


Introduction
The anatomical and physiological details of the auricular branch of the vagus nerve (Arnold's nerve) are legion and have dogged many a medical student. Coughing induced by ear syringing and ear cleaning is commonly ascribed to stimulation of this nerve. The nerve has also been anecdotally implicated as a cause of chronic cough secondary to ear wax, but such a presumption has not been backed with scientific evidence. This report presents a case of recurrent reflex syncope caused by stimulation of the Arnold's nerve. Specific and targeted autonomic function testing demonstrated a hyperactive vagal response consequent to external auditory canal stimulation.
Case report
A 13-year-old girl presented with a six-year history of episodic, repeated attacks of transient loss of awareness and consciousness. The attacks lasted a few minutes and were sometimes associated with amnesia, but had never been associated with local or generalised tonic–clonic movements, loss of sphincteric function, or tongue biting. Computed tomography, magnetic resonance imaging and electro-encephalography (EEG) had been previously undertaken and were all largely normal, although the EEG had suggested a possible left, posterior, temporal, epileptogenic focus. On this basis, the patient had been treated with oral carbamazepine for the last four years, but had continued to suffer attacks.
Most of the attacks had occurred in school and had lasted a few seconds to a few minutes. No associated tinnitus, hearing impairment, headaches, nausea or vomiting was noted. One recent and particularly severe attack had occurred at home, wherein the child had collapsed and lost consciousness, and then recovered spontaneously after a few minutes. Curiously, this attack had occurred while the patient's mother was ‘cleaning’ the girl's ears.
General physical, cardiovascular, central nervous system and routine otological examinations were all normal. The post-auricular area and the external auditory canals were then specifically stimulated by light rubbing with a cotton-tipped ear probe. A feeling of giddiness and light-headedness was evoked on stimulation of the left external auditory canal. No associated nystagmus was noted.
These unusual manifestations prompted a more detailed evaluation of the patient's sympathetic and parasympathetic function at our institution's autonomic function laboratory, within the physiology department. Informed consent was obtained. The child was too young to cooperate with the entire test battery; hence, limited testing was undertaken, and monitoring was restricted to continuous electrocardiography and respiratory movement recording. The cold face test was normal, suggesting normal parasympathetic reactivity. Heart rate variability was also normal, suggesting normal autonomic drive to the heart. The patient was then asked to lie supine, and the post-auricular areas and the external auditory meati were each stimulated with a cotton bud for 30 seconds each. The 30 second interval was chosen so that the confounding effects of respiration-induced heart rate changes (i.e. inspiration-induced bradycardia, also termed sinus bradycardia) could be minimised. A definite bradycardia was demonstrated on stimulation of the left external auditory canal, particularly of its posterior wall, with a drop in heart rate of 12 beats per minute (Table I, Figure 1). Repeating the stimulation with the patient standing elicited similar bradycardia and a sense of fainting. Further stimulation was aborted for fear of precipitating a full fledged syncopal attack. The bradycardia response was reproducible on repeated testing by stimulation of the left external auditory canal posterior wall. No similar response was elicited by control stimulations (bilateral neck), stimulation of the other ear, or even stimulation of the anterior wall of the left external auditory canal (Table I).

Fig. 1 Electrocardiography trace taken with the patient in a standing position, demonstrating bradycardia and an increase in the R–R interval on stimulation of the posterior wall of the left external auditory canal. The lower trace indicates respiratory chest movements.
Table I Variations in heart rate in response to stimulation
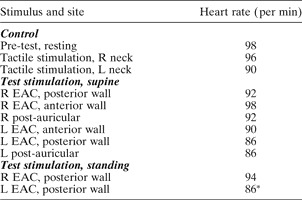
* Associated pre-syncope. Min = minute; R = right, L = left; EAC = external auditory canal
The clinical history, the elicitation of lightheadedness by stimulation of the left external auditory canal in the clinic, and the elicitation of repeated lightheadedness and bradycardia by similar stimulations in the laboratory indicated a diagnosis of Arnold's nerve (i.e. vagus nerve auricular branch) induced bradycardia with resultant syncope.
The patient was advised of the diagnosis, and the treatment was restricted to advice regarding avoiding ear stimulation and ear scratching. The patient thereafter refrained from the same, and at the time of writing had remained symptom free for over three years. Her anti-epileptic medication was discontinued.
Discussion
In this case, the circumstances of the history and the autonomic function testing clearly indicated an aurally mediated bradycardia brought about by stimulating the external auditory canal. It is to be expected that this is mediated by the auricular branch of the vagus nerve (Arnold's nerve), which supplies afferent fibres to the external auditory canal. The term ‘auricular syncope’ is proposed for this unusual manifestation.
Neurally mediated reflex syncope (also termed vasovagal syncope or neurocardiogenic syncope) is the most frequent cause of syncope, accounting for approximately half of all cases.Reference Brignole1 It is usually consequent to emotional or orthostatic stress. However, it may also be precipitated by direct vagal stimulation consequent to carotid sinus stimulation (‘neck tie syncope’), severe coughing or sneezing, gastrointestinal stimulation (swallowing, defecation or visceral pain), or micturition.Reference Brignole1 A comprehensive history by an alert physician, specifically seeking precipitating factors, is the key to the diagnosis. In cases in which the diagnosis remains uncertain, further, specialised testing may be undertaken, including carotid sinus massage, tilt testing and implantable loop recording, and, occasionally, the adenosine triphosphate test, eyeball compression test, external loop recording and Holter monitoring.Reference Brignole1
Auricular syncope, as described here, would best be classified as an unusual type of reflex syncope caused by direct vagal stimulation.
• This paper describes a previously unreported syndrome of recurrent syncopal attacks provoked by light stimulation of the external auditory canal
• Targeted autonomic function tests confirmed a hyperactive vagal response, with documented, significant bradycardia and lightheadedness, provoked by mild stimulation of the posterior wall of the left external auditory canal
• Reflex syncope consequent to stimulation of the auricular branch of the vagus nerve is proposed as the pathophysiological mechanism for this previously undocumented syndrome
The other, more frequent reflex mediated by the auricular branch of the vagus nerve is the cough reflex. Impacted cerumen, foreign bodies, ear syringing and a hair lying against the tympanic membrane have all been reported to induce cough.Reference Ballantyne, Ballantyne and Groves2, Reference Feldman and Woodworth3 Tekdemir et al. noted the frequency of the ear-cough reflex to be 2.3 per cent (12 out of 514 patients), being primarily elicited by simulation of the postero-inferior wall of the external auditory canal, and having a latency of 5 to 10 seconds.Reference Tekdemir, Aslan and Elhan4 These authors did not report syncopal attacks in any of their subjects;Reference Tekdemir, Aslan and Elhan4 however, death caused by ear syringing has been noted.Reference Ballantyne, Ballantyne and Groves2
Vagal nerve stimulation therapy by an implanted electrical stimulator has been demonstrated to alter the concentrations of neurotransmitters and their metabolites in the central nervous system, and is currently being evaluated for the treatment of intractable depression and seizures.Reference Rush, Marangell, Sackeim, George, Brannan and Davis5 It is to be expected that stimulation of Arnold's nerve would have qualitatively similar effects.
The lay belief that light stimulation of the external auditory canal induces a sense of relaxation and satiety may have a neural basis in Arnold's nerve mediated vagal stimulation.Reference Ballantyne, Ballantyne and Groves2 Ancient Vedic practices, wherein the Bramhamanical sacred thread is looped around the ear lobule and gently rubs against the post-auricular skin, may also have its basis in the same neural pathway.


