


Introduction
Head and neck cancer is a common malignancy in Indian men.Reference Ferlay, Soerjomataram, Ervik, Dikshit, Eser and Mathers1 In developing countries, approximately 80 per cent of head and neck cancer patients present with an advanced stage tumour (III and IV).Reference Mohanti, Nachiappan, Pandey, Sharma, Bahadur and Thakar2 The standard treatment for locally advanced head and neck cancer generally comprises either surgery followed by adjuvant radiotherapy, concurrent chemoradiotherapy or radiotherapy alone, depending on the tumour stage, tumour site, performance status and patient preference.Reference Pignon, le Maître, Maillard and Bourhis3 This combined modality treatment approach may lead to multiple complications, such as absence of a cough reflex, swallowing disorder and xerostomia, which may in turn lead to aspiration during or after treatment.Reference Batth, Caudell and Chen4 In clinical practice, many subtle aspiration events may pass unnoticed in the early stages, eventually leading to sepsis or respiratory failure.Reference Nguyen, Frank, Moltz, Vos, Smith and Bhamidipati5, Reference Stenson, Mccracken, List, Haraf, Brockstein and Weichselbaum6 Therefore, it is very important to select high-risk patients for early rehabilitation procedures to decrease the morbidity and mortality associated with aspiration pneumonia.
The current retrospective analysis aimed to estimate the prevalence of aspiration pneumonia in head and neck cancer patients, and to identify the risk factors associated with this disease. This study is the first of its kind from the Indian subcontinent. It may guide us to select head and neck cancer patients at a high risk of aspiration pneumonia for prompt management, thus avoiding fatal outcomes.
Materials and methods
Hospital death records from 2000–2012 were reviewed to obtain the number of patient deaths and retrieve treatment files. Eighty-five patients with head and neck cancer (at all subsites and stages) who died in the hospital during this period were identified. Records of these patients were analysed for treatment details and the cause of death (stated on the death certificate, as completed by the senior resident on duty and countersigned by the consultant on call). The study fully complied with our institutional ethical standards and with the Helsinki Declaration of 1975, as revised in 2008. The impact of factors such as age, sex, tumour stage, tumour site, treatment modality (surgery vs chemoradiation), baseline swallowing capacity, intent of treatment, co-morbidities and history of smoking were analysed using chi-square and Fisher's exact tests. Both univariate and multivariate analyses were performed to investigate the statistical significance of these prognostic factors. Stata 11.1 software (StataCorp, College Station, Texas, USA) was used for the statistical analysis.
Results
Patient demographics
A total of 85 head and neck cancer patients who died at the hospital during the study period were identified. The median (± standard deviation) patient age at the time of diagnosis was 51.2 ± 16.9 years, with a male-to-female ratio of 6:1. Overall, 18 patients (21 per cent) had medical co-morbidities including diabetes, hypertension or tuberculosis. Fifty-seven (67 per cent) patients were known to be smokers. The distribution of primary tumour site and tumour stage in the study cohort is shown in Table I.
Table I Patient demographics

SD = Standard deviation
Patient signs and symptoms before death
In our study, the most prevalent symptoms before death were decreased swallowing capacity (52 out of 85), combined shortness of breath and dysphagia (41 out of 85), shortness of breath alone (14 out of 85) and dysphagia alone (8 out of 85). In 22 patients, specific symptoms could not be ascertained. Significant weight loss (of more than 10 per cent in the last six months) was noted in 49 patients. Chest X-rays (CXRs) showed evidence of aspiration pneumonitis in 31 patients. Patchy consolidation was visible in five patients, while CXR findings were completely normal in six patients (Table II).
Table II Symptom burden before death
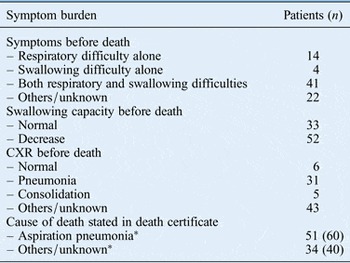
*Data represent n (%). CXR = chest X-ray
Treatment details and toxicities
The treatment intent was curative in 75 patients (surgery followed by post-operative radiotherapy and/or chemoradiotherapy, concurrent chemoradiotherapy and radiotherapy alone in 19, 38 and 28 patients respectively). Palliative treatment was planned for 10 patients (Table III). In most patients, radiotherapy was delivered using a two-dimensional simulator-based technique. A three-dimensional computed tomography based technique or intensity modulated radiotherapy was used for 14 patients.
Table III Treatment details

Grade 3 or above toxicity occurred in 25 patients. Nasogastric tube feeding was required for 37 patients, while 3 patients were offered nutrition via a feeding jejunostomy tube. Four patients underwent elective tracheostomy. Treatment was interrupted in 10 patients due to treatment-related toxicity (median delay of 10.4 days). Hospital admission was required for 49 patients (for treatment-induced toxicity in 39 patients and disease progression in 10 patients).
Prognostic factors
According to the death certificates, aspiration pneumonia was the primary cause of death in 51 out of 85 patients (60 per cent). Pharyngeal primary tumours (oropharynx and hypopharynx) and advanced tumour stage had significantly negative impacts on aspiration pneumonia related deaths (p = 0.02 for both). The intent of treatment (curative vs palliative) had a borderline significant effect (p = 0.05) on the outcome (Table IV). In a multivariate analysis, the primary tumour site (odds ratio 3.3, 95 per cent confidence interval (CI) 1.17–9.4, p = 0.05) and stage (odds ratio 4.2, 95 per cent CI 1.16–15.61, p = 0.05) retained a borderline significant impact on deaths attributable to aspiration pneumonia (Table V).
Table IV Association of various factors and aspiration pneumonia
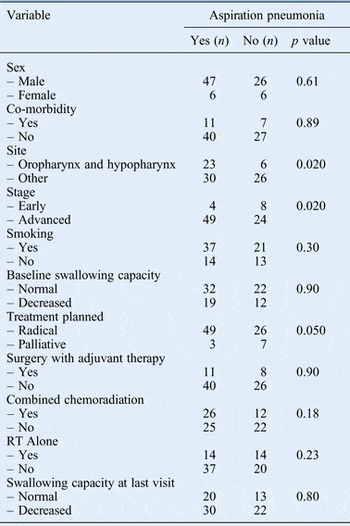
Table V Odds ratio and 95% CI after multivariate analysis

S no = Serial number; CI = confidence interval; Opx = oropharynx; Hpx = hypopharynx
Discussion
Aspiration is defined as inhalation of the oropharyngeal or gastric contents into the larynx or lower respiratory tract.Reference Russi, Corvò, Merlotti, Alterio, Franco and Pergolizzi7 Inhalation of small amounts of oropharyngeal secretions is common during sleep in healthy individuals. A low burden of virulent bacteria in normal pharyngeal secretions, the cough reflex, active ciliary transport and immune mechanisms lead to the clearance of infective material, often without any sequelae.Reference Marik8 However, any condition which increases the bacterial burden of pharyngeal secretions in a person with an impaired defence mechanism may lead to aspiration pneumonia.
Aspiration pneumonia is alleged to be a significant cause of morbidity and mortality amongst head and neck cancer patients.Reference Nguyen, Frank, Moltz, Vos, Smith and Bhamidipati5 It has been found to affect patients with primary tumours at all sites, irrespective of disease stage. Although aspiration events are mostly under-detected and underestimated, the reported rates range from 33 per cent to 81 per cent following initiation of chemoradiotherapy for head and neck cancer. Langerman et al. reported a predominance of aspiration in laryngeal carcinoma patients, followed by hypopharyngeal carcinoma patients.Reference Langerman, Maccracken, Kasza, Haraf, Vokes and Stenson9 Swallowing dysfunction prior to treatment can increase the probability of aspiration pneumonia due to chemoradiation, which negatively influences the prognosis for head and neck cancer patients. A Scandinavian study reported the incidence of aspiration pneumonia as 5.3 per cent (95 per cent CI 3.1–8.3 per cent) in the first year after radiotherapy.Reference Mortensen, Jensen and Grau10
Various studies have attempted to identify the risk factors and aetiology of aspiration. In one of these, Jung et al. showed that advanced age, higher tumour stage, and a history of surgery, chemotherapy and radiotherapy were significantly associated with aspiration.Reference Jung, Kim and Joo11 In the current study, oropharyngeal and hypopharyngeal cancer sites and advanced disease stage were found to be important risk factors for developing aspiration pneumonia.
Although palliative intent of treatment was also a risk factor for developing aspiration pneumonia, it did not reach statistical significance. Patients with a poor performance status and heavy disease burden are often selected for palliative therapy, which might have confounded the association. Our study, however, did not show any correlation between chemoradiation and the risk of developing aspiration, in contrast to a previous study.Reference Kotz, Costello, Li and Posner12
A comprehensive swallowing evaluation supplemented by either a video-fluoroscopic swallow or fibre-optic endoscopic evaluation and a modified barium swallow is the ‘gold standard’ for identifying patients at a high risk of aspiration pneumonia.Reference Langmore, Schatz and Olson13 Smith et al. reported severe swallowing dysfunction in the base of the tongue, larynx and pharyngeal muscles by video-fluoroscopic swallow after chemoradiation; this may lead to bolus stasis, residue in the vallecula, impaired mobility of the epiglottis and, finally, aspiration pneumonia.Reference Smith, Kotz, Beitler and Wadler14 Various other video-fluoroscopic swallow studies have shown that a delayed swallowing reflex and reduced laryngeal elevation might be risk factors for aspiration. Modified barium swallow findings for head and neck cancer patients who received concurrent chemoradiation was first reported by Nguyen et al.Reference Nguyen, Smith, Dutta, Alfieri, North and Nguyen15 They noted that 13 per cent (15 out of 144) of patients develop aspiration during chemoradiation. A CXR was diagnostic in nine patients, while the combined use of CXR and a modified barium swallow enhances the diagnostic accuracy to 80 per cent.
In a developing country such as India, the burden of head and neck cancer is so high that it is not cost-effective to assess swallowing using video-fluoroscopic swallow or modified barium swallow evaluation for every patient. Instead, behavioural, dietary and medical strategies, and the institution of feeding manoeuvres to reduce the risk of aspiration may be more cost-effective ways to reduce the incidence of aspiration pneumonia. However, studies like this one will help to establish a role for judicious utilisation of video-fluoroscopic swallow and modified barium swallow analysis in the early detection of aspiration pneumonia in patients with advanced stage (III–IVb) pharyngeal primary tumours, especially those intended to undergo curative anticancer therapy. Special attention should be given to patients having swallowing dysfunction and compensatory feeding strategies should be taught from the onset of anticancer therapy.
• Aspiration pneumonia causes morbidity and mortality in head and neck cancer patients
• Pharyngeal (oropharyngeal and hypopharyngeal) tumours and advanced disease stage have negative impacts on aspiration pneumonia related mortality
• Early detection of high-risk patients is very important
• The selective use of swallow analysis in high-risk patients may be a cost-effective way to reduce the risk of aspiration pneumonia
Studies have been carried out to establish the impact of modern techniques such as intensity modulated radiation on aspiration pneumonia.Reference Hunter, Lee, Lyden, Haxer, Feng, Schipper, Worden, Prince, McLean, Wolf, Bradford, Chepeha and Eisbruch16 Even with such improved delivery techniques with better organ sparing, 16 patients out of a total cohort of 72 developed aspiration pneumonia in a prospective study. Further studies with long-term follow up are necessary to visualise the impact of these high yield techniques on aspiration pneumonia. No effect of intensity modulated radiotherapy was seen in the study by Mortensen et al.Reference Russi, Corvò, Merlotti, Alterio, Franco and Pergolizzi7
In this study, we observed aspiration pneumonia to be a significant contributory factor to mortality in patients with oropharynx and hypopharynx primary tumours and advanced disease stages. These two subsites (oropharynx and hypopharynx) were considered together because of low patient numbers. Intent of treatment (curative vs palliative) also had a borderline significant effect on outcome.
This retrospective analysis aimed to draw attention to aspiration pneumonia, which often goes unnoticed and neglected. However, it had many drawbacks. For example, only hospital-based death records were considered and deaths outside the hospital were not. Although efforts have been made to eliminate bias related to different definitions of aspiration, the lack of use of modified barium swallow and video-fluoroscopic swallow evaluations was a major drawback of the current study.





