Introduction
Cognitive behavioral therapy (CBT) is standard, evidence-based psychotherapy for generalized social anxiety disorder (gSAD), a common, debilitating disorder characterized by excessive fear of situations involving potential scrutiny by others (Kessler et al. Reference Kessler, Berglund, Demler, Jin, Merikangas and Walters2005). According to cognitive models of anxiety, attentional bias to threat attributed to poor attentional control and/or vigilant–avoidant behaviors factors into beliefs that the environment is unduly dangerous or hostile (Eysenck, Reference Eysenck1992; Williams et al. Reference Williams, Watts, MacLeod and Mathews1997; Mogg et al. Reference Mogg, McNamara, Powys, Rawlinson, Seiffer and Bradley2000; Mathews & MacLeod, Reference Mathews and MacLeod2005).
Attentional control refers to implicit emotion regulation, a process involving an appropriate balance between the execution of cognitive goals while being sensitive to motivationally relevant signals outside task-relevant aims (Whalen et al. Reference Whalen, Bush, Shin and Rauch2006; Ochsner et al. Reference Ochsner, Silvers and Buhle2012). Behavioral data showing that anxious individuals have difficultly ignoring threat distractors (Derryberry & Reed, Reference Derryberry and Reed2002; Bögels & Mansell, Reference Bögels and Mansell2004; Moriya & Tanno, Reference Moriya and Tanno2008) point to a disrupted regulation system. Not mutually exclusive of control deficiencies is a vigilant–avoidant strategy (Marks, Reference Marks, Garfield and Bergin1978; Mathews, Reference Mathews1990; Mogg et al. Reference Mogg, Bradley, Miles and Dixon2004), with avoidance (cognitive or behavioral) constituting an explicit means of regulation to cope with anxiety evoked when threat signals are encountered.
CBT attempts to address social and performance-related fears principally through the volitional strategies of cognitive restructuring (e.g. reappraisal of negative beliefs) and elimination of avoidance behaviors, an objective of exposure techniques, which utilizes natural conditioning processes (habituation and extinction). Notably, attentional control is not a direct target of CBT, yet behavioral studies have demonstrated that gSAD is associated with increased control over threat distractors in patients who have responded to treatment (Mattia et al. Reference Mattia, Heimberg and Hope1993; Lundh & Öst, Reference Lundh and Öst2001; Pishyar et al. Reference Pishyar, Harris and Menzies2008). Though it is not entirely clear whether the reduction in attentional bias is due to improved top-down control (e.g. more efficient executive functioning), reduction in the salience of threat, or both, findings imply that brain areas involved in implicit emotion regulation (Whalen et al. Reference Whalen, Bush, Shin and Rauch2006; Etkin et al. Reference Etkin, Egner and Kalisch2011; Ochsner et al. Reference Ochsner, Silvers and Buhle2012) might mediate recovery. Using pre-CBT functional magnetic resonance imaging (fMRI) data might aid in increasing our understanding of mechanisms mediated by CBT and potentially serve to identify biomarkers for individuals who are likely to improve following CBT.
The utility of brain markers as treatment predictors is underscored by the high variability in treatment response, with 30–40% of patients with gSAD failing to fully respond to therapy (Heimberg et al. Reference Heimberg, Liebowitz, Hope, Schneier, Holt, Welkowitz, Juster, Campeas, Bruch, Cloitre, Fallon and Klein1998; Davidson et al. Reference Davidson, Foa, Huppert, Keefe, Franklin, Compton, Zhao, Connor, Lynch and Gadde2004). Highlighting the value of neural predictors is a recent study that revealed that fMRI data were more accurate at classifying CBT responders in patients with generalized anxiety disorder and/or panic disorder than clinical or demographic data (Ball et al. Reference Ball, Stein, Ramsawh, Campbell-Sills and Paulus2013). Thus, biomarkers could be used to tailor initial treatment selection (e.g. CBT versus pharmacotherapy) based on a patient's predicted outcome for a particular treatment (Shin et al. Reference Shin, Davis, Vanelzakker, Dahlgren and Dubois2013).
In light of attentional bias and its remediation in gSAD treatment responders, the anterior cingulate cortex (ACC) is a potential marker of CBT response. The ACC plays a crucial role in attention–emotion processes with the ventral–rostral region predominately associated with evaluative functions and emotion regulation via conflict resolution (Bush et al. Reference Bush, Luu and Posner2000; Etkin et al. Reference Etkin, Egner and Kalisch2011), which interacts with the dorsal–caudal area that is primarily involved in conflict-related processing (e.g. error detection, conflict monitoring) and response to motivationally relevant information (Carter et al. Reference Carter, Braver, Barch, Botvinick, Noll and Cohen1998; Bush et al. Reference Bush, Luu and Posner2000; MacDonald et al. Reference MacDonald, Cohen, Stenger and Carter2000; Botvinick et al. Reference Botvinick, Braver, Barch, Carter and Cohen2001; Liu et al. Reference Liu, Banich, Jacobson and Tanabe2006; Banich et al. Reference Banich, Mackiewicz, Depue, Whitmer, Miller and Heller2009; Etkin et al. Reference Etkin, Egner and Kalisch2011).
Both subregions are implicated in the pathophysiology of gSAD. Specifically, rostral and dorsal ACC hyper-reactivity has been demonstrated in gSAD during threat perception in addition to exaggerated amygdala and anterior insula activation (Etkin & Wager, Reference Etkin and Wager2007; Freitas-Ferrari et al. Reference Freitas-Ferrari, Hallak, Trzesniak, Filho, Machado-de-Sousa, Chagas, Nardi and Crippa2010), key limbic/paralimbic emotion generation and processing regions (Adolphs et al. Reference Adolphs, Tranel, Damasio and Damasio1995; Davidson, Reference Davidson2000; Davis & Whalen, Reference Davis and Whalen2001; Craig, Reference Craig2009; Critchley, Reference Critchley2009; Jones et al. Reference Jones, Ward and Critchley2010). In contrast, when attentional control is required by means of conflict resolution (i.e. counting Stroop, emotional interference), gSAD is linked with reduced rostral and dorsal ACC activation though without concomitant anomalous limbic activity (Blair et al. Reference Blair, Geraci, Smith, Hollon, Devido, Otero, Blair and Pine2012; Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013b ). Thus, depending on the target of attentional deployment, substrates of bias encompass heightened threat processing, consistent with observations that anxiety is characterized by vigilance for threat (Mathews, Reference Mathews1990; Mogg et al. Reference Mogg, Bradley, Miles and Dixon2004) and deficient ‘top-down’ control (Bögels & Mansell, Reference Bögels and Mansell2004), signifying impoverished implicit regulation and/or conflict-related processing disturbances (Liu et al. Reference Liu, Banich, Jacobson and Tanabe2006; Whalen et al. Reference Whalen, Bush, Shin and Rauch2006; Banich et al. Reference Banich, Mackiewicz, Depue, Whitmer, Miller and Heller2009; Etkin et al. Reference Etkin, Egner and Kalisch2011; Ochsner et al. Reference Ochsner, Silvers and Buhle2012).
Regarding brain-based predictors of CBT success in gSAD, we have shown that greater response is foretold by greater pre-treatment activation in the dorsal ACC and other prefrontal regions [e.g. dorsomedial prefrontal cortex (dmPFC), orbitofrontal cortex] for fearful versus happy faces when regressing pre/post-CBT change in symptom severity while controlling for initial severity (Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013b ), suggesting that CBT capitalizes on a hypersensitive system that may involve mechanisms associated with dysfunctional regulation. For example, volitional regulation strategies are subserved by ventral and dorsal prefrontal regions and therefore may be recruited when using avoidance to manage anxiety (Hofmann et al. Reference Hofmann, Ellard and Siegle2012). Interestingly, no association between CBT outcome and amygdala activity emerged, an observation also reported by Doehrmann et al. (Reference Doehrmann, Ghosh, Polli, Reynolds, Horn, Keshavan, Triantafyllou, Saygin, Whitfield-Gabrieli, Hofmann, Pollack and Gabrieli2013) which involved a comparable regression design. In their study, increased CBT response was linked with increased activation to threatening faces in secondary visual areas (e.g. middle temporal gyrus, dorsal and ventral occipitotemporal regions). Similarly, we found that middle temporal gyrus activity positively covaried with treatment outcome (Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013b ). Taken together, individuals with baseline neural substrates associated with enhanced prefrontal and extrastriate reactivity to threat cues may be more likely to attend to threat (e.g. vigilance) but also engage in avoidance behaviors, thus impeding habituation to threat.
Differing results have been found in another anxiety disorder, post-traumatic stress disorder (PTSD), in which CBT response was shown to correspond with decreased baseline rostral ACC activity to subliminal (i.e. masked) fearful faces when initial symptom severity was not controlled for (Bryant et al. Reference Bryant, Felmingham, Kemp, Das, Hughes, Peduto and Williams2008). Reduced pre-treatment amygdala activity to fear-evoking stimuli was also a prognostic indicator of CBT response. Investigators propose that less reactivity in the rostral ACC and amygdala may make it easier to tolerate the anxiety brought about by CBT procedures (Bryant et al. Reference Bryant, Felmingham, Kemp, Das, Hughes, Peduto and Williams2008). In major depressive disorder a slightly different neural pattern has been observed, wherein improvement was predicted by decreased activity in subgenual ACC and increased amygdala reactivity to negative words, independent of baseline severity, indicating that depressed patients with deficient regulatory capacity may benefit most from CBT (Siegle et al. Reference Siegle, Carter and Thase2006). Despite inconsistencies in study design, such as controlling versus not controlling for initial symptom severity which may moderate findings, supraliminal (i.e. consciously perceived) versus subliminal (i.e. below awareness) stimulus presentation, and differences in populations, for example, individuals with PTSD tend to exhibit rostral ACC hypo-activation to threat (Etkin & Wager, Reference Etkin and Wager2007), there is mounting evidence to suggest that the ACC, and possibly the amygdala, are biomarkers of CBT success when attention is directed to relevant stimuli.
In light of cognitive models that propose a causal role for attentional bias in the maintenance of anxiety (Williams et al. Reference Williams, Watts, MacLeod and Mathews1997; Mathews & MacLeod, Reference Mathews and MacLeod2005), attentional control should be taken into consideration when studying relationships between baseline activation and CBT response. It may be the case that individuals with greater pre-CBT reactivity to motivationally relevant cues respond more to CBT when emotion regulation is largely intact. Such a neural profile may be well suited for exposure work that necessitates the activation of a fear structure and the incorporation of new information that is incompatible with pathological fears (Foa & Kozak, Reference Foa and Kozak1986). On the other hand, processes beyond cognitive control (e.g. habituation to fear) are proposed to correct automatic information-processing biases (Öhman & Soares, Reference Öhman and Soares1994; McNally, Reference McNally1995). Moreover, evidence that the therapeutic effects of CBT are mediated by early changes in attentional bias (Abend & Bar-Haim, Reference Abend and Bar-Haim2013) indicates that individuals with less implicit regulatory ability to begin with may have more to gain from CBT. Therefore, the study of attentional control via conflict resolution is an important step toward further delineating mechanisms of therapeutic actions of CBT in gSAD.
To this end, the objective of the current study was to examine attentional control relative to emotion processing with a paradigm shown to probe the rostral ACC and amygdala, respectively, across angry, fearful and happy faces (Klumpp et al. Reference Klumpp, Angstadt and Phan2012b ). In the paradigm, participants are presented with images comprising a trio of geometric shapes (circles, rectangles, triangles) alongside a trio of emotional faces (angry, fearful, happy) within the same field of view. The instruction to ‘match shapes’ elicits attentional control, as directing attention away from faces requires resolving the conflict that arises when salient distractors compete with the non-affective top-down goal (i.e. shapes). ‘Match shapes’ is contrasted with a ‘match faces’ condition, which directs attention towards emotional faces and away from shapes, thereby engaging areas critical for emotion processing (e.g. amygdala: Phan et al. Reference Phan, Wager, Taylor and Liberzon2002; Wager et al. Reference Wager, Phan, Liberzon and Taylor2003).
Based on findings that patients with gSAD compared with healthy controls exhibit reduced rostral ACC recruitment in the presence of angry, fearful or happy face distractors (i.e. match shapes > match faces) (Klumpp et al. Reference Klumpp, Post, Angstadt, Fitzgerald and Phan2013a ), further supporting evidence that emotional faces are especially salient in gSAD (McTeague et al. Reference McTeague, Shumen, Wieser, Lang and Keil2011) and thus difficult to ignore, along with behavioral indications of improved attentional control in treatment responders (Mattia et al. Reference Mattia, Heimberg and Hope1993; Lundh & Öst, Reference Lundh and Öst2001; Pishyar et al. Reference Pishyar, Harris and Menzies2008), we hypothesized that CBT success would be predicted by less baseline rostral ACC activation. Regarding emotion processing (i.e. match faces > match shapes), we hypothesized that results would be consistent with previous data – namely, greater CBT response would positively correspond with more activation in the dorsal ACC and secondary visual areas (Doehrmann et al. Reference Doehrmann, Ghosh, Polli, Reynolds, Horn, Keshavan, Triantafyllou, Saygin, Whitfield-Gabrieli, Hofmann, Pollack and Gabrieli2013; Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013b ). Even though the amygdala has not yet emerged as a predictor of symptom improvement in gSAD (Doehrmann et al. Reference Doehrmann, Ghosh, Polli, Reynolds, Horn, Keshavan, Triantafyllou, Saygin, Whitfield-Gabrieli, Hofmann, Pollack and Gabrieli2013; Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013b ), its study is warranted given the dearth of research in this area and evidence of its predictive ability in other studies. We hypothesized that CBT response would be predicted by decreased amygdala activity during emotion perception (i.e. ‘match faces’) and extended this hypothesis to the anterior insula given accumulating data of its involvement in the pathophysiology of gSAD (Freitas-Ferrari et al. Reference Freitas-Ferrari, Hallak, Trzesniak, Filho, Machado-de-Sousa, Chagas, Nardi and Crippa2010; Schmidt et al. Reference Schmidt, Mohr, Miltner and Straube2010; Klumpp et al. Reference Klumpp, Angstadt and Phan2012a ).
The proposal that less limbic/paralimbic activation during the perceptual assessment of emotional faces would be an indicator of CBT response may appear to contradict the proposal that fear activation is required for therapeutic exposure; however, excessive fear (i.e. above an optimal level for emotional processing) is believed to obstruct habituation (Foa & Kozak, Reference Foa and Kozak1986). In support is evidence that symptom improvement is associated with less, not greater, exposure-based levels of anxiety (Norton et al. Reference Norton, Hayes-Skelton and Klenck2011). Therefore, we hypothesized that patients with pre-CBT diminished reactivity during automatic emotion processing would be more likely to manage anxiety and consequently fully benefit from exposure techniques.
Method
Participants
The current cohort of 21 patients (15 female, six male) comprising two Asian, three African-American, two Hispanic and 14 Caucasian participants with an average age of 24.9 (s.d. = 6.3) years were from a larger cohort in an earlier study (Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013b ). All participants received a diagnosis of gSAD based on the Structured Clinical Interview for DSM-IV (First et al. Reference First, Spitzer, Gibbon and Williams1996) conducted by licensed clinicians in conjunction with the Liebowitz Social Anxiety Scale (LSAS), a symptom severity measure comprising a total score based on fear/anxiety and avoidance subscales (Liebowitz, Reference Liebowitz1987) and the Beck Depression Inventory (BDI; Beck et al. Reference Beck, Steer, Ball and Ranieri1996) to evaluate depression level. As long as gSAD was the primary complaint, we did not exclude patients with co-morbid anxiety disorders, which were specific phobia (n = 3), generalized anxiety disorder (n = 3) and panic disorder (n = 1).
The average pre-CBT LSAS score was 72.5 (s.d. = 11.6), in line with a clinical cut-off of ⩾60 for gSAD (Heimberg et al. Reference Heimberg, Horner, Juster, Safren, Brown, Schneier and Liebowitz1999; Mennin et al. Reference Mennin, Heimberg, Turk and Fresco2002); BDI scores averaged 12.3 (s.d. = 8.4), below the threshold for major depression (Lasa et al. Reference Lasa, Ayuso-Mateos, Vázquez-Barquero, Dı́ez-Manrique and Dowrick2000). Clinical Global Impression-Improvement (CGI-I; Busner & Targum, Reference Busner and Targum2007), comprising a seven-point scale (1 = very much improved, 7 = worsening symptoms), was used to measure treatment response.
All but two participants were free of psychotropic medication, with those two patients remaining on a stable dose of bupropion for at least 8 weeks prior to, and throughout the remainder of, the study. Excluding the two patients who were taking bupropion, seven had a history of a medication trial, but all were free of psychotropric medications at a minimum of 8 weeks prior to study enrollment. Exclusion criteria included co-morbid major depressive disorder, current or recent substance abuse/dependence (within 6 months of study), or any history of major psychiatric illness (e.g. bipolar disorder, psychotic disorder).
Participants were between 18 and 55 years of age, right-handed, and free of current and past major medical or neurological illness, as confirmed by a board-certified physician. None of the participants tested positive for alcohol or illegal substances. All participants provided written informed consent, as approved by the Institutional Review Boards of the University of Michigan Medical School. All procedures complied with the Helsinki Declaration.
Patients received 12 weeks of manualized individual CBT (Hope et al. Reference Hope, Heimberg and Turk2006), which consisted of one 60-min session per week, conducted by the same licensed clinical psychologist under the supervision of a licensed clinical psychologist with expertise in CBT and clinical trial investigations involving CBT to ensure adherence to treatment. CBT comprised psychoeducation, cognitive restructuring, in vivo exposures and relapse prevention (Hope et al. Reference Hope, Heimberg and Turk2006).
fMRI task
During scanning, participants viewed images comprising a trio of geometric shapes (circles, rectangles, triangles) presented alongside a trio of faces within the same field of view (Fig. 1). During the ‘match shapes’ condition, participants selected between two top shapes the one that matched the bottom target shape, whereas in the ‘match faces’ condition, participants selected between two bottom faces (one emotional versus one neutral) the one that matched the top target emotional expression. The faces were chosen from a validated stimulus set (Gur et al. Reference Gur, Schroeder, Turner, McGrath, Chan, Turetsky, Alsop, Maldjian and Gur2002), were presented without repetition, and equally represented both genders.

Fig. 1. Schematic of exemplar ‘match faces’ and ‘match shapes’ blocks in the Emotional Faces Shifting Attention Task.
The task comprised 36 back-to-back blocks: 18 blocks of matching shapes interleaved with 18 blocks of matching emotional faces, counterbalanced across two runs. Each target emotional face condition (angry, fearful and happy) was presented in six 20-s blocks; these were presented pseudo-randomly, without subsequent repetition of individual faces. Each block began with a 4 s cue to either ‘match faces’ (attend to faces) or ‘match shapes’ (attend away from faces) followed by the four sequential matching trials, each lasting 4 s. Participant responses were recorded via button press.
fMRI data acquisition and pre-processing
Functional imaging was performed with blood oxygen level-dependent sensitive whole-brain fMRI on a 3.0 Tesla GE Signa System (General Electric, USA) using a standard radio frequency coil. Images were acquired with 30 axial, 5 mm-thick slices using a standard T2*-sensitive gradient echo reverse spiral acquisition sequence (2 s repetition time; 25 ms echo time; 64 × 64 matrix; 24 cm field of view; flip angle 77°; 3.75 × 3.75 × 5 mm final voxel size). A high-resolution, T1-weighted volumetric anatomical scan was also acquired for anatomical localization. Data from all participants met criteria for quality with minimal motion correction (movements were less than 3 mm in any one direction across each functional run) and the first four volumes from each run were discarded to allow for T1 equilibration effects. Conventional pre-processing steps were used in the Statistical Parametric Mapping (SPM8) software package (Wellcome Trust Centre for Neuroimaging, UK; www.fil.ion.ucl.ac.uk/spm). Briefly, images were temporally corrected to account for differences in slice time collection, spatially realigned to the first image of the first run, normalized to a Montreal Neurological Institute (MNI) template, and smoothed with an 8 mm isotropic Gaussian kernel.
A general linear model was applied to the time series, convolved with the canonical hemodynamic response function and with a 128 s high-pass filter. Blocks of match faces (shapes in ‘background’) and match shapes (faces in ‘background’) were modeled separately based on the target emotion or shape (angry, fearful or happy/circle, square or triangle), resulting in six regressors, the effects of which were estimated for each voxel for each participant and taken to the second level for random-effects analysis.
To investigate baseline predictors of treatment response, match faces versus match shapes, from gSAD pre-treatment scans, were entered into a whole-brain analysis of covariance, regressing LSAS change (change pre-treatment to post-treatment; ΔPreTx – PostTx) while initial severity (LSAS pre-treatment; LSASPreTx) was controlled for as a regressor of no interest. Regions of interest (ROIs), specifically, the ACC, amygdala and anterior insula, were examined at the whole-brain level with significance defined as p < 0.001 uncorrected with at least 10 contiguous voxels per cluster. ROIs were identified by visual assessment and cross-referenced with the Automated Anatomical Labeling atlas based on the Talairach Daemon database (Lancaster et al. Reference Lancaster, Woldorff, Parsons, Liotti, Freitas, Rainey, Kochunov, Nickerson, Mikiten and Fox2000; Tzourio-Mazoyer et al. Reference Tzourio-Mazoyer, Landeau, Papathanassiou, Crivello, Etard, Delcroix, Mazoyer and Joliot2002).
For illustrative purposes and to clarify the directionality of activity with change in symptom severity, 10 mm diameter spherical ROIs were generated around the peak activation of a whole-brain cluster and subsequently parameter estimates (β weights, arbitrary units) were extracted from the spherical ROIs for each participant and submitted to two-tailed Pearson correlations and scatterplots in SPSS (version 20; IBM, USA). Importantly, as attentional control was based on the contrast match faces versus match shapes, control in the presence of emotional distractors was represented by parameter estimates with a value of zero or less (<0) and emotion processing was denoted by values greater than zero (>0).
Results
Behavioral performance
Behavioral data: match shapes
Average accuracy for matching shapes was 91.4%, suggesting that participants followed task instructions. A repeated-measures analysis of variance (ANOVA) revealed no main effect of emotion type (distractor angry, distractor fearful, distractor happy) (F 2,40 = 0.101, p = 0.904). However, mean reaction times (RTs) for accurate trials revealed a main effect for (distractor) emotion (F 2,40 = 4.203, p < 0.030). Follow-up analysis showed that all participants were faster at matching shapes alongside happy versus angry distractors (p < 0.027), with a trend towards faster RTs in the presence of fearful than angry face distractors (p = 0.065). There was no significant effect between fearful and happy distractors (p = 0.377). See Table 1 for behavioral descriptives.
Table 1. Accuracy and reaction times for accurate trials

Data are given as mean (standard error of the mean).
Behavioral data: match faces
Overall, mean accuracy for matching faces was 85.3%, again indicating that participants followed task instructions. A repeated-measures ANOVA revealed a non-significant trend toward a main effect of emotion (angry, fearful, happy) (F 2,40 = 2.457, p = 0.099). Simple-effects analysis indicated that the trend was driven by greater accuracy when matching fearful relative to angry faces (p < 0.053), with a tendency to be more accurate for fearful than happy expressions (p = 0.093). No differences were evident for angry versus happy target faces (p = 0.553).
Mean RTs for accurate trials showed a main effect for emotion (F 2,40 = 13.779, p < 0.001); follow-up analysis revealed that participants were faster at matching happy than angry faces (p < 0.001) and faster for fearful than angry faces (p < 0.001). There was no significant difference between happy and fearful faces (p = 0.867). See Table 1 for behavioral descriptives.
Treatment effects on social anxiety severity
After 12 weeks of individual CBT, gSAD symptom severity, as assessed with the LSAS, significantly decreased from an average of 72.5 (s.d. = 11.6) to 50.4 (s.d. = 19.5) (t = 5.51, p < 0.001), as did depression level [12.3 (s.d. = 8.4) to 6.2 (s.d. = 7.9); t = 3.63, p < 0.002]. Based on the CGI-I, about 70% of the gSAD group (15 of 21 patients) were considered to be ‘responders’ as they were rated to be ‘very much improved’ or ‘much improved’ (CGI-I score of 1 or 2) while six of 21 patients had a CGI-I score of >2 post-treatment and were thus considered ‘non-responders’.
fMRI results
Controlling for initial severity (LSASPreTx), LSAS change (ΔPreTx – PostTx) was predicted by increased pre-treatment activity in the right dorsal ACC (i.e. anterior cingulum) (MNI coordinates 4, 22, 22; Z = 3.62, volume = 368 mm3) during attentional control as evinced by the association between greater improvement and negative parameter estimates of activation (i.e. <0) based on the faces versus shapes contrast (Fig. 2). Additionally, symptom improvement covaried negatively with activity in the left amygdala (MNI coordinates –26, 2, –22; Z = 3.93, volume = 200 mm3) during emotion perception (Fig. 3) as signified by the relationship between less LSAS change and positive parameter estimates of activation (i.e. >0), though the amygdala was only evident when the whole-brain threshold was extended to a more liberal threshold of 0.005 uncorrected. There was no evidence of anterior insula activity.

Fig. 2. (a) Regressing Liebowitz Social Anxiety Scale (LSAS) change (change pre-treatment to post-treatment; ΔPreTx – PostTx) while initial severity (LSAS pre-treatment; LSASPreTx) is controlled for as a regressor of no interest, the brain map depicts whole-brain analysis of covariance showing enhanced dorsal anterior cingulate activity during attentional control in generalized social anxiety disorder (gSAD) as denoted by negative parameter estimates of activation based on the faces versus shapes contrast displayed on the statistical t-map at p < 0.001. (b) Scatterplot of the regression analyses depicting extracted parameter estimates of activation from the dorsal anterior cingulate region of interest showing that greater response to cognitive behavioral therapy in gSAD was predicted by enhanced dorsal anterior cingulate activity in the presence of emotional face distractors. BOLD, Blood oxygen level-dependent; a.u., arbitrary units.

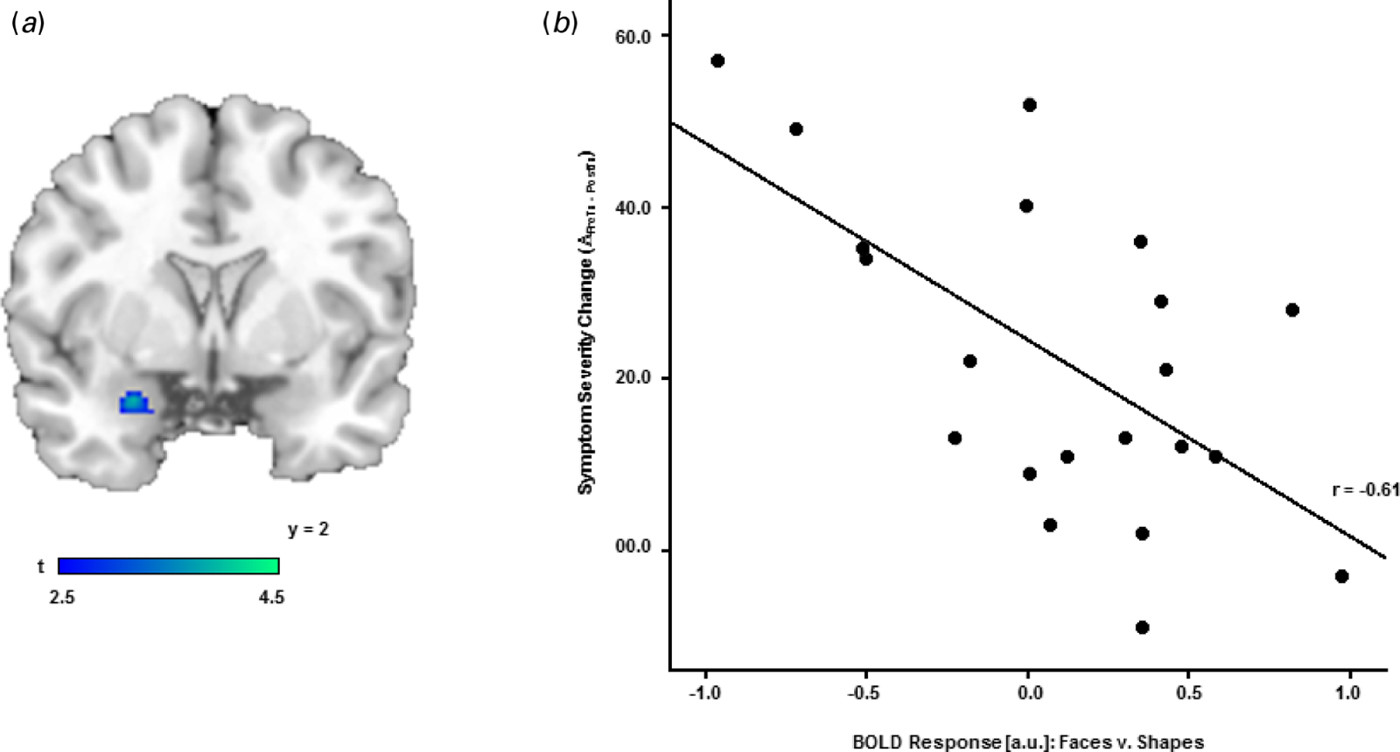
Fig. 3. (a) Regressing Liebowitz Social Anxiety Scale (LSAS) change (change pre-treatment to post-treatment; ΔPreTx – PostTx) while initial severity (LSAS pre-treatment; LSASPreTx) is controlled for as a regressor of no interest, the brain map depicts whole-brain analysis of covariance showing less amygdala activity during emotion processing in generalized social anxiety disorder (gSAD) as denoted by positive parameter estimates of activation based on the faces versus shapes contrast displayed on the statistical t-map at p < 0.005. (b) Scatterplot of the regression analyses depicting extracted parameter estimates of activation from the amygdala region of interest showing that greater response to cognitive behavioral therapy in gSAD was predicted by less amygdala activity to emotional faces. BOLD, Blood oxygen level-dependent; a.u., arbitrary units.
Beyond these ROIs, CBT response was also predicted by a negative relationship in the right frontal superior medial gyrus (MNI coordinates 8, 58, 18; Z = 4.58, volume = 3264 mm3). Due to the relevance of this region in control functions, we submitted parameter estimates to a scatterplot and found that greater activity in the frontal superior medial gyrus during attentional control corresponded with CBT success (Fig. 4).

Fig. 4. (a) Regressing Liebowitz Social Anxiety Scale (LSAS) change (change pre-treatment to post-treatment; ΔPreTx – PostTx) while initial severity (LSAS pre-treatment; LSASPreTx) is controlled for as a regressor of no interest, the brain map depicts whole-brain analysis of covariance showing enhanced frontal superior medial gyrus activity during attentional control in generalized social anxiety disorder (gSAD) as signified by negative parameter estimates of activation based on the faces versus shapes contrast displayed on the statistical t-map at p < 0.001. (b) Scatterplot of the regression analyses depicting extracted parameter estimates of activation from the frontal superior medial gyrus region of interest showing that greater response to cognitive behavioral therapy in gSAD was predicted by greater frontal superior medial gyrus activity in the presence of emotional face distractors. BOLD, Blood oxygen level-dependent; a.u., arbitrary units.
A negative correspondence between CBT success and activity in the left inferior temporal gyrus (MNI coordinates –40, –24, –20; Z = 3.51, volume = 200 mm3), right superior temporal pole (MNI coordinates 46, 18, –24; Z = 3.96, volume = 448 mm3), left precentral gyrus (MNI coordinates –46, 2, 50; Z = 3.88, volume = 256 mm3), left pallidum (M NI coordinates –22, –6, 0; Z = 3.59, volume = 184 mm3), right caudate (MNI coordinates 10, 14, 12; Z = 3.51, volume = 144 mm3) and the right supplementary motor area (MNI coordinates 10, 20, 62; Z = 3.34, volume = 80 mm3) indicates that these regions were subserved either by enhanced activity during attentional control or reduced reactivity to emotional faces.
In contrast to the above results, a positive CBT outcome was predicted by increased activity to emotional faces in the right frontal medial orbital gyrus extending to the medial frontal gyrus (MNI coordinates 8, 36, –14; Z = 3.83, volume = 152 mm3) (Fig. 5). See Table 2 for all regression results.

Fig. 5. (a) Regressing Liebowitz Social Anxiety Scale (LSAS) change (change pre-treatment to post-treatment; ΔPreTx – PostTx) while initial severity (LSAS pre-treatment; LSASPreTx) is controlled for as a regressor of no interest, the brain map depicts whole-brain analysis of covariance showing greater frontal medial orbital gyrus activity during emotion processing in generalized social anxiety disorder (gSAD) as reflected by positive parameter estimates of activation based on the faces versus shapes contrast displayed on the statistical t-map at p < 0.001. (b) Scatterplot of the regression analyses depicting extracted parameter estimates of activation from the frontal medial orbital gyrus region of interest showing that greater response to cognitive behavioral therapy in gSAD was predicted by greater frontal medial orbital gyrus activity to emotional faces. BOLD, Blood oxygen level-dependent; a.u., arbitrary units.
Table 2. Pre-treatment to post-treatment decrease in social anxiety severity, controlling for pre-treatment severity: whole-brain voxel-wise regression a

MNI, Montreal Neurological Institute; Z, Z-score.
a All listed clusters significant at p < 0.001 (uncorrected) with a cluster extent threshold of at least 10 contiguous voxels.
b Cluster significant at p < 0.005 (uncorrected) with a cluster extent threshold of at least 10 contiguous voxels.
c Region of interest.
Discussion
In this study, we used fMRI to examine potential brain predictors of response to CBT in the context of attentional control relative to emotion processing. Based on a standard clinician measure (i.e. CGI-I), the majority of patients with gSAD improved following 12 weeks of individual CBT; however, the extent to which patients benefited from CBT was foretold by baseline individual differences in ROIs – the ACC and amygdala, but not the anterior insula.
We hypothesized that patients with deficient implicit emotion-regulation ability, signified by less rostral ACC activation in the presence of emotional face distractors, would be more likely to benefit from CBT. However, when controlling for initial symptom severity, improvement (i.e. LSAS change; ΔPreTx – PostTx) was predicted by increased activity in the dorsal ACC during attentional control. The dorsal ACC is substantively involved in error detection, conflict monitoring, inhibition of pre-potent responses and appraisal processes (Carter et al. Reference Carter, Braver, Barch, Botvinick, Noll and Cohen1998; Bush et al. Reference Bush, Luu and Posner2000; MacDonald et al. Reference MacDonald, Cohen, Stenger and Carter2000; Botvinick et al. Reference Botvinick, Braver, Barch, Carter and Cohen2001; Etkin et al. Reference Etkin, Egner, Peraza, Kandel and Hirsch2006, Reference Etkin, Egner and Kalisch2011; Liu et al. Reference Liu, Banich, Jacobson and Tanabe2006; Banich et al. Reference Banich, Mackiewicz, Depue, Whitmer, Miller and Heller2009; Kanske & Kotz, Reference Kanske and Kotz2011). Therefore, individuals with gSAD who demonstrated greater pre-treatment dorsal ACC activity when sustained attentional control over emotional distractors was required were more likely to improve potentially due to gating mechanisms that were intact.
CBT response linked with top-down control in the presence of distractors also corresponded with increased pre-treatment activity in the dmPFC (i.e. frontal superior medial gyrus), part of a cognitive control network (e.g. conflict monitoring; Carter et al. Reference Carter, Braver, Barch, Botvinick, Noll and Cohen1998; Botvinick et al. Reference Botvinick, Braver, Barch, Carter and Cohen2001), signifying that patients are benefitted by a dorsal prefrontal functional architecture that diminishes attentional disruptions related to emotional distractors. Presumably, greater activity in top-down control mechanisms facilitates improvement related to conscious, deliberate CBT strategies such as cognitive restructuring, which would be expected to utilize executive functions. Alternatively, the dmPFC, along with the amygdala, has been shown to play a role in anxiety-related vigilance to threat (Robinson et al. Reference Robinson, Charney, Overstreet, Vytal and Grillon2012). Accordingly, CBT response may have corresponded with less attention to face distractors, suggesting that mechanisms that intercede hyper-vigilance rather than regulatory capacity factored into treatment response.
Reduced activation as a prognostic indicator of CBT outcome was observed in the amygdala when using a more liberal threshold than our whole-brain cut-off. Nevertheless, the amygdala result was still within the recommended threshold for determining significance in neuroimaging (Lieberman & Cunningham, Reference Lieberman and Cunningham2009). Our hypothesis that CBT success would be predicted by less pre-CBT amygdala reactivity to emotional faces was supported; as such, results are consonant with Bryant et al. (Reference Bryant, Felmingham, Kemp, Das, Hughes, Peduto and Williams2008) who showed that reduced amygdala activation to threat in PTSD corresponded with improvement following CBT. Greater baseline amygdala reactivity to emotional faces in some patients may reflect a hypersensitivity to pre-potent cues that could be exacerbated in the course of CBT, potentially leading to less engagement in anxiety-eliciting techniques such as exposure. Moreover, the amygdala is thought to be part of an extended face system critical in processing the relevance of information ascertained from facial expressions (Haxby et al. Reference Haxby, Hoffman and Gobbini2002). Consequently, individuals with gSAD who extensively process emotional faces due to delays in disengaging attention from salient information (Yiend & Mathews, Reference Yiend and Mathews2001; Fox et al. Reference Fox, Russo and Dutton2002) or personality traits that heighten amygdala reactivity during emotion processing (e.g. neuroticism; Cremers et al. Reference Cremers, Demenescu, Aleman, Renken, van Tol, van der Wee, Veltman and Roelofs2010; Ormel et al. Reference Ormel, Bastiaansen, Riese, Bos, Servaas, Ellenbogen, Rosmalen and Aleman2013) may benefit less from CBT.
We also proposed that symptom improvement would be linked with reduced anterior insula activity during emotion processing, which was not supported in this study. Although null findings suggest that certain regions implicated in the pathophysiology of gSAD (Etkin & Wager, Reference Etkin and Wager2007; Freitas-Ferrari et al. Reference Freitas-Ferrari, Hallak, Trzesniak, Filho, Machado-de-Sousa, Chagas, Nardi and Crippa2010) may not serve as predictors for treatment response, we cannot rule out the possibility that the small number of patients in our sample may have reduced our ability to detect insula effects.
Beyond ROIs, increased activity to emotional faces in the medial orbitofrontal cortex, encompassing the ventral medial prefrontal cortex (vmPFC), showed a positive correspondence with CBT response. In a previous study, we observed a similar outcome for fearful versus happy faces (Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013a ), thus partially replicating findings. This region has reciprocal connections to the amygdala and is part of an extended medial prefrontal network involved in assessing the valence and value of stimuli, learning associations (e.g. fear extinction, positive reinforcement) and generating adaptive responses that guide behavior (Price, Reference Price1999; Öngür & Price, Reference Öngür and Price2000; Price & Drevets, Reference Price and Drevets2009; Etkin et al. Reference Etkin, Egner and Kalisch2011). Therefore, greater pre-treatment activity to emotional faces in this area suggests that some individuals were more likely to improve if they had an enhanced capacity to regulate responses to emotional signals, potentially due to processes further upstream (e.g. planning of appropriate actions based on stimulus evaluation) that facilitated an adaptive output. A different interpretation concerns the involvement of the vmPFC in safety learning, namely, fear extinction learning and its recall (Quirk et al. Reference Quirk, Garcia and González-Lima2006; Milad et al. Reference Milad, Wright, Orr, Pitman, Quirk and Rauch2007). In this framework, vmPFC activity may reflect associative-learning deficiencies related to the false belief that avoiding fears is the key to feeling safe. As such, instead of CBT capitalizing on regulation capacity, CBT success would be predicted by a ‘deficiency’ signified by maladaptive attempts to regulate reactivity to salient cues. However, as CBT response was also predicted by less amygdala activation during emotion processing, the patients with the most to gain from therapeutic exposures may also have the most difficulty tolerating exposure-related anxiety.
Another area of interest that emerged from whole-brain findings was the inferior temporal gyrus (ITG), a region involved in emotion perception (Sabatinelli et al. Reference Sabatinelli, Fortune, Li, Siddiqui, Krafft, Oliver, Beck and Jeffries2011). However, CBT response was predicted by less, not more, higher-order visual activity to emotional faces as hypothesized. Furthermore, results regarding secondary visual processes were limited to the ITG as opposed to a broader network of areas (e.g. dorsal and ventral occipitotemporal regions) observed in other studies (Doehrmann et al. Reference Doehrmann, Ghosh, Polli, Reynolds, Horn, Keshavan, Triantafyllou, Saygin, Whitfield-Gabrieli, Hofmann, Pollack and Gabrieli2013; Klumpp et al. Reference Klumpp, Fitzgerald and Phan2013a ). In our paradigm ‘match faces’ is contrasted with ‘match shapes’ as opposed to a non-cognitive ‘baseline’ (e.g. fixation). By introducing an attentional control condition, perceptual assessment of emotional faces may not robustly elicit activity related to secondary visual areas. The higher-level visual region that did emerge indicates less activity, possibly reflective of less attentional deployment to emotional faces portends CBT response. Findings are consistent with the interpretation that CBT success might be predicted by less vigilance for relevant signals, though our study design does not permit dissociation between mechanisms that mediate attention from emotion regulation.
Symptom improvement was also predicted by a negative relationship between CBT response and activity to faces versus shapes in the superior temporal pole, a region associated with higher-level recognition (Olson et al. Reference Olson, Plotzker and Ezzyat2007); and the precentral gyrus, pallidum, caudate and supplementary motor area, regions involved in the preparation and regulation of movement (Alexander et al. Reference Alexander, DeLong and Strick1986; Rektor, Reference Rektor2000; Simon et al. Reference Simon, Meunier, Piettre, Berardi, Segebarth and Boussaoud2002). These preliminary, exploratory results suggest that symptom improvement positively corresponded with less engagement with emotional faces.
Together, preliminary results indicate that CBT success was modulated by prefrontal–limbic regions. Namely, improvement was predicted by greater pre-treatment dorsal prefrontal activity (dorsal ACC, dmPFC) during attentional control, less amygdala reactivity during emotion processing, and/or greater activity in the medial orbital gyrus during emotion perception. Findings suggest that CBT may be mediated by intact implicit top-down regulation and reduced reactivity, whether attention is directed toward or away from salient stimuli, or mechanisms associated with dysfunctional strategic regulation when confronting emotional faces.
Limitations
Our study is not without important limitations. First, there was no baseline (e.g. fixation) condition; therefore findings cannot be interpreted in relation to a non-cognitive and non-emotional task. Second, no ‘neutral’ target expressions were possible with the present paradigm, which did not permit dissociation between face and emotion-processing influences. Third, two of the 21 participants with gSAD were taking bupropion; even though the medication was stable before entering the study and remained unchanged during the study, any influence it may have had on results cannot be ruled out. Fourth, the small sample size and lack of a waitlist group to serve as a control for changes in symptoms unrelated to treatment reduces our ability to draw firm conclusions about brain markers of CBT response. Fifth, the exploratory nature of the findings and lack of independent evaluators of treatment fidelity and symptom change warrant replication and further investigation. Sixth, findings are based at the group-, as opposed to single-subject, level of analysis, thus reducing the clinical utility of using fMRI data to predict who specifically will be likely to respond to treatment. Lastly, results cannot be generalized to other anxiety disorders or to other treatments such as pharmacological interventions also proven to be effective in treating gSAD. Future studies are needed to determine if the brain predictors observed here are specific to CBT or shared across any therapeutic modality as long as the treatment is effective.
Conclusions
Pre-treatment activity in prefrontal and subcortical regions may serve as brain predictors of CBT response in individuals with gSAD. Findings indicate that improvement following CBT pertained to enhanced dorsal prefrontal activity in the presence of emotional distractors, reduced amygdala reactivity to emotional faces and/or greater activity in the medial orbital gyrus to emotional faces. The observation that neural predictors were modulated by attentional control and emotion processing indicates that probes of attentional control should be considered when evaluating brain markers. Future studies that employ a randomized placebo-controlled and/or comparative active treatment designs and larger samples are needed to determine whether CBT effects are mediated by these brain predictors to better delineate the mechanisms of therapeutic actions of CBT and other effective treatments and predictors of treatment response.
Acknowledgements
This work was supported by grants from the National Institutes of Health, National Institute of Mental Health (no. MH076198 to K.L.P. and MH093679 to H.K.).
Declaration of Interest
None.