poverty reaches across multiple developmental outcomes throughout life. However, while previous research has shown that growing up in poverty predicts adult behavioral problems, few studies have examined childhood poverty and developmental trajectories from childhood through adulthood. In addition, the few prior studies on developmental trajectories following childhood poverty have been limited to behavioral problem reports. We address these limitations by examining developmental trajectories of psychological well-being as a function of childhood poverty. A second contribution of this study is the inclusion of multimethodological indicators of psychological well-being development that supplement information on behavioral problems. We add to the childhood disadvantage literature information on developmental trajectories by including measures of learned helplessness and chronic physiological stress.
Looking beyond the main effects of poverty, few investigators have explored underlying mechanisms that may account for the associations between early childhood poverty and psychological well-being over time. One of the unique and defining qualities of poverty is exposure to a plethora of suboptimal physical (e.g., substandard housing) and psychosocial (e.g., family turmoil) risk factors (Evans, Reference Evans2004; Evans & Kim, Reference Evans and Kim2010; McEwen & McEwen, Reference McEwen and McEwen2017; Repetti, Taylor, & Seeman, Reference Repetti, Taylor and Seeman2002; Taylor, Repetti, & Seeman, Reference Taylor, Repetti and Seeman1997). Therefore, a third contribution of the present study is analysis of whether the hypothesized, adverse developmental trajectories of childhood poverty can be explained, to some degree, by changes in cumulative risk exposure over time. Finally, we conduct additional sensitivity analyses to supplement our primary hypothesis testing by examining some alternative, candidate mediating processes that may also account for some of the expected adverse trajectories of childhood poverty.
Poverty shows consistent, positive associations with behavioral problems during childhood (Bradley & Corwyn, Reference Bradley and Corwyn2002; Grant et al., Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003; McLoyd, Reference McLoyd1998; Wadsworth, Evans, Grant, Carter, & Duffy, Reference Wadsworth, Evans, Grant, Carter, Duffy and Cicchetti D2016). Although the literature on the psychological distress sequelae of childhood poverty is abundant, longitudinal studies ranging from early in life through adulthood are infrequent. Nonetheless, longitudinal studies indicate that as early as three years of age, behavioral problems among disadvantaged children are elevated, and increase faster through adolescence, relative to their middle-class peers (Bolger, Patterson, Thompson, & Kupersmidt, Reference Bolger, Patterson, Thompson and Kupersmidt1995; Bradley & Corwyn, Reference Bradley, Corwyn, Bornstein and Bradley2003; Dubow & Ippolito, Reference Dubow and Ippolito1994; Evans & Cassells, Reference Evans and Cassells2014; Keiley, Bates, Dodge, & Pettit, Reference Keiley, Bates, Dodge and Pettit2000; McLeod & Shanahan, Reference McLeod and Shanahan1996; Melchior et al., Reference Melchior, Chastang, Walburg, Arsenault, Galera and Fombonne2010; Sacker, Schoon, & Bartley, Reference Sacker, Schoon and Bartley2002; Slopen, Fitzmaurice, Williams, & Gilman, Reference Slopen, Fitzmaurice, Williams and Gilman2010; Stroschein, Reference Stroschein2005; Votruba-Drzal, Reference Votruba-Drzal2006; Wadsworth & Achenbach, Reference Wadsworth and Achenbach2005).
While these previous results present evidence for the psychological well-being implications of childhood disadvantage throughout childhood into adolescence, only a few studies show the psychological residue of early poverty persists into adulthood (McLaughlin et al., Reference McLaughlin, Breslau, Green, Lakoma, Sampson, Zaslavsky and Kessler2011; Najman et al., Reference Najman, Hayatbakhsh, Clavarino, Bor, O'Callaghan and Williams2010; Schoon, Sacker, & Bartley, Reference Schoon, Sacker and Bartley2003). Understanding the developmental trajectories of well-being into adulthood is of interest to know what these trends look like; in what form are they manifested; and because longitudinal data can provide insight into the nature of how and when experiences of early disadvantage affect health and well-being. There may also be utility in knowing whether disparities are static or shift over time, suggesting differential effects based on aging as well as duration of exposure.
We extend reliance on surveys and interviews in research on psychological well-being sequelae of early disadvantage with two other methodological assessments. First, we include an overt behavioral indicator of learned helplessness consisting of persistence on challenging tasks and with assessments of allostatic load, an index of chronic physiological stress. Although one of the adverse outcomes of poverty is believed to be a sense of despair and hopelessness, only a handful of empirical studies have evaluated this hypothesis. Low-income preschool children facing a greater array of poverty-related stressors (e.g., residential mobility, unemployment) were less persistent on challenging, geometric puzzles than their peers facing fewer of these poverty-related stressors (Brown, Reference Brown2009). Using a different sample of low-income children, Brown, Seyler, Knorr, Garnett, and Laurenceau (Reference Brown, Seyler, Knorr, Garnett and Laurenceau2016) found that daily fluctuations in these poverty-related stressors were tracked by task persistence at the end of each day over a 10-day period. Finally, 9-year-olds from low- versus middle-income homes were less persistent on challenging geometric puzzles (Evans & English, Reference Evans and English2002) and this continued through age 17 (Evans & Cassells, 2017). In the current study, we examine whether childhood poverty exposure alters the developmental trajectories of learned helplessness from age 9 through 24.
Second, we incorporate another methodological assessment of psychological well-being development by including a measure of chronic physiological stress. Emerging work indicates that a biological residue of early disadvantage begins to accumulate in young organisms and may remain throughout life (Kim, Evans, Chen, Miller, Seeman, Reference Kim, Evans, Chen, Miller, Seeman, Halfon, Lerner and Faustman2018; Miller & Chen, Reference Miller and Chen2013; Seeman, Epel, Gruenwald, Karlamangla, & McEwen, Reference Seeman, Epel, Gruenwald, Karlamangla and McEwen2010). One key mechanism for how childhood poverty gets under the skin to damage physical health may be elevated, chronic physiological stress. Allostatic load as an indicator of chronic physiological stress marks chronic wear and tear on the body caused by the mobilization of resources to meet changing environmental demands. It reflects the degree of co-ordination among multiple physiological response systems as they adapt to environmental demands (Ganzel, Morris, & Wethington, Reference Ganzel, Morris and Wethington2010; McEwen, Reference McEwen1998; Seeman & McEwen, Reference Seeman and McEwen1996). Composite indexes of allostatic load across multiple physiological response systems predict morbidity and mortality better than any singular biomarker of chronic stress (Juster, McEwen, & Lupien, Reference Juster, McEwen and Lupien2010; McEwen, Reference McEwen1998; McEwen & Gianaros, Reference McEwen and Gianaros2010; Seeman, McEwen, Row, & Singer, Reference Seeman, McEwen, Row and Singer2001; Seeman et al., Reference Seeman, Epel, Gruenwald, Karlamangla and McEwen2010). Prior work has found evidence of elevated allostatic load in relation to childhood disadvantage (Brody et al., Reference Brody, Yu, Chen and Kogan2013, Reference Brody, Lei, Chen and Miller2014; Evans & Kim, Reference Evans and Kim2012; Evans & Schamberg, Reference Evans and Schamberg2009; Milligan, Thompson, Vandongen, Beilin, & Burke, Reference Milligan, Thompson, Vandongen, Beilin and Burke1995; Rainisch & Upchurch, Reference Rainisch and Upchurch2013; Worthman & Panter-Brick, Reference Worthman and Panter-Brick2008). What is absent from these few studies on allostatic load and childhood disadvantage are data on developmental trajectories.
Finally, we examined changes in exposure to cumulative risk factors at multiple time points throughout childhood and adolescence to assess whether an individual's trajectory of cumulative risk exposure could explain some of the hypothesized alterations in developmental trajectories emanating from childhood poverty. One of the key and unique signatures of childhood poverty is the confluence of risk exposures as disadvantaged children face a plethora of suboptimal physical conditions such as poor housing quality, ambient toxins, noise, and chaotic surroundings (Evans, Reference Evans2004; Evans & Kim, Reference Evans and Kim2010). Children growing up in poverty are also more likely to confront family turmoil, conflict, separation from caregivers, and multiple forms of instability in their social relationships (Conger & Donnellan, Reference Conger and Donnellan2007; Evans, Reference Evans2004; Evans & Kim, Reference Evans and Kim2010; Grant et al., Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003; Repetti et al., Reference Repetti, Taylor and Seeman2002; Wadsworth et al., Reference Wadsworth, Evans, Grant, Carter, Duffy and Cicchetti D2016). Thus we constructed an index of cumulative risk exposure that assessed both psychosocial risk factors (family turmoil, separation from family, violence) as well as physical environmental risk factors (noise, crowding, suboptimal housing quality) that are well-documented features of childhood disadvantage (Evans, Reference Evans2004; Repetti et al., Reference Repetti, Taylor and Seeman2002; Taylor et al., Reference Taylor, Repetti and Seeman1997). There is also a small amount of evidence that although multiple, singular risk factors covary with disadvantage, particularly striking is the degree of correspondence between poverty and the accumulation of risk exposure (Evans, Reference Evans2004; Evans & Kim, Reference Evans and Kim2010). This is important given the robust finding that exposure to cumulative risk factors far outweighs singular risk exposure in causing adverse developmental outcomes (Evans, Li, & Whipple, Reference Evans, Li and Whipple2013); Kraemer, Lowe, & Kupfer, Reference Kraemer, Lowe and Kupfer2005; Obradovic, Shaffer, & Masten, Reference Obradovic, Shaffer, Masten, Mayes and Lewis2012; Pressman, Klebanov, & Brooks-Gunn, Reference Pressman, Klebanov, Brooks-Gunn, Mayes and Lewis2012; Sameroff, Reference Sameroff, Clarke-Stewart and Dunn J2006. Furthermore, the developmental impacts of cumulative risk exposure are additive, indicating that the number of risk factors encountered rather than their particular composition is what matters. The specific cumulative risk index used herein was constructed to reflect both psychosocial and physical environmental risk exposures within the microsystem because both domains of the proximal environment contribute to children's development (Bronfenbrenner & Evans, Reference Bronfenbrenner and Evans2000; Wachs & Gruen, Reference Wachs and Gruen1982). Moreover, in prior work, this cumulative index of adverse physical and psychosocial exposures accounted for a significant portion of the covariance between childhood poverty and adverse developmental outcomes (Evans & Cassells, Reference Evans and Cassells2014; Evans & English, Reference Evans and English2002; Evans & Kim, Reference Evans and Kim2007, Reference Evans and Kim2012).
We expand our prior work by investigating whether cumulative risk exposure can account for multiple methodological markers of psychological well-being development (i.e., behavior problems, learned helplessness, chronic physiological stress) and do so from age 9 through age 24. Moreover in additional sensitivity analyses, we disaggregate overall cumulative risk into separate domains of physical and psychosocial risk exposure to evaluate their respective contributions to the developmental course following exposure to early poverty. Lastly, we also evaluate two, additional mechanisms – maternal sensitivity and family social cohesion – to examine a broader array of potential underlying, explanatory processes that may provide further insights into how poverty influences psychological well-being over time.
In summary, the primary objectives of this study were: (a) to identify poverty-related developmental trajectories of multimethodological measures of psychological well-being development from childhood to early adulthood, and (b) to examine whether these expected alterations in the course of psychological well-being development from childhood poverty could be explained, in part, by elevated cumulative risk exposure throughout ages 9 to 24. In addition, we conducted several sensitivity analyses to explore the robustness of our findings and to examine in more depth the hypothesized mediating mechanism of cumulative risk exposure as well as some alternative, underlying explanatory psychological processes.
Method
Participants
The study included 341 participants, ages 8 and 9 years old (M = 9.2 years, 49% female; 94% Caucasian) and their families who were recruited for a long-term program on childhood poverty, cumulative risk exposure, and well-being. Follow up data were collected at ages 13, 17, and 24. The families resided in rural areas in the Northeastern United States and were recruited from public schools, Co-Operative Extension, 4-H, and various anti-poverty programs including Headstart, WIC, Food Pantries, and both regional and federal housing assistance programs. Families were informed that the study was about how stress affects child development without specific reference to poverty. Parental informed consent and child assent were obtained at each wave until the participant reached 18 years of age, at which point informed participant consent was obtained.
Low-income families were over-sampled given the objective of this childhood poverty research program with approximately 45% of the sample from households at or below the federal poverty threshold of 1.0 income-to-needs. Income-to-needs is an annually adjusted per capita poverty index based upon the number of children and adults in the household. The other half of the sample was 2–4 times the federal poverty line, the income level of most American families. The mean income to needs ratio of the sample at Wave 1 was (M = 1.67, SD = 1.10). Among the parents of the children at this initial Wave, 7% reported high school dropout, 12% graduated from college, and 42% of 9-year-olds were living with a single parent. Income to needs was calculated at the time of recruitment (Wave 1). Utilizing a personally informed calendar (e.g., maternal birthdate, children's birthdates, important family holidays, major family transitions) the interviewer and the child's mother worked backwards in time from Wave 1 to the target child's birth to estimate exposure to poverty in 6-month blocks. The child's mother was queried about any changes in financial support (e.g., job change, entry or exit of maternal partner) in relation to the current (i.e., age 9) household income. When a change in finances occurred, she was asked about changes in the magnitude of income. Precise dollar figures were not queried, instead we ascertained whether income went up or down and whether this was a typical yearly increase or a larger raise or with parallel probes for income loss.
Procedure
All data were collected with a standardized protocol in the participant's residence by two experimenters working independently with the child and the child's mother until Wave 4 when only the participant provided data.
Measures
Internalizing and externalizing
Internalizing and externalizing symptoms were collected at each wave. In Wave 1 the primary caregiver, and in Waves 2–4 the participant, rated whether specific behavioral symptoms described the participant (0 = not true – 2 very true). Internalizing symptoms included measures of depression (e.g., “I feel lonely”) and anxiety (e.g., “I worry a lot”), while externalizing symptoms included the assessment of behavioral conduct problems (e.g., “I get into many fights”; “I am too impatient”) (Achenbach, Reference Achenbach1991; Achenbach & Rescorla, Reference Achenbach and Rescorla2003; Rutter, Tizard, & Whitmore, Reference Rutter, Tizard and Whitmore1970). These standardized measures of psychological well-being development have been widely used across heterogenous, sociodemographic samples with excellent psychometric properties. Indices of internal consistency (α) for these two subscales ranged from .64 to .91 across the four waves of data collection herein.
Learned helplessness
Helplessness was measured with a standard behavioral protocol at each wave consisting of age-appropriate puzzles (age 9: tracing lines connecting different animals without lifting the pencil or retracing over any line; age 13: reproducing with plastic pieces an illustration of a tangram; age 17: tracing over abstract, geometric line drawings without lifting pencil or retracing over any line; age 24: rearrange cars on a plastic base by slotting them into different spaces so that the target car could move from the starting point to the exit). Following a practice puzzle with feedback to ensure task comprehension, the participant was given a similar initial puzzle that, unbeknownst to her/him, was unsolvable. The participant was instructed to continue working on the puzzle until solved or until s/he felt unable to do so at which point s/he could move on to a second puzzle. The participant was informed that once they had moved on to the second puzzle, they could not return to the first one. All participants solved the second puzzle and were assured that the initial puzzle was difficult, and most persons could not solve it. Because the total amount of time allotted to solve the two puzzles varied across waves (10–15 min), the proportion of available time spent persisting on the initial puzzle was the index of learned helplessness. This helplessness protocol is associated with beliefs in personal control and mastery, experimental manipulations of control, as well as chronic exposure to uncontrollable stressors (Cohen, Reference Cohen1980; Evans & Stecker, Reference Evans and Stecker2004; Glass & Singer, Reference Glass and Singer1972).
Allostatic load
Allostatic load is a composite index of chronic physiological stress consisting of cardiovascular, neuroendocrine, and metabolic biomarkers of bodily responses to chronic environmental demands. Resting diastolic and systolic blood pressure were measured with an automated blood pressure monitor (Dinamap Pro-100) while seated at rest and reading in a quiet room in the home with only one experimenter present. The means of readings 2–7 were incorporated into the allostatic load composite (Kamarck et al., Reference Kamarck, Jennings, Debski, Glicksman-Weis, Johnson, Eddy and Manuck1992; Krantz & Falconer, Reference Krantz, Falconer, Cohen, Kessler and Gordon1995). Overnight urinary epinephrine and norepinephrine (Riggin & Kissinger, Reference Riggin and Kissinger1977) and cortisol (Contreras, Hane, & Tyrrell, Reference Contreras, Hane and Tyrrell1986) with a creatinine control were analyzed. All voids from bedtime to morning were collected at home, kept on dry ice, and then in the morning immediately transferred and stored at −80° C until assay. Body mass index (BMI) (kg/m2) was assessed at each wave at home by the experimenter. For each biomarker at each wave, participants in the upper quartile of the distribution were scored a 1 and values below the upper quartile scored as 0. Allostatic load was the sum of these six binary values (0–6).
Cumulative risk
Cumulative risk exposure was calculated by exposure to three psychosocial (family turmoil, separation from family, exposure to violence) and three physical (crowding, noise, housing problems) risks at each wave of data collection. Exposure to psychosocial risk factors was assessed by maternal ratings on the Life Events and Circumstances Checklist (Work, Cowen, Parker, & Wyman, Reference Work, Cowen, Parker and Wyman1990) and participant's reports on the Adolescent Perceived Events Scale (Compas, Reference Compas1997). At Wave 1 only mother reports were used; at Wave 4 only participant's; and at Waves 2 and 3 both maternal and participant reports were combined with an event counted once if mentioned by either source or both. Noise was assessed continuously with a decibel meter (Bruel & Kjaer, 2239A) in the home over a two-hour period. Residential crowding was indexed as people/room. Housing problems were measured on a standardized instrument consisting of trained raters’ walk-through evaluations of structural problems and maintenance, cleanliness and clutter, physical hazards, and indoor climate conditions (Evans, Wells, Chan, & Saltzman, Reference Evans, Wells, Chan and Saltzman2000). This standardized scale has been used globally with excellent psychometric properties. These three physical risk factors were calculated the same way at each wave of data collection. For each of the six risk factors at each wave of data collection, exposure in the upper quartile was designated equal to a value of 1 and remaining exposure levels designated as 0, yielding a cumulative risk exposure index ranging from 0–6 at each wave of data. This additive cumulative risk index is the most robust and psychometrically sound index of exposure to multiple risk factors (see Evans et al., Reference Evans, Li and Whipple2013; Kraemer et al., Reference Kraemer, Lowe and Kupfer2005; Obradovic et al., Reference Obradovic, Shaffer, Masten, Mayes and Lewis2012; Pressman et al., Reference Pressman, Klebanov, Brooks-Gunn, Mayes and Lewis2012; Sameroff, Reference Sameroff, Clarke-Stewart and Dunn J2006 for detailed discussions about cumulative risk theory and measurement).
Results
Table 1 provides zero-order correlations. Data were missing completely at random, χ2 = 149.78, p = .20) thus multiple imputation of missing data was calculated (Little, Reference Little1988). To test whether the proportion of life spent in poverty from birth to late childhood predicted the slope of well-being indices from late childhood to adulthood, we ran a series of multilevel models in MPlus (Muthen & Muthen, Reference Muthen and Muthen2011). Poverty was grand-mean centered, random slopes were generated for each participant, and gender was added as a covariate given its association with the outcome variables. There were no significant gender by poverty interactions for any of the growth curves. For each well-being index, wave of data collection (at ages 9, 13, 17, 24) was used to predict a growth curve for each participant. At Level 2, the slope of the well-being index was predicted by proportion of life spent in poverty from birth to age 9 (see Figures 1–4). This analysis allows us to assess the extent to which the change in well-being indices over time was associated with the amount of time an individual spent in poverty in early life.

Figure 1. Slope of internalizing symptoms over time for poor and not poor early childhood participants.

Figure 2. Slope of externalizing symptoms over time for poor and not poor early childhood participants.

Figure 3. Slope of learned helplessness over time for poor and not poor early childhood participants.

Figure 4. Slope of allostatic load over time for poor and not poor early childhood participants.
Table 1. Intercorrelations for all study variables
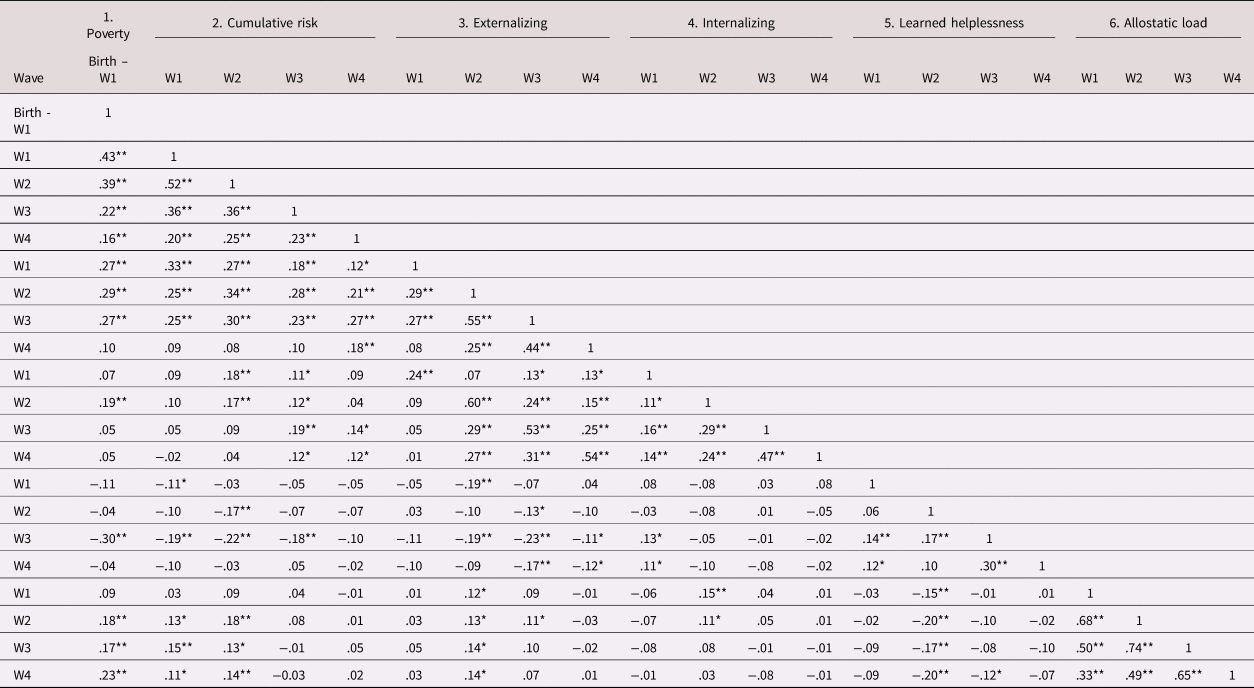
Note. 1: Poverty, 2: Cumulative risk, 3: Externalizing, 4: Internalizing, 5: Learned helplessness; 6: Allostatic load. W1, W2, W3, W4 equals waves of data collection at ages 9, 13, 17, and 24 years.
* p < .05, **p < .01.
Multilevel results show that the proportion of early life spent in poverty significantly predicts individual trajectories of multiple measures of psychological well-being over time. The proportion of early childhood spent in poverty (birth to age 9) alters the trajectories for internalizing (b = .02, CI = .01–.03; B = .15), externalizing (b = .04, CI = .03–.05; B = .35), learned helplessness (b = −.03, CI = −.04–−.01; B = −.24), and allostatic load (b = .11, CI = .08–.20; B = .14). See Table 2. Note that the continuous values of proportion of life in early childhood poverty were used in all inferential tests. The data are categorized as poor versus not poor in Figures 1–4 for descriptive purposes only with the growth curve analyses preserving the continuous variable of proportion of life in poverty from birth to age 9.
Table 2. Total, direct, and indirect path loadings for mediation models

Note. *p <. 05, **p <. 01, ***p < .001.
Finally, to test whether the slope of cumulative risk exposure over time mediated the association between early childhood poverty and the slope of the mental health indices, a series of indirect effects models were run in MPlus. At Level 1, the slope of cumulative risk exposure was added to the models by using wave of data collection (at ages 9, 13, 17, 24) to predict a growth curve for each participant. At Level 2, an indirect effect was defined by generating the interaction term between Path A (defined by regressing the slope of Cumulative Risk onto Poverty) and Path B (defined by regressing the slope of each mental health index onto the slope of Cumulative Risk).
As shown in Figure 5, early childhood poverty significantly predicted greater cumulative risk exposure over time, b = .22, p < .001, CI = .16–.28. As indicated in Table 2, the indirect effect of poverty through cumulative risk exposure significantly predicted the slope of externalizing and internalizing symptoms but not the slope of Learned Helplessness or Allostatic Load.

Figure 5. Slope of cumulative risk over time for poor and not poor early childhood participants.
Sensitivity analyses
In order to examine both the robustness of our major findings as well as probe in more detail alternative mediating mechanisms, several additional analyses were conducted. Bonferroni corrections were applied to these post-hoc analyses.
The initial set of analyses focused on whether the childhood poverty influences on the four growth curves (Figures 1–4) uncovered in our primary analyses above reflect early in life poverty exposure or are a function of the accumulation of poverty exposure over time. Thus we repeated each of the four growth curves regressing the slope of the outcome variable onto the duration of poverty exposure from birth to Wave 1 (age 9) with gender as a covariate and added a second covariate, income to needs at Wave 4 (age 24). The results for externalizing, learned helplessness, and allostatic load remained unchanged with the duration of early childhood poverty significantly predicting the growth curves for externalizing, b = .03, CI = .02–.04; learned helplessness, b = −.02, CI = −.04–−.01; allostatic load, b = .13, CI = .07–.20. The growth curve for internalizing symptoms no longer significantly followed from early childhood poverty, b = .01, CI = −.01–.02 when income to needs at Wave 4 was included in the model.
The second and third sets of sensitivity analyses examined alternative mediating mechanisms to account for the significant link between early poverty exposure and subsequent changes in psychological well-being from age 9 to age 24. We subdivided the original cumulative risk measure into two risk domains reflecting psychosocial cumulative risks (i.e., family turmoil, separation from family, and violence) and physical cumulative risk (i.e., crowding, residential noise, and housing quality), respectively. We used the same criteria for risk designation as described in the Method section risk designation. We then ran growth curve analyses regressing the slopes for each outcome variable on to the duration of poverty from birth to Wave 1 with the addition of one of these two, domain-specific cumulative risk indices. We found that the slope of cumulative psychosocial risk exposures mediated maturation in externalizing symptoms, indirect effect b = .02, CI = .01–.03. No other indirect effects were significant.
The final set of sensitivity analyses explored two, alternative mediating mechanisms. We do not have data on any of these mediating mechanisms for Wave 4 so growth curves for Waves 1–3 are examined to see if either of them mediate the developmental outcomes of childhood poverty on each of the four developmental trajectories (i.e., internalizing symptoms, externalizing symptoms, learned helplessness, chronic physiological stress). The first alternative mediator was maternal sensitivity assessed by maternal descriptions of responsiveness (0 = Never to 4 = Very often) to the child's needs (e.g. “ When [target child] is worried or upset about something, I let her/him know we can talk about it“; “When [target child] wants to talk with me, I find the time”). The second mediator examined was social cohesion in the family assessed from the Moos Family Climate Scales (Moos & Moos, Reference Moos and Moos2009). Two sample items are “Family members really help and support one another” and “There is a feeling of togetherness in our family”. These are scores as 0|1 (True or False). Each of these mediators was examined for the four outcomes. None of these alternative mediational growth curve analyses yielded a significant indirect effect.
Discussion
Growing up in a low-income household is related to multimethodological indicators of psychological well-being trajectories age 9 to 24. The more marked increases in externalizing symptom (e.g., aggression, conflict) trajectories in relation to early poverty relative to more modest changes in internalizing (e.g., depression, anxiety) trajectories match the preponderance of prior evidence indicating stronger and more consistent externalizing correlates of poverty among children and adolescents (Bradley & Corwyn, Reference Bradley and Corwyn2002; Grant et al., Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003; McLoyd, Reference McLoyd1998; Wadsworth et al., Reference Wadsworth, Evans, Grant, Carter, Duffy and Cicchetti D2016). The relation between the proportion of life in early poverty and maturational patterns of psychological well-being development are robust in several respects. First, we show that the accumulation of poverty exposure from birth to age 9 is significantly related to self-reported behavioral problems, a task measure of learned helplessness, and to chronic physiological stress. Furthermore, for three of the four developmental trajectories (externalizing symptoms, learned helplessness, and chronic physiological stress), these early childhood effects are independent of income levels as an adult.
The present findings contribute to the poverty and psychological well-being development literature in several ways. First, we show that maturational patterns of psychological well-being throughout childhood and into adulthood are related to childhood poverty exposure. Second, we supplement symptom rating scales with an overt, behavioral measure of learned helplessness, and with a composite index of chronic physiological stress (allostatic load). Few studies have examined the link between childhood disadvantage and learned helplessness (Brown, Reference Brown2009; Brown et al., Reference Brown, Seyler, Knorr, Garnett and Laurenceau2016; Evans & Cassells, 2017; Evans & English, Reference Evans and English2002), and this is the only study to show that maturational shifts in persistence to solve challenging puzzles are compromised by childhood poverty. A critical but understudied aspect of the etiology of physical and mental well-being concomitants of childhood poverty is learned helplessness. Both the volume and uncontrollability of environmental challenges facing low-income families may undermine a sense of competency and self-efficacy. We also extend previous work showing linkages between childhood disadvantage and elevated allostatic load (Brody et al., Reference Brody, Yu, Chen and Kogan2013, Reference Brody, Lei, Chen and Miller2014; Evans & Kim, Reference Evans and Kim2012; Evans & Schamberg, Reference Evans and Schamberg2009; Milligan et al., Reference Milligan, Thompson, Vandongen, Beilin and Burke1995; Rainisch & Upchurch, Reference Rainisch and Upchurch2013; Worthman & Panter-Brick, Reference Worthman and Panter-Brick2008) by providing, for the first time, growth curve analyses of these effects. Consistent with prior point estimates of allostatic load and childhood disadvantage, we show that the degree of elevation in allostatic load over time is accelerated among those who spent longer durations of early childhood in poverty.
Whereas the amount of data demonstrating linkages between childhood poverty and elevated behavioral problems is large, less is known about the mechanisms underlying the robust evidence on this relation (Bradley & Corwyn, Reference Bradley and Corwyn2002; Grant et al., Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003; McLoyd, Reference McLoyd1998; Wadsworth et al., Reference Wadsworth, Evans, Grant, Carter, Duffy and Cicchetti D2016). As such, our third contribution is demonstrating that changes in exposure to cumulative risk factors accompanying poverty convey some of its impacts on internalizing and externalizing symptoms throughout the life course. Unfortunately, disadvantaged children and their caregivers face a plethora of suboptimal environmental conditions such as substandard housing, crowding, and noise along with more strains in their social environments including family turmoil, violence, and separation from primary caregivers (Evans, Reference Evans2004; McEwen & McEwen, Reference McEwen and McEwen2017; Repetti et al., Reference Repetti, Taylor and Seeman2002; Taylor et al., Reference Taylor, Repetti and Seeman1997). We show that the degree of convergence of such risk exposures over time impacts behavior problem trajectories, and that these effects help account for the robust behavior problem sequelae of childhood poverty.
It is important to note, however, that these significant growth curve mediational findings for cumulative risk exposure do not extend to learned helplessness behaviors or to chronic physiological stress. Helplessness is particularly sensitive to the degree of controllability in risk exposures which our index of cumulative risk exposure may not capture well. Rather than the intensity of risk exposure, the degree of controllability or mastery over the risk may be more critical for learned helplessness (Cohen, Reference Cohen1980; Glass & Singer, Reference Glass and Singer1972; Peterson, Maier, & Seligman, Reference Peterson, Maier and Seligman1993). In future work it would be valuable to assess both the intensity of risk exposure as well as individual's assessments of the degree of controllability over the risk exposure. This is particularly relevant to poverty given the high degree of instability that pervades the lives of many low-income children. Disadvantaged children are much more likely to face residential relocations, nonnormative changes in schools, and alterations in the composition of their households (Evans, Eckenrode, & Marcynyszyn, Reference Evans, Eckenrode, Marcynyszyn, Evans and Wachs2010). Not only is instability stressful, it may also erode various resources such as social support.
Prior research, primarily cross-sectional, suggests that cumulative risk exposure can help account for some of the ill effects of early childhood poverty on health and well-being (Evans & Kim, Reference Evans and Kim2010). We extend and strengthen that work by showing that not only is cumulative risk exposure one of the pathways that appears to explain why childhood poverty leads to elevated behavior problems, but also that trajectories of cumulative risk exposure remain elevated throughout childhood at least until early adulthood for those growing up in poverty. We also show that these trajectories account for some of the variability in behavioral problem trajectories over time. Schoon et al. (Reference Schoon, Sacker and Bartley2003) also found evidence in the UK Millennium birth cohort that higher levels of exposure to risk factors over time partly accounted for the ill effects of poverty on behavior problems throughout childhood, adolescence, and adulthood. However, her risk exposure metric was different than the cumulative risk index herein. We show that the amount of exposure to high levels of physical (crowding, noise, housing problems) and psychosocial (violence, family turmoil, separation from family) risks partially mediates internalizing and externalizing sequelae of childhood poverty. Schoon found that parental occupational status, material conditions, and receipt of social welfare conveyed much of the adverse impacts of poverty on mental health over time.
With additional sensitivity analyses, we also provide information about the nature of the cumulative risk metric. We find that disaggregating the cumulative risk metric into two respective domains of psychosocial risk factors (family turmoil, separation from family, violence) and physical risk factors (housing problems, noise, crowding) in general has little or no mediating impacts. Of the eight mediational analyses (two mediator domains: psychosocial, physical by four growth curves), only one of the specific risk domain analyses (psychosocial risks and externalizing symptoms) yielded a significant, indirect effect. In addition, this indirect effect is smaller than that found for the full psychosocial and physical cumulative risk index.
Finally, we tested the viability of two alternative, mediational constructs in addition to cumulative risk exposure to account for the impacts of early childhood disadvantage on psychological well-being developmental trajectories. The first alternative mediating construct, maternal sensitivity, did not mediate any of the growth curves. This negative finding contradicts a large literature indicating that insensitive and harsh parenting is a viable, underlying pathway that helps explain why early disadvantage leads to adverse developmental outcomes (Conger & Donnellan, Reference Conger and Donnellan2007; Grant et al., Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003; Repetti et al., Reference Repetti, Taylor and Seeman2002). One reason for this non-replication might be our extension of prior work on behavioral problems to also include a behavioral index of learned helplessness and a composite, biomarker (allostatic load) of chronic physiological stress. However, this does not explain the lack of replication for maternal sensitivity mediating behavioral problems which both the Conger and Donnellan (Reference Conger and Donnellan2007) and Grant et al. (Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003) reviews reveal is a robust phenomenon. A second reason for the non-replication could be that in most of the studies that reveal the poverty → parenting → behavior problems pathway, both insensitivity and harshness are included together in the mediating variable construct. We did not do this, assessing only maternal sensitivity. A third explanation could be that we are testing mediation of behavioral problems growth curves. The prior studies have been restricted to concurrent or prospective, point estimates of behavioral problems in relation to childhood disadvantage rather than examination of developmental trajectories. Nonetheless, the lack of replication for maternal sensitivity as an underlying explanation for the ill effects of early disadvantage on multiple indicators of child development calls for further examination of the boundary conditions for this underlying mechanism. This would seem especially important in consideration of the ability of maternal sensitivity to account for developmental trajectories of psychological well-being development. We also explored the potential mediating effects of social cohesion within the family on psychological well-being development over time. We uncovered no evidence for this alternative mediating mechanism.
Although the present study makes several contributions to what we know about childhood poverty, human development, and psychopathology, like most research on social factors and health and well-being, the design is nonexperimental and thus subject to alternative causal explanations. It is worth noting, however, that recent reviews of the few experimental studies of childhood poverty (e.g., Earned Income Tax Credit or Conditional Cash Transfer programs, respectively which provide income supplements to poor families, plus several adoption studies) find consistent, converging evidence with abundant correlational data on the ill effects of poverty on children's cognitive and psychological well-being development (Adler, Bush, & Pantell, Reference Adler, Bush and Pantell2012; Cooper & Stewart, Reference Cooper and Stewart2013, Reference Cooper and Stewart2017; National Academy of Sciences, 2019).
Some additional limitations also stem from the design of the study. The inter-wave intervals are longer than ideal, thus precluding our ability to capture a more fine-grained description of development trajectories. Similarly, by defining poverty exposure from birth to age 9, we lose the ability to examine precise developmental timing of poverty exposure, particularly during the early childhood period. Ideally, we should have initiated data collection at an earlier age and done it more often. However given the strong covariation in income over time, particularly common in rural samples such as this one, the challenge of multicollinearity renders such analyses challenging. We can say with confidence that the duration of childhood exposure to poverty appears to affect the developmental trajectories of several, multimethodological indicators of psychological well-being development. As noted in a sensitivity analysis above, incorporating a statistical control for concurrent income at Wave 4 (age 24) did not alter the conclusions, with the exception of internalizing symptoms. For this developmental trajectory which is more weakly linked to childhood poverty herein and in many other studies (Bradley & Corwyn, Reference Bradley and Corwyn2002; Grant et al., Reference Grant, Compas, Stuhlmacher, Thurm, McMahon and Halpert2003; McLoyd, Reference McLoyd1998; Wadsworth et al., Reference Wadsworth, Evans, Grant, Carter, Duffy and Cicchetti D2016), inclusion of a statistical control for adult income diminishes the effects of early childhood disadvantage.
In addition to strengthening the research design, some additional questions and issues raised by these findings emerge. First, it is unlikely that any one mediating process such as cumulative risk exposure, parenting quality, or child investments alone is likely to transmit all or even most of the covariation between such a complex, powerful factor as childhood disadvantage and developmental outcomes. Nor should we necessarily expect that the same mechanism would operate similarly for different developmental domains (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996). Our data in fact support the latter point given that cumulative risk exposure does provide some explanatory power for behavioral problems but not for learned helplessness or chronic physiological stress. The latter finding is particularly surprising given prior findings from earlier waves of the present research program showing both cross sectionally and in a prospective, longitudinal design that early poverty's positive correlations with allostatic load were mediated by cumulative risk exposure (Evans & English, Reference Evans and English2002; Evans & Kim, Reference Evans and Kim2012). One important difference between the current and former studies is our use herein of developmental trajectories. In Sensitivity Analyses above we provide some additional exploratory analyses to examine other potential, underlying mediating mechanisms. Current scientific thinking and analysis of underlying explanatory processes to explain main effects is moving towards more nuanced evaluations of multiple mediating factors. This perspective needs to be applied to poverty research where there is a dearth of such analyses (Hackman, Gallop, Evans, & Farah, Reference Hackman, Gallop, Evans and Farah2015). Another shortcoming of the present paper is inattention to potential moderators of the various mediational pathways that might help explain why early disadvantage sets children on compromised developmental trajectories. For instance temperament which has well documented interactions with self-regulatory skills (Blair, Reference Blair2019; Carlson, Zelazo, & Faja, Reference Carlson, Zelazo, Faja and Zelazo2013; Muller & Kerns, Reference Muller, Kerns and Lerner2015) and with life circumstances (Belsky & Pluess, Reference Belsky and Pluess2007; Ellis & Boyce, Reference Ellis and Boyce2008), along with control-related beliefs such as self-efficacy or mastery that interact with stressor exposure (Averill, Reference Averill1973; Cohen, Evans, Krantz, & Stokols, Reference Cohen, Evans, Krantz and Stokols1986), are prime candidates worthy of inclusion in work on childhood disadvantage and human development.
Another topic warranting further exploration is whether the relations among childhood disadvantage, behavioral problems, learned helplessness, and chronic physiological stress can be unpacked. For instance in a previous paper, Evans and Schamberg (Reference Evans and Schamberg2009) showed that childhood poverty's inverse relationship with working memory was explained, in part, by elevated, chronic physiological stress (allostatic load). For behavioral problems one might examine, for instance, whether internalizing or externalizing sequelae of childhood poverty are accounted for by learned helplessness. Parallel to this one could explore whether chronic physiological stress helps explain the link between childhood poverty and learned helplessness. It would also have been valuable to incorporate measures of cognitive development such as verbal and analytic skills along with executive functioning into this research program over time. We have no measures of cognitive achievement but did show in cross-sectional data that early poverty was associated with decrements in children's delay of gratification at age 9 (Evans & English, Reference Evans and English2002) and adolescent working memory at age 17 (Evans & Schamberg, Reference Evans and Schamberg2009). Unfortunately, we did not collect executive functioning data throughout this research program. Given what we now know about childhood socioeconomic status (SES) and executive functioning (Blair, Reference Blair2019; Lawson, Hook, & Farah, Reference Lawson, Hook and Farah2018), in hindsight inclusion of these measures over time would have been especially valuable.
Childhood poverty is inimical to human development. Not only the levels but the form of developmental trajectories of children, youth, and young adults are altered in ways that do not bode well for the long-term physical and psychological well-being of individuals growing up in disadvantaged families. Some of these impacts, particularly for depression, anxiety, and behavioral conduct problems, appear to be conveyed, in part, by exposure to greater levels of cumulative risk throughout life. Unfortunately, the plethora of risk exposure beginning in childhood for poor families continues to take a toll on trajectories of behavioral problems of their children throughout life.
Acknowledgments
We are grateful to the families who have been participating in this research for two decades. We thank Shoshana Aleinikoff, Daniel Bartholomew, Jana Cooperman, Kim English, Missy Globerman, Matt Kleinman, Rebecca Kurland, Melissa Medoway, Tina Merilees, Chanelle Richards, Adam Rohksar, Amy Scheier, and Kyle Sherman-Wilkins for assistance with data collection.
Funding Statement
This research was supported by the W.T. Grant Foundation, the John D. and Catherine T. Mac Arthur Foundation Network on Socioeconomic Status and Health, and National Institute for Minority Health and Health Disparities Grant 5RC2MD00467.
Conflict of Interest
None







