Coronary artery aneurysms are very rare, with prevalence rates that vary from 0.25% in Asian populationsReference Wang, Ting Ch, Sutton and Cheng1 to 2.6% in White populations.Reference Syel and Lesch2 Aneurysms of the left main coronary artery are even rarer. In a study by Topaz et alReference Topaz, DiSciascio and Cowley3 involving a series of 22,000 coronary angiograms, they were found in only twenty-two patients (an occurrence rate of 0.1%.These dilated sections of the coronary artery are not benign entities because they are subject to spasm, thrombosis, and spontaneous dissection and can be a potential cause of myocardial infarction.
Case report
A 19-year-old school-going male presented to a primary-care physician with prolonged chest pain of 3-hour duration associated with severe perspiration. He had neither conventional risk factors nor a family history of premature coronary artery disease or sudden cardiac death. His electrocardiography showed normal sinus rhythm with ST elevation in inferior leads with possible culprit vessel localisation to the left circumflex artery. Cardiac biomarkers were significantly elevated. In view of lack of facility for primary percutaneous coronary intervention, he was successfully thrombolysed with intravenous streptokinase (15,00,000 units). Following thrombolysis, he had relief from chest pain and electrocardiogram showed ST segment resolution. Later, he was referred to our tertiary cardiac care unit for further evaluation and management.
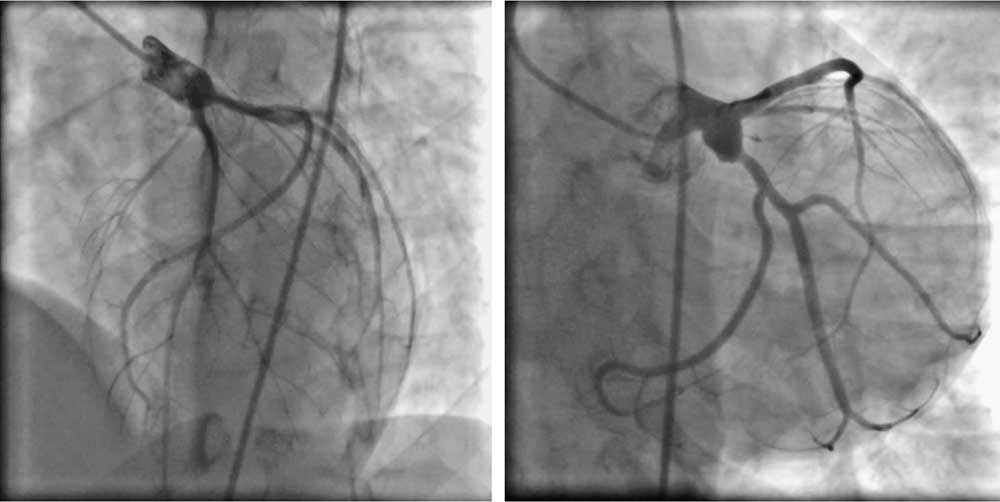
At admission to the coronary care unit, he was haemodynamically stable and the electrocardiogram showed features of evolved inferior wall myocardial infarction. Transthoracic echocardiography showed basal and mid-inferior and -posterior segmental hypokinesia with left ventricular ejection fraction of 45%. He was non-diabetic and his haematological and biochemical parameters, including serum lipid profile, were within normal range. Investigations for hypercoagulable state and connective tissue markers yielded negative results. Later, coronary angiography revealed an aneurysmally dilated left main coronary artery (Fig 1, videos 1–2) with selective extension of the aneurysm towards the proximal left circumflex coronary artery. The left anterior descending artery ostium was not involved in the aneurysm. The left circumflex artery was dominant. Except for the presence of the left main coronary artery aneurysm, the rest of the coronary system was normal. Left ventricular angiography showed hypokinetic diaphragmatic and inferior segments with mildly reduced ejection fraction. The patient was managed conservatively with aspirin, clopidogrel, and anti-coagulants.

Figure 1 Conventional coronary angiography images showing aneurysm of the left main coronary artery with its selective extension into the proximal left circumflex coronary artery with otherwise normal coronary tree. Please note the normal left anterior descending coronary artery without its involvement in the aneurysm.
Discussion
The incidence of coronary artery aneurysms has been reported to be 0.2–4.9% of patients undergoing coronary angiography. Aneurysms of the left main coronary artery are even more rare; in a study by Topaz et alReference Topaz, DiSciascio and Cowley3 involving a series of 22,000 coronary angiograms, they were found in only 22 patients (an occurrence rate of 0.1%). Over 50% of the left main coronary artery aneurysms are atherosclerotic in origin. Other aetiologies include congenital malformations, Kawasaki disease, Marfan and Ehlers-Danlos syndromes, Takayasu’s arteritis, syphilitic or infectious arteritis, thoracic trauma, and fibromuscular dysplasia. Isolated left main coronary artery aneurysm without arteriosclerotic lesions is, therefore, rare, and clinical management of these patients is not well established because of the lack of cases documented in the literature.
As with other aneurysms, it appears that thrombosis or embolisation, or both, with vessel occlusionReference Rath, Har-Zahav and Battler4 and rupture of the aneurysm with sudden cardiac tamponadeReference Iga, Fujikawa, Ueda, Miki and Konishi5 are the two most serious, although rare, consequences and can occur in isolated cases of coronary aneurysm without associated cardiac lesions.
Aneurysms are clinically manifested with acute myocardial infarction accounting for 30–50% of cases.Reference Wang, Ting Ch, Sutton and Cheng1, Reference Von Rotz, Niederhauser, Straumann, Kurz, Bertel and Turina6 The rest either cause myocardial ischaemia or, more often, constitute an occasional finding in coronary angiography. It is reasonable to assume that thrombosis, facilitated by turbulence and local slow flow, can occur within an aneurysm and lead to vessel occlusion, as in our patient the left main coronary artery aneurysm involving the ostial left circumflex artery might have led to inferior wall myocardial infarction.
Although the management of coronary artery aneurysm is not well established as yet owing to the rarity and unpredictable natural history, these dilated sections of the coronary artery are not benign entities because they are subject to spasm, thrombosis, and spontaneous dissection and can be a potential cause of myocardial infarction. In the selected cases of left main coronary artery aneurysm, adequate medical management including anti-platelets and/or anti-coagulation may confer optimal management without surgery with a careful periodic follow-up. If pharmacological treatment fails, then a surgical approach is proposed or an intra-coronary stent implanted. The surgical approach involves the plastic correction of the coronary vessel aneurysm using part of a veinReference Moriyama, Hisatomi, Shimokawa, Taira and Arima7 or of an arteryReference Lepojarvi, Salmela, Huikuri and Karkola8 or stent implantationReference Leung, Wong, Wu, Tsui, Mok and Lau9 or covered stent, plastic correction ligation with bypass graft.
Conclusion
Aneurysm of the left main coronary artery is an uncommon clinical entity and may complicate with acute myocardial infarction. Left main coronary artery aneurysm should be considered when a young patient without conventional risk factors presents with acute myocardial infarction.
Conflict of interest
None declared
Prior Publications/presentations
None