


Introduction
Enlarged internal auditory canal is a rare congenital developmental anatomical variant. The condition is characterised by usually bilateral, symmetrical, patulous internal auditory canals. It may be clearly visualised, either alone or in combination with other anomalies of the cochlea and labyrinth.
The typical clinical presentation depends upon the type of concomitant congenital inner ear dysplasia, and may include mixed hearing loss, sensorineural hearing loss (SNHL), profound hearing loss, cerebrospinal fluid (CSF) fistulae and meningitis.Reference Phelps1–Reference Weinberg, Kim and Gore3
When no other labyrinth anomaly occurs, patients are asymptomatic, with normal hearing.Reference Migirov4 Diagnosis of their condition may be incidental.
We report the case of a young man with enlarged internal auditory canals who developed sudden SNHL following weight-lifting exercise.
Case report
A previously healthy, 32-year-old man presented to our hospital with sudden, left-sided deafness which had commenced half an hour earlier. The patient had noted left-sided hearing loss immediately following body-building exercise involving repeated lifting of heavy weights. He had no vestibular disturbance.
Otoscopy showed normal tympanic membranes bilaterally.
Pure tone audiometry revealed profound left-sided hearing loss (>90 dB) with no auditory brainstem response. Right-sided hearing was normal (Figure 1).

Fig. 1 The patient's audiogram on presentation, showing profound left-sided hearing loss with normal right-sided hearing.
High resolution computed tomography (CT) scanning of the temporal bone showed bilaterally enlarged internal auditory canals without any associated dysplasia of the labyrinth (Figures 2 and 3). Inner ear assessment was normal; quantitative evaluation of the cochlear height and the bony island of the lateral semicircular canal (as suggested by Purcell et al.) was normal, measuring respectively 5.00 mm (normal value 5.31 ± 1.04) and 4.00 mm (normal value 3.67 ± 0.70) on both sides.Reference Purcell, Johnson, Fischbein and Lalwani5 This was confirmed on magnetic resonance imaging (MRI) (Figure 4). Cerebrospinal fluid collections were seen around the trigeminal ganglia, linked to enlarged foramina for the trigeminal ganglia, similar in concept to the enlargement of the internal auditory canals.

Fig. 2 Axial, high resolution computed tomography scan showing enlarged left internal auditory canal.

Fig. 3 Axial, high resolution computed tomography scan showing enlarged right internal auditory canal.
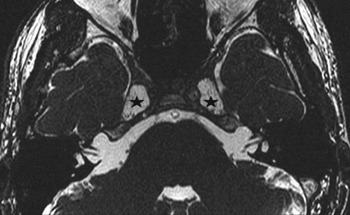
Fig. 4 Axial, T2-weighted magnetic resonance imaging scan showing exceptionally large internal auditory canals with normal cerebrospinal fluid signal and cranial nerve appearances (i.e. the VIIth and superior vestibular nerves in this scan). Associated bilateral herniation of Meckel's cave cistern into the petrous apex (stars) is also seen.
The patient was treated with steroids (prednisone) and an antiviral drug (acyclovir) for 15 days, and a plasma expander for 6 days.
Unfortunately, the patient's hearing loss did not resolve. He resumed his body-building exercise, and suffered no other hearing or vestibular disturbances over the following eight months.
However, during another session of weight-lifting exercise, the patient again experienced sudden hearing loss.
Pure tone audiometry at this time demonstrated a 50 dB, right-sided SNHL (Figure 5). The same therapy as for the previous attack was immediately administered. Furthermore, exploratory tympanotomy was planned to exclude a perilymphatic fistula. No specific lesions were detected at surgery. Repeated MRI confirmed previous appearances.

Fig. 5 Repeated audiogram taken after the patient suffered right-sided hearing loss during another weight-lifting session.
No subsequent recovery of right-sided or left-sided hearing was obtained. The patient was followed up for 14 months, with no improvement in left-sided hearing and no other episodes of vertigo or right-sided hearing deterioration.
Discussion
Enlarged internal auditory canal is a bilateral anatomical variant which appears as increased diameter at the midportion of the internal auditory canal. Patients with this condition may show different patterns of hearing loss associated with other congenital abnormalities.Reference Phelps1, Reference Swartz and Harnsberger2 However, enlarged internal auditory canal is commonly associated with normal hearing. In all reported cases of this condition, patulous internal auditory canal was not combined with any anomaly of the labyrinth.Reference Weinberg, Kim and Gore3, Reference Migirov4
The pathogenetic mechanism of the hearing impairment caused by enlarged internal auditory canal is not well defined and is a subject of debate. However, the present case seems to suggest a new potential pathogenetic mechanism.
The majority of sudden SNHL cases are referred to as idiopathic; a specific aetiology is identified in only 10 to 15 per cent of patients. The importance of identifying and differentiating the various aetiologies of sudden deafness is thus clear. In our patient, it is reasonable to hypothesise that the absence of bony covering of the internal auditory canal may have resulted in reduced protection of the cochlear nerve against increased CSF pressure due to physical straining, as occurred in our patient during repeated lifting of heavy weights. It should be remembered that, at the level of the cochlear foramina nervosa, the nervous filaments are very thin and thus potentially disrupted by a direct CSF pressure wave. In contrast to this hypothesis, however, are many opposing considerations. Sudden SNHL can occur at any time in any patient. Its association with enlarged internal auditory canals in this patient may be purely coincidental.
• Enlarged internal auditory canal is a bilateral anatomical variant which appears as increased diameter at the midportion of the internal auditory canal
• This paper describes a patient with patulous internal auditory canals and no other anomalies, who developed bilateral sudden hearing loss after two separate sessions of weight-lifting exercise
Our patient's offending weight-lifting sessions were unlikely to have been his first. Why did sudden SNHL develop on these two specific occasions? It is difficult to answer this question. Imaging identified no specific features of decreased bone density or thinner bone between the internal auditory canal and the inner ear components. However, it is important to note that sudden SNHL occurred on two different occasions, involving both sides, and that the patient had continued his exercise regime. Furthermore, the presence of perilymphatic fistula of the middle ear was excluded. Thus, it is perhaps reasonable to speculate that, following the patient's first episode of sudden deafness, warnings regarding the need to cease athletic exercise may have prevented the following (fortunately less severe) hearing loss episode.
Such speculation prompted us to recommend that the patient change his lifestyle and avoid athletic exercise. Our current policy is that patients with enlarged internal auditory canals, even if asymptomatic, should be reviewed by an otologist.
Conclusions
To the best of our knowledge, this is the first report of a patient with patulous internal auditory canals, and no other anomalies, who developed bilateral sudden hearing loss. Although no definitive conclusions can be drawn, close surveillance and lifestyle warnings should be considered in such patients.





