D-transposition of the great arteries with intact ventricular septum has been described in combination with various lesions. The association with aortopulmonary window is very rare. There are very few case reports of aortopulmonary window in d-transposition of the great arteries with intact ventricular septum. Its presence is associated with poor prognosis.Reference Vanini 1 , Reference Krishna, Barron and Brawn 2 Children with transposition of the great arteries presenting late in infancy often have regressed left ventricular mass. An aortopulmonary window, when present, could provide a pressure-head and prevent the left ventricle from regression.Reference Krishnan, Arian, Sambamurthy, Shrivastava, Rajani and Rao 3 , Reference Amato 4
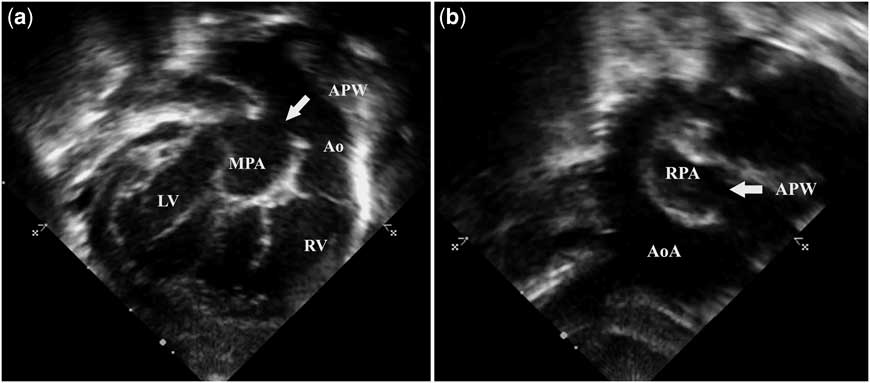
A 3-month-old baby presented with feeding difficulty. The oxygen saturation recorded was 94% in room air, and the electrocardiogram showed features of biventricular dominance. The echocardiographic data showed situs solitus, levocardia, concordant atrioventricular connection, and discordant ventriculoarterial connection with an anterior–posterior relation of the great arteries. The ventricular septum was intact and a tiny ostium secundum atrial septal defect with left to right shunt was present. The left ventricle was functioning normally and had retained its shape. The subcostal echocardiographic evaluation revealed a large aortopulmonary window, which was explanatory of the clinical picture (Fig 1a and b, Supplementary Movies 1 and 2). The higher oxygen saturation, non-regressed left ventricle despite intact ventricular septum with small atrial septal defect and absence of ductus arteriosus were the interesting features. The baby was further evaluated by a paediatric cardiothoracic surgeon and subsequently underwent successful arterial switch with repair of the aortopulmonary window.
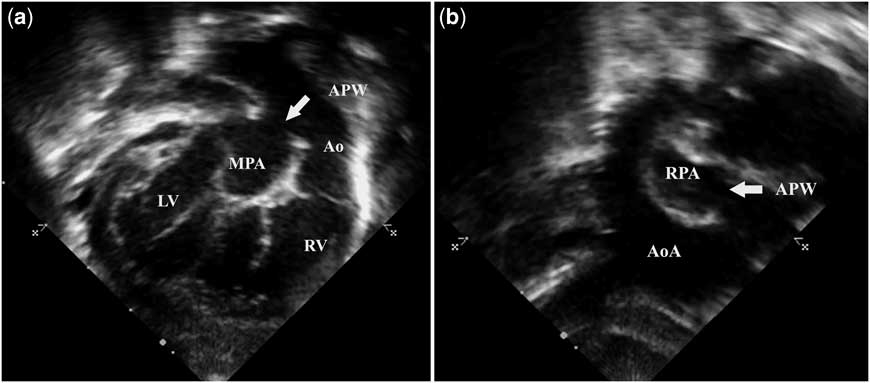
Figure 1 ( a ) Transthoracic echocardiogram subcostal view showing large aortopulmonary window (arrow). ( b ) Transthoracic echocardiogram suprasternal view showing communication (arrow) between the aorta and right pulmonary artery. Ao = aorta; AoA = arch of aorta; APW = aortopulmonary window; LV = left ventricle; MPA = main pulmonary artery; RPA = right pulmonary artery; RV = right ventricle.
Transposition of the great arteries with intact ventricular septum presenting in late infancy usually has regressed left ventricular mass. Rarely, one may come across patients in late infancy in whom the left ventricle has not regressed. These patients need a detailed echocardiographic evaluation for possible causes of elevated pulmonary artery pressure. An aortopulmonary window is an unusual cause for non-regressed or prepared left ventricle in transposition beyond the first month of life. The other common causes for non-regression of the left ventricle are ventricular septal defect, patent ductus arteriosus, and presence of significant aortopulmonary collaterals. Arterial switch operation with repair of the aortopulmonary window is the procedure of choice in these patients, but post-operative pulmonary hypertensive crisis is associated with significant morbidity and mortality.Reference Hopkins, Bull, Haworth, de Leval and Stark 5 , Reference Kumar, Taylor, Sandor and Patterson 6 Previously described patients did not survive the post-operative period and were found to be having pulmonary vascular disease on autopsy. The risk of post-operative pulmonary hypertensive crisis is minimised by using a fenestrated ventricular septal defect patch if transposition is associated with ventricular septal defect. In the presence of an aortopulmonary window, the window can be included at the level of division of the great vessels or leaving fenestration at the atrial level as an easy and useful tool to mitigate the adverse effects of post-operative pulmonary hypertensive crisis.Reference Mignosa, Duca, Bianca, Salvo, Ferlazzo and Abbate 7 Sometimes, an aortopulmonary window may be restrictive and hence the patient is protected from developing severe pulmonary vascular disease and can successfully undergo arterial switch operation and repair of aortopulmonary window.Reference Marwah, Maheshwari, Suresh, Misri and Sharma 8
Acknowledgement
Special thanks to Sajeer Kalathingathodika for his contribution in preparing the figures.
Financial Support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
None.