The CentriMag ventricular assist device (Thoratec Corporation, Pleasanton, California, United States of America) is a third-generation bearingless centrifugal pump designed for short-term mechanical support. It has emerged as an effective short-term ventricular assist device in adults over the past decade.Reference John, Liao and Lietz 1 – Reference Shuhaiber, Jenkins and Berman 3 It has also increasingly been adopted as a bridge to transplantation and recovery in children.Reference Hirata, Charette, Mosca, Quaegebeur and Chen 4 The use of the CentriMag pump in children poses certain unique challenges. We describe these challenges with reference to its use as a bridge to recovery in a child with chemotherapy-induced heart failure.
Case summary
A 7-year-old male patient with a history of leukaemia was referred from an outside institution for severely depressed heart function following two cycles of chemotherapy. At admission, the left ventricular ejection fraction measured ~10% with severely depressed right ventricular function. There was also evidence of severe end organ dysfunction. The decision was made to place the patient on ventricular assist device as a bridge to possible recovery. The Berlin Heart Excor (Berlin Heart GmbH, Berlin, Germany) was not considered as the patient was not a candidate for heart transplantation. Extracorporeal membrane oxygenation was again not a good option because of the increasing risk profile associated with its use beyond 2- to 3-week period. The CentriMag assist device pump emerged as the best option.
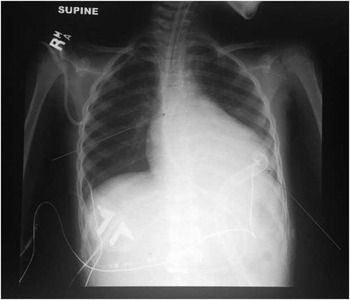
A transoesophageal echocardiogram confirmed severely depressed left ventricle function, with no evidence of septal defects or thrombus. Following standard median sternotomy inflow (34 DLP; Medtronic Inc., Minneapolis, Minnesota, United States of America) and outflow (18 F EOPA; Medtronic Inc.), cannulas were tunnelled from previously marked skin sites across the anterior abdominal wall to the mediastinum. The patient was placed on cardiopulmonary bypass through cannulation of the ascending aorta and right atrium. The inflow cannula was placed through the left ventricular apex and secured in position using two Ethibond purse strings. The outflow cannula was placed in the ascending aorta and secured in position using two Prolene purse strings. Both cannulas were deaired and connected to CentriMag pump (Fig 1). Additional sutures were placed over both the cannulas to secure them to the skin of the abdominal wall. Following complete separation from cardiopulmonary bypass, the assist device flow was steadily increased to achieve cardiac index of 2 L/minute/m2. Echocardiogram demonstrated neutral position of the septum and improved right ventricular function. Hemostasis was secured and both cannulas were wrapped in Gore-Tex sheet before chest closure.

Figure 1 Chest X-ray demonstrating position of inflow and outflow cannulae.
The activated clotting time was maintained between 160 and 200 seconds using continuous heparin drip in the post-operative period. Continuous infusions of epinephrine (0.07 mcg/kg/minute) and milrinone (1 mcg/kg/minute) were used to support the right ventricle. Systemic hypertension was treated with nitroprusside and esmolol infusions to achieve mean arterial blood pressure around 90 mmHg. The patient was extubated within 24 hours of device implantation. An increase in chest tube output was noted following extubation and this did not subside with lowering of heparin. At re-exploration, there was no evidence of surgical bleeding. The same sequence of events repeated following extubation for a second time. Each time, the bleeding subsided with lower mean blood pressure under anaesthesia. Following this realisation, the mean blood pressure was strictly managed around 70 mmHg with no further episodes of bleeding. This strategy worked well and the heart showed significant recovery over the next 3 weeks. The patient was not allowed to ambulate during this time. He tolerated weaning of the device well. The device was subsequently explanted on bypass. His left ventricle ejection fraction at the time of explant was 50–55% with low normal right ventricle systolic function. The patient progressed well and was discharged from the hospital. At follow-up more than a year later, the patient continues to do well with a normal ejection fraction.
Discussion
Although the patient did well and was discharged home, there were some important things we learned about the use of CentriMag assist device in children.
Choice of pump head
The CentriMag pump is designed to provide flows up to 10 L/minute with priming volume of 31 cc. The paediatric version of the device, that is, the PediMag (Thoratec Corporation, Pleasanton, California, USA), provides flows up to 1.5 L/minute and has priming volume of 14 cc. The choice of pump is always not obvious as, for example, in a child requiring flow of 2.5 L/minute. In such cases one has to choose between partial support with PediMag running at high speed (and risk of haemolysis) or full support with a CentriMag operating at lower speed (and risk of thrombosis).
Cannulas for CentriMag
The CentriMag device does not come equipped with special cannulas for central cannulation in children. This is unlike the Berlin Excor that offers a wide range of cannulas with Dacron cuff. We used Medtronic cannulas for our patient. Although these cannulas can be secured by purse strings at the sites of cannulation and abdominal wall exit, sliding movement cannot be eliminated. This makes ambulation risky. Some groups have reported use of Berlin cannulas for the CentriMag device.Reference Maat, van Thiel, Dalinghaus and Bogers 5 , Reference Loforte, Potapov and Krabatsch 6 Others have described novel techniques to secure cannulas.Reference Takayama, Chen, Jorde and Naka 7
Flow rates and mean arterial pressures on CentriMag
The CentriMag is a continuous flow device and the same principles of post-operative management apply as for any other continuous flow device.Reference Slaughter, Pagani and Rogers 8 It is important to initiate flows at a low rate and build it up gradually to avoid systemic hypertension. Goal blood pressure should be age appropriate. At hindsight, our bleeding seemed to be related to high blood pressure in the post-operative period. High blood pressure not only increases afterload on the device but can potentially cause bleeding around the cannulation sites.
Weaning from the CentriMag device
There are no established protocols for weaning children off the CentriMag device. Strategies similar to extracorporeal membrane oxygenation weaning can be used. It is important to maintain higher activated clotting time during this period of low flows and monitor heart function by echocardiogram and serial lactate levels.
Conclusion
The rapidity and ease of implantation along with low incidence of pump-related complications make CentriMag an attractive device for extended use in children. However, it is important to appreciate the challenges that come along when used in children.
Acknowledgements
We would like to acknowledge the support of Dr Mayte Figueroa and Dr Mohammed Ali, cardiac intensive care attendings, who were intensely involved in the care of the patient. We would also like to acknowledge the support of our perfusion team consisting of Jerry Allen, Michael Solimine, and Lindsay Berrios.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national guidelines on Humanitarian Use Device and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by the institutional review board of Le Bonheur Children’s Hospital.