



Conduct disorder (CD) is a diagnosis given to minors who engage in extreme and persistent antisocial behavior (American Psychiatric Association, 2013). Youths with CD and high levels of callous and unemotional (CU) traits (e.g., low empathy and remorse) usually have more severe CD (CD/HCU) than those with low levels of CU traits (CD/LCU; Frick, Stickle, Dandreaux, Farrell, & Kimonis, Reference Frick, Stickle, Dandreaux, Farrell and Kimonis2005). Furthermore, CD/HCU is considered a developmental precursor of psychopathy due to their similar characteristics (Blair, Reference Blair2013). Consequently, CD/HCU and CD/LCU are now recognized as distinct subtypes of CD (American Psychiatric Association, 2013). Researchers have posited different developmental pathways to CD/HCU and CD/LCU, with CD/HCU having a stronger genetic component and CD/LCU a stronger environmental component (e.g., Viding, Blair, Moffitt, & Plomin, Reference Viding, Blair, Moffitt and Plomin2005). CU traits themselves are between 36% and 67% heritable, according to a recent estimate (Moore, Blair, Hettema, & Roberson-Nay, Reference Moore, Blair, Hettema and Roberson-Nay2019). In line with this, early research suggested that ineffective parenting was associated with conduct problems only in youths with low levels of CU traits; those with high levels of CU traits tended to exhibit conduct problems regardless of parenting quality (Wootton, Frick, Shelton, & Silverthorn, Reference Wootton, Frick, Shelton and Silverthorn1997). However, there is a growing consensus that parenting plays a role in the development of both CD/HCU and CD/LCU, even if this role is not yet well understood (Waller, Gardner, & Hyde, Reference Waller, Gardner and Hyde2013). Here, we investigated the extent to which various dimensions of positive and negative parenting (parental involvement, positive reinforcement, poor supervision, inconsistent discipline, and corporal punishment) are associated with CD/HCU and CD/LCU. In addition to investigating differences at the group level, we also investigated differences at the individual level, using a multivariate classification approach. Specifically, we trained classifiers to distinguish between CD/HCU, CD/LCU, and typical development (TD) using multiple measures of parenting, thus estimating the relevance of these different facets for determining the “diagnostic” status of individual youths.
Positive Parenting as a Protective Factor Against the Development of CU Traits
Positive parenting includes high levels of interest and involvement with the child, emotional warmth, and positive reinforcement of prosocial and other desirable behavior. These characteristics are thought to promote empathy development and moral conscience in young children (Kochanska, Forman, Aksan, & Dunbar, Reference Kochanska, Forman, Aksan and Dunbar2005). Several recent, large-scale adoption studies provide compelling evidence that positive parenting is associated with reductions in CU-type behavior in high-risk toddlers. Hyde et al. (Reference Hyde, Waller, Trentacosta, Shaw, Neiderhiser, Ganiban and Leve2016) collected observational and questionnaire data from 561 adopted children and parents at 18 and 27 months. Antisocial behavior of the biological mother predicted CU-type behavior in the child at 27 months, suggesting an inherited genetic risk for CU traits. However, positive parenting by the adoptive parents (observed during a 3-min clean-up task at 18 months) buffered this inherited risk. In the same sample, Waller et al. (Reference Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Hyde2016) likewise demonstrated that fearlessness in biological mothers predicted CU-type behavior in their children, but this pathway was moderated by positive adoptive parenting, such that no association existed for children with above mean levels of positive parenting (although there was no moderation for a low affiliative behavior to CU pathway). Likewise, in toddlers aged 2–3 years, Waller et al. (Reference Waller, Gardner, Viding, Shaw, Dishion, Wilson and Hyde2014) found evidence that warm positive parenting was associated with later reductions in CU-type behaviors. In a separate longitudinal sample of boys aged 18 months to 12 years, Waller, Shaw, and Hyde (Reference Waller, Shaw and Hyde2017) found that fearless temperament at 24 months (a risk factor for CU traits) was associated with CU-type behavior at 10–12 years, but only in boys who experienced low levels of positive parenting. The interaction between positive parenting and fearlessness also predicted CU-type behavior at 10–12 years, via earlier CU-type behavior at 42 months. As further evidence for its protective role, a positive parenting intervention has demonstrated some success with at-risk preschoolers, promoting techniques such as effective discipline, positive reinforcement, and promotion of good behavior through storytelling (Elizur & Somech, Reference Elizur and Somech2018).
Positive parenting has also been associated with a reduction in CU traits in older children (Muratori et al., Reference Muratori, Lochman, Lai, Milone, Nocentini, Pisano and Masi2016; Pardini, Lochman, & Powell, Reference Pardini, Lochman and Powell2007). A genetically informed, population-representative study of children aged 6–11 years demonstrated that while parental harshness was associated with both aggression and CU traits, low parental warmth was uniquely associated with CU traits (Waller, Hyde, Klump & Burt, Reference Waller, Hyde, Klump and Burt2018). Finally, in a longitudinal study of 660 twin pairs followed from birth onward, Henry et al. (Reference Henry, Dionne, Viding, Vitaro, Brendgen, Tremblay and Boivin2018) demonstrated that CU traits were less heritable in children who experienced high levels of warm and rewarding parenting. It should be noted, however, that associations between positive parenting and CU traits are likely bidirectional, with child temperament influencing parenting practices as well as vice versa (e.g., Hawes, Dadds, Frost, & Hasking, Reference Hawes, Dadds, Frost and Hasking2011; Larsson, Viding, & Plomin, Reference Larsson, Viding and Plomin2008; Muñoz, Pakalniskiene, & Frick, Reference Muñoz, Pakalniskiene and Frick2011; Pardini et al., Reference Pardini, Lochman and Powell2007; Pisano et al., Reference Pisano, Muratori, Gorga, Levantini, Iuliano, Catone and Masi2017). Nonetheless, there is good evidence to suggest that positive parenting inhibits the development of CU traits in high-risk children, especially during early childhood.
Negative Parenting as a Risk Factor for the Development of CU Traits
Negative parenting includes harsh and inconsistent discipline, and is a common feature of the parenting environment in both CD/HCU and CD/LCU (e.g., Fontaine, McCrory, Boivin, Moffitt, & Viding, Reference Fontaine, McCrory, Boivin, Moffitt and Viding2011; but cf. Enebrink, Andershed, & Langstrom, Reference Enebrink, Andershed and Långström2005). Although less than for positive parenting, there is some evidence that negative parenting in young children is associated with the development of CU traits. As previously described (Waller et al., Reference Waller, Hyde, Klump and Burt2018) harsh parenting was associated with both aggression and CU traits in 6- to 10-year-old children. In addition, in a study of 561 adopted children from 18 to 54 months, Trentacosta et al. (Reference Trentacosta, Waller, Neiderhiser, Shaw, Natsuaki, Ganiban and Hyde2019) reported that while CU-type behaviors predicted later harsh parenting, harsh parenting in turn predicted later CU-type behaviors. Furthermore, there was an interaction with inherited risk for CU traits, such that these bidirectional effects were strongest for high-risk children. Of note, even more so than for positive parenting, there is strong evidence that negative parenting and CU traits have bidirectional relationships (Flom, White, Ganiban, & Saudino, Reference Flom, White, Ganiban and Saudino2019; Hawes et al., Reference Hawes, Dadds, Frost and Hasking2011; Larsson et al., Reference Larsson, Viding and Plomin2008; Muñoz et al., Reference Muñoz, Pakalniskiene and Frick2011; Pardini et al., Reference Pardini, Lochman and Powell2007; Pisano et al., Reference Pisano, Muratori, Gorga, Levantini, Iuliano, Catone and Masi2017). In summary, there is evidence that both positive and negative parenting drive increases in CU traits in young children, as well as vice versa. At present, however, there is slightly more evidence for positive parenting driving changes in CU traits than for negative parenting driving these changes.
Associations Between Parenting and Conduct Problems in CD/HCU and CD/LCU
While there is now good evidence that positive and negative parenting are associated with the expression of CU traits in young children, it is less clear how CU traits moderate the relationships between these dimensions of parenting and conduct problems. This is especially true in older children with clinically significant conduct problems, that is, CD/HCU and CD/LCU. Following Wootton et al.'s seminal study (Reference Wootton, Frick, Shelton and Silverthorn1997), a number of studies have investigated the moderating role of CU traits in the relationship between parenting and conduct problems. In a mixed-sex sample of second and third graders, Oxford, Cavell, and Hughes (Reference Oxford, Cavell and Hughes2003) demonstrated an interaction between a continuous measure of CU traits and ineffective (i.e., high negative and low positive) parenting when predicting conduct problems. Partially replicating the findings of Wootton et al., ineffective parenting was associated with conduct problems only in children with lower CU scores. By contrast, the same authors found only weak evidence for an interaction when using a dichotomous measure of CU traits. Both Wootton et al. and Oxford et al. used broad, composite measures of ineffective parenting, which included both positive and negative dimensions. Oxford et al.'s composite measure was weighted toward negative parenting, and a similar interaction (between negative parenting and the affective dimension of psychopathy) was observed in a study that focused exclusively on harsh and inconsistent discipline in young offenders (Edens, Skop, & Cahill, Reference Edens, Skopp and Cahill2008). It has been hypothesized that youths with high levels of CU traits are insensitive to negative parenting because they are insensitive to punishment more generally (Blair, Colledge, & Mitchell, Reference Blair, Colledge and Mitchell2001; Dadds & Salmon, Reference Dadds and Salmon2003). However, these findings are not unanimous across the literature; for example, in 6- to 9-year-old children, Falk and Lee (Reference Falk and Lee2012) found no evidence for interactions between CU traits and corporal punishment when predicting various measures of conduct problems. One study even reported a stronger association between negative parenting and CD severity at high levels of CU traits, although this pattern was not consistent across different measures of antisocial behavior (Crum, Waschbusch, Bagner, & Coxe, Reference Crum, Waschbusch, Bagner and Coxe2015).
This picture of insensitivity to parenting in CD/HCU becomes even less clear when the distinction between positive and negative parenting is explicitly made. For example, in a sample of 4- to 12-year-old clinic-referred boys, coercive parenting was a stronger predictor of conduct problems in boys with low levels of CU traits than in those with high levels of CU traits, while parental warmth was a stronger (negative) predictor of conduct problems in boys with high levels of CU traits (Pasalich, Dadds, Hawes, & Brennan, Reference Pasalich, Dadds, Hawes and Brennan2011). This study focused specifically on the affective quality of the parent–child relationship (warmth versus coercion) rather than on goal-directed parenting behaviors such as discipline and reinforcement. Somewhat similarly, Ray et al. (Reference Ray, Frick, Thornton, Wall Myers, Steinberg and Cauffman2017) demonstrated that an association between CU traits and delinquent peer association, which led to offending, was weaker in adolescents with high levels of parental warmth and supervision. By contrast, Falk and Lee (Reference Falk and Lee2012) defined positive parenting as parental involvement and positive reinforcement (a more goal-directed measure) and reported an interaction with CU traits, such that positive parenting was associated with fewer conduct problems only in children with low or average levels of CU traits. It is interesting to note that these goal-directed measures of positive parenting evidenced interactions with CU traits that were more in line with previous findings relating to negative parenting, suggesting that positive parenting is not a unitary concept and that affective warmth is somewhat distinct from goal-directed positive parenting. In summary, there is a tendency––albeit not fully consistent––for negative parenting to be less strongly associated with conduct problems at higher levels of CU traits, perhaps due to punishment insensitivity (Dadds & Salmon, Reference Dadds and Salmon2003). By contrast, positive parenting is generally inversely associated with conduct problem severity even at higher levels of CU traits, although this finding is most consistent when focusing on parental warmth rather than the more goal-directed positive parenting behaviors.
Advantages of a Machine Learning Classification Approach
While traditional statistical techniques are appropriate for investigating average differences between groups, or associations between continuous variables, they provide little indication of the relevance of these variables for distinguishing between individuals. A classification approach can address this gap in two ways. First, the performance of a classifier indicates how accurately youths with CD/HCU, youths with CD/LCU, and TD youths can be distinguished from each other, using a holistic measure of parenting (i.e., all parenting dimensions considered together in a multivariate fashion). This is important because, regardless of their effect size or statistical significance, it is of practical importance to know whether these univariate group-level differences translate into reliable individual differences. Second, the classifier used here––Angle-based Generalized Matrix Learning Vector Quantization (Angle-GMLVQ)––quantifies the relevance of each dimension of parenting to the classifier (Bunte, Baranowski, Arlt, & Tino, Reference Bunte, Baranowski, Arlt and Tino2016). Because the classifier is multivariate, these relevance scores reflect the importance of each parenting dimension while accounting for all other dimensions simultaneously. In doing so, it provides information that is neither intuitively obvious nor easily quantifiable from traditional univariate analyses.
Summary and Hypotheses
In summary, low levels of positive parenting (and to a slightly lesser extent, negative parenting) are bidirectionally associated with the development of CU traits in young children. However, there is also some evidence that in youths with CD/HCU, as opposed to CD/LCU, negative parenting is not associated with CD severity. By contrast, this moderating role of CU traits occurs less frequently for positive parenting (but see Falk & Lee, Reference Falk and Lee2012). Here, we addressed two questions regarding the associations between parenting, CD/HCU, and CD/LCU. First, using a traditional univariate approach, we investigated whether youths with CD/HCU, youths with CD/LCU, and TD youths differed, on average, in their exposure to various dimensions of positive and negative parenting practices. Second, using a classification approach, we investigated the utility of these differences for determining the diagnoses of individuals within each group (i.e., CD/HCU, CD/LCU, or TD). Angle-GMLVQ has an advantage over more common classifiers in that it provides a relevance score for each feature (variable) in the model, enabling features to be ranked by their contribution to successful classification. In addition, in contrast to most classifiers, Angle-GMLVQ is sensitive to relative differences between features (i.e., scores on different types of parenting behavior) rather than the absolute magnitude of feature scores. It should thus perform well when individuals are characterized by different patterns of parenting, while minimizing the effect of subjective, idiosyncratic tendencies of participants to give uniformly high or low ratings across items.Footnote 1
Given previous findings (e.g., Waller et al., Reference Waller, Hyde, Klump and Burt2018), we hypothesized that youths with CD/HCU would be characterized by low levels of positive parenting as well as high levels of negative parenting, while youths with CD/LCU would be characterized mainly by high levels of negative parenting. Similarly, we predicted that parenting behaviors would distinguish both youths with CD/HCU and youths with CD/LCU from TD youths at above chance levels in Angle-GMLVQ analyses. Next, we predicted that if youths with CD/HCU do experience lower levels of positive parenting as well as similar (or higher) levels of negative parenting compared to those with CD/LCU, then these groups too would be distinguished at above-chance levels in classification analyses. As a further test of the same hypothesis, we constructed a CD-against-TD classifier (without distinguishing between CD/HCU and CD/LCU, i.e., a Mixed-TD model) and compared its performance with the CD/HCU-against-TD (HCU-TD) and CD/LCU-against-TD (LCU-TD) classifiers. If youths with CD/HCU and youths with CD/LCU experience qualitatively distinct patterns of parenting as outlined above, then both of these classifiers should outperform the Mixed-TD model. Finally, in line with expected group differences, we predicted that both positive and negative parenting behaviors would be relevant for the HCU-TD model, negative parenting would be more relevant for the LCU-TD model, and positive parenting would be more relevant for the HCU-LCU model. Our measures of parenting (parental involvement, positive reinforcement, poor supervision, inconsistent discipline, and corporal punishment) have generally been conceived of as goal directed, rather than directly representing the affective quality of the relationship (Pasalich et al., Reference Pasalich, Dadds, Hawes and Brennan2011). Consequently, we did not make specific hypotheses about the individual dimensions of positive and negative parenting and their associations with CD/HCU or CD/LCU.
Method
Recruitment and eligibility criteria
Data were drawn from the FemNAT-CD sample in November 2017 (Freitag et al., Reference Freitag, Konrad, Stadler, De Brito, Popma, Herpertz and Fairchild2018). Participants aged 9–18 years were recruited at 11 sites across Europe, from mainstream and special schools, youth and community groups, healthcare providers and mental health services, youth offending services, and by word of mouth. While many participants with CD were receiving treatment or special educational provision for behavioral problems, and TD youths were generally recruited from mainstream schools and community groups, this was not a requirement for inclusion in the study. Inclusion in either group was based solely on the outcome of a clinical interview (described below). Participants were excluded if they had a current or past diagnosis of autism, psychosis, neurological or genetic disorders, or learning disability with IQ below 70. TD participants were additionally required to have no current mental disorders and no history of externalizing disorders, bipolar disorder, or manic episodes. Participants received a small financial reimbursement, or equivalent in vouchers, as approved by the local ethics committees (see Kersten et al., Reference Kersten, Vriends, Steppan, Raschle, Praetzlich, Oldenhof and Martinelli2017). The full FemNAT-CD sample consisted of 1,743 participants in November 2017, of whom 756 were included in the present analyses. The procedure for selecting the final sample is described in detail below.
Questionnaire and interview measures
Schedule for Affective Disorders and Schizophrenia for School-Age Children: Present and Lifetime Version (K-SADS-PL)
The K-SADS-PL (Kaufman et al., Reference Kaufman, Birmaher, Brent, Rao, Flynn, Moreci and Ryan1997) was used to assess for CD and other disorders. The K-SADS-PL is a semistructured diagnostic interview used to assess current and past psychopathology in children and adolescents. The interview was administered separately to participants and parents by trained researchers, and combined parent and child summary ratings of all symptoms (past, present, and lifetime) were then generated. Where assessors gave discrepant ratings for a symptom, they discussed all available information until an agreement was reached for the summary rating. All diagnoses were generated based on the text-revised fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR; American Psychiatric Association, 2000) diagnostic criteria. Interrater reliability for current CD diagnoses was high (94.7% agreement across raters, Cohen's κ = .91). Assuming all other relevant eligibility criteria were met, youths with a K-SADS-PL CD diagnosis were assigned to the CD group, while those without were assigned to the TD group.
Wechsler Intelligence Scale (Wechsler Abbreviated Scale of Intelligence, Wechsler Adult Intelligence Scale, Wechsler Intelligence Scale for Children)
In English-speaking sites, IQ was estimated with the vocabulary and matrix reasoning subscales of the Wechsler Abbreviated Scale of Intelligence (Wechsler, Reference Wechsler1999). Other sites used the vocabulary, block design, and matrix reasoning tests of the Wechsler Intelligence Scale for Children (for participants aged 16 or under) or the Wechsler Adult Intelligence Scale (for participants aged 17–18 years; Wechsler, Reference Wechsler2008).
Alabama Parenting Questionnaire, child-report and parent-report versions (APQ)
The APQ (Essau, Sasagawa, & Frick, Reference Essau, Sasagawa and Frick2006a) is a 42-item measure of parenting, with separate subscales for maternal and paternal involvement (e.g., “You have a friendly talk with your mom”), positive parenting (e.g., “Your parents reward or give something extra to you for behaving well”), poor supervision (e.g., “You stay out in the evening past the time you are supposed to be home”), inconsistent discipline (e.g., “Your parents threaten to punish you and then do not do it”), and corporal punishment (e.g., “Your parents slap you when you have done something wrong”). Items are rated on a 5-point scale ranging from 1 (never) to 5 (always). In order to avoid confusion with the broader concept of positive parenting, we refer to the APQ positive parenting subscale as positive reinforcement hereafter. The parent-report APQ consists of the same subscales as the child-report version, except that maternal and paternal involvement are replaced by a single parental involvement subscale. For the current analyses, the more negative of the child and parent ratings for each item was taken as the summary item score, that is, the lower score on the positive parenting items and the higher score on the poor supervision and negative parenting items. For the parental involvement items, the higher score from the child-report maternal involvement and corresponding paternal involvement items was first taken, as this was assumed to reflect the involvement of the primary carer. The lower score from this and the parent-rated parental involvement item was then taken as the summary score. In line with previous studies, parental involvement and positive reinforcement subscales were used as measures of positive parenting. Inconsistent discipline and corporal punishment were used as measures of negative parenting, and poor supervision was treated as a distinct component (Molinuevo, Pardo, & Torrubia, Reference Molinuevo, Pardo and Torrubia2011; Muratori et al., Reference Muratori, Lochman, Lai, Milone, Nocentini, Pisano and Masi2016). Reliability was good for all subscales (Cronbach's αs: involvement α = .78, positive reinforcement α = .80, poor supervision α = .82, inconsistent discipline α = .65, and corporal punishment α = .77).
Inventory of Callous–Unemotional Traits, parent-report version (ICU)
The ICU (Essau, Sasagawa, & Frick, Reference Essau, Sasagawa and Frick2006b) is a 24-item questionnaire measure of CU traits in children and adolescents. There are three subscales (callous, uncaring, and unemotional) and a total score. Items are rated on a 4-point scale from 0 (not at all true) to 3 (definitely true). Reliability was good in the current sample (callous α = .88, uncaring α = .88, unemotional α = .78, and total α = .93).
Pubertal Development Scale (PDS)
The PDS (Petersen, Crockett, Richards, & Boxer, Reference Petersen, Crockett, Richards and Boxer1988) is a self-report measure of pubertal development. Items related to growth of body and facial hair, height, change of voice, and menstruation are rated on a scale from 1 (not yet started) to 4 (seems complete), and the participant is assigned to an overall category (prepubertal, early pubertal, midpubertal, late pubertal, or postpubertal). The response option 0 (I don't know) was removed shortly after data collection began, as its inclusion resulted in excessive amounts of missing data. PDS data were collected in addition to age in order to provide a fuller picture of maturity level.
Socioeconomic status (SES)
SES was assessed using a standard FemNAT-CD procedure, based on parental income, education, and occupation. Assessments were based on the International Standard Classification of Occupations (International Labour Organization, 2012) and the International Classification of Education (UNESCO, 2015). Human rater and computer-based ratings were combined into a factor score using principal component analysis. A clear one-dimensional structure underlying the different measures could be corroborated using confirmatory factor analysis (comparative fit index = .995; root mean square error of approximation = .035). Reliability of the composite SES score was acceptable (Cronbach's α =.74). In order to account for economic variation between countries, the final SES score was scaled and mean-centred within each country, thus providing a measure of relative SES.
Imputation of missing data
Missing data were imputed by statisticians at the Institute of Medical Biometry and Statistics, a member of the FemNAT-CD consortium. The procedure is described in the online-only Supplementary materials under “Imputation of Missing Data.”
Selection of participants from the larger FemNAT-CD sample
Of the 1,743 participants in the FemNAT-CD sample, 1 was excluded because it later emerged that this participant did not meet the eligibility criteria as described above, 67 were excluded due to missing data on CU traits, 14 for missing child-report data on parenting, 413 for missing parent-report data on parenting (i.e., these data could not be imputed), and 37 because they did not live with a parent or guardian. Participants with CD (as determined by the K-SADS clinical interview) were then assigned to CD/HCU and CD/LCU groups using a tertile split of the total ICU scores for the CD group (1st tertile cutoff score = 40, 3rd tertile cutoff = 30).Footnote 2 Participants with CD and scores in the 2nd tertile (n = 166) were excluded. TD participants with scores in the 1st tertile (n = 6) or the 2nd tertile (n = 36) were also excluded, on the grounds that youths with elevated CU traits are unlikely to be truly TD, even in the absence of a CD diagnosis (Rowe et al., Reference Rowe, Maughan, Moran, Ford, Briskman and Goodman2010). Next, 247 participants (TD n = 226, CD/LCU n = 21) were excluded so that groups were matched for site of data collection, number of males and females, mean age, and pubertal status (Match software; van Casteren & Davis, Reference van Casteren and Davis2007). This left a final sample of 756 participants (CD/HCU n = 164, 89 females; CD/LCU n = 164, 86 females; TD n = 428, 261 females). Finally, the “mixed” CD group (CD/mixed) was formed by combining the CD/HCU and CD/LCU groups (n = 328). The final sample differed significantly from the excluded participants on age and IQ; excluded participants were older, t (1741) = –5.64, p < .001, 2-tailed, partial η2 = .02, and had lower total IQ scores, t (1682) = 4.66, p < .001, 2-tailed, partial η2 =.01. There was also a greater proportion of females in the excluded participants, which reflected a deliberate strategy of oversampling females in the wider FemNAT-CD sample by a ratio of 2:1 (Freitag et al., Reference Freitag, Konrad, Stadler, De Brito, Popma, Herpertz and Fairchild2018; χ2 = 14.14, p <.001, φ = .09). Participants with CD in the final sample did not differ significantly from excluded participants with CD on CU trait scores or on current or lifetime maximum CD symptoms: CU score, t (566.63) = 1.65, p =.10, partial η2 = .004; current CD symptoms, t (745.23) = –1.22, p =.22, partial η2 = .002; lifetime CD symptoms, t (741.18) = –1.71, p =.09, partial η2 = .003.
Analysis
Univariate analyses
Group differences on parenting measures were assessed with one-way analyses of variance. Differences on other measures (e.g., CD symptoms and age) were assessed with one-way analyses of variance or chi square tests as appropriate. Correlations between CD symptoms, CU traits, and the five dimensions of parenting are also presented in the online-only Supplementary materials under “Correlations Between CD Symptoms, CU Traits, and Parenting.”
Classification models
Angle-GMLVQ is a prototype-based machine learning classifier. Angle-GMLVQ predicts class membership by positioning prototypes as class exemplars (i.e., representatives). It then assigns each data point to the class of the most similar prototype. Here, the similarity between a data point and a class prototype is quantified through their angle. In line with other machine learning classifiers, Angle-GMLVQ is a multivariate technique, which makes it more sensitive than univariate techniques to complex differences between groups. Angle-GMLVQ has the additional advantage that it provides information on the relevance of each feature (i.e., variable) to the model. Because the aim was to generate feature relevance scores that distinguish between specific groups, models were created for each pair of groups of interest:
1. CD/mixed against TD (referred to hereafter as Mixed-TD)
2. CD/HCU against TD (HCU-TD)
3. CD/LCU against TD (LCU-TD)
4. CD/HCU against CD/LCU (HCU-LCU)
Training and testing procedure
The classifier was trained and tested for each model, with one prototype per class. Features were parenting scores on each of the five APQ subscales, after regressing out variance associated with IQ, sex, pubertal status, and site of data collection. (Information on family structure and SES was not available for the full sample, and thus was not controlled for in these analyses. However, we did repeat the classification analyses after controlling for SES where available; these results were similar to those for the main models and thus are not discussed further; see online-only Supplementary materials under “Repetition of Angle-GMLVQ Classification Analyses After Regressing Out Variance Associated With SES.”). Performance was assessed using a holdout design with an 80/20 training/testing split, repeated for 1,000 random subsamplings in order to ensure stability of the model. In each resampling, where classes were initially balanced, 80% of each class was selected at random. Where classes were imbalanced, the larger class was instead randomly downsampled to the size of the smaller class. Next, the selected data were partitioned into the training and testing sets before training and testing the model. Mean performance metrics across all resamplings were then compared between models.
Assessment of model performance
In each model, the CD group was defined as the positive class and TD as the negative class. In the HCU-LCU model, the CD/HCU group was the positive class. True refers to correct classifications and false refers to incorrect classifications; hence, true positives are correctly classified members of the positive class, false positives are incorrectly classified members of the negative class, and so on (TP = true positives, FP = false positives, TN = true negatives, and FN = false negatives). Overall model performance was judged by classification accuracy (i.e., proportion of all participants classified correctly, or [TN + TP] / [TN + TP + FN + FP]). Confidence in positive and negative classifications was assessed with the positive predictive value (PPV) and the negative predictive value (NPV), respectively. PPV is the number of true positives as a proportion of all positive classifications (TP / [TP + FP]), while NPV is the number of true negatives as a proportion of all negative classifications (TN / [TN + FN]). The ability of the classifier to detect members of the positive and negative classes was assessed using the true positive rate (TPR; also known as sensitivity) and true negative rate (TNR; also known as specificity), respectively. TPR is the number of true positives as a proportion of all genuine positives, that is, the proportion of CD (or CD/HCU) participants who are classified correctly (TP / [TP + FN]). Similarly, TNR is the number of true negatives as a proportion of all genuine negatives (TN / [TN + FP]). Because accuracy can be misleading when class sizes are imbalanced, we used macroaveraged classification error rate (MCER) as the main measure of overall performance. MCER is the (unweighted) average of the error rates for each class, adapted from Fouad and Tino (Reference Fouad and Tino2012). MCER is therefore more meaningful than accuracy as a measure of performance when class sizes are imbalanced.
Assessment of feature relevance
Relevance scores were considered high if they were in the top 20% of scores across all resamplings with a corresponding classification MCER of 0.40 or below. Features were ranked by number of high scores. Note that relevance scores were normalized for each resampling, so that direct comparisons could be made across resamplings.
Results
Sample characteristics
There were no differences between the CD/HCU, CD/LCU, and TD groups in the proportion of participants included from each site (χ2 = 24.68, p =.21, φ = .21), nor in the proportion of females, mean age, or pubertal status (see Table 1). In the main analyses, males and females were not separated. However, we also investigated Sex × Group interactions; these are reported in detail in the online-only Supplementary materials under “Sex Differences.”Footnote 3 The CD/HCU and CD/LCU groups did not differ from each other on performance, verbal, or total IQ scores, but both had significantly lower IQ scores than the TD group. The same was true for SES (Table 1). As expected, the CD/HCU group had significantly more CD symptoms than the CD/LCU group, as well as more oppositional defiant disorder and attention-deficit/hyperactivity disorder symptoms, although these groups did not differ significantly in the proportion of childhood versus adolescent onset cases (Table 1). Information on family composition is displayed in Table 2. Although youths living independently were excluded, information on caregivers living in the household was only available for a subset of the full sample (information available for female carer: CD/HCU: 119, CD/LCU: 127, TD: 414. Male carer: CD/HCU: 91, CD/LCU: 91, TD: 336).
Table 1. Demographic and clinical characteristics (mean [95% confidence intervals of the mean] unless stated otherwise)
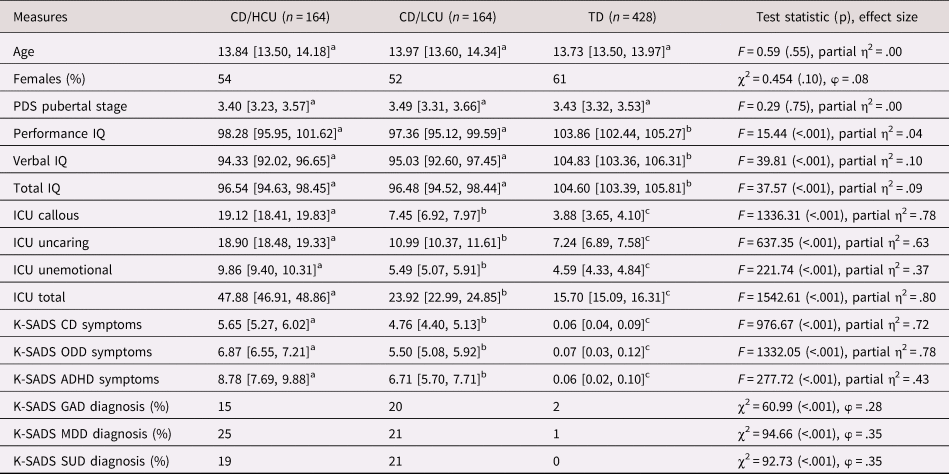
Notes: Groups with different superscript indices differ significantly in post hoc comparisons (p < .05, Bonferroni corrected). CD, conduct disorder. CD/HCU, conduct disorder with high levels of callous–unemotional traits. CD/LCU, conduct disorder with low levels of callous–unemotional traits. TD, typically developing. K-SADS, Schedule for Affective Disorders and Schizophrenia for School-age Children: Present and Lifetime Version (lifetime maximum symptoms/diagnosis). ODD, oppositional defiant disorder. ADHD, attention-deficit/hyperactivity disorder. GAD, generalized anxiety disorder. MDD, major depressive disorder. SUD, substance use disorder. PDS, Self-rating Scale for Pubertal Development. ICU, Inventory of Callous–Unemotional Traits.
Table 2. Caregivers living in family home (% of group)

Note: Participants who were not living with parents or caregivers were excluded, but information about caregivers was not available for the full sample. Significance tests reported in column 5 were conducted using only those with data concerning the relevant caregiver. CD/HCU, conduct disorder with high levels of callous–unemotional traits. CD/LCU, conduct disorder with low levels of callous–unemotional traits. TD, typically developing.
Group differences in parenting
Mean group differences for each APQ subscale are displayed in Table 3. Raw scores are displayed for ease of interpretation, but we indicate where the pattern of significant differences changed after regressing out variance associated with IQ, sex, pubertal status, site of data collection, and family structure. All three groups differed significantly on positive parenting, with the TD group scoring highest and the CD/HCU group scoring lowest for both involvement and positive reinforcement. Each group also differed significantly on poor supervision (it is interesting to note that the CD/LCU and TD groups no longer differed significantly on positive parenting after controlling for differences in family structure, although it should be noted that this information was not available for the full sample).Footnote 4 The CD/HCU and CD/LCU groups did not differ significantly on negative parenting, although both groups experienced significantly more negative parenting than the TD group. These group differences support the hypothesis that youths with CD/HCU are characterized by high negative and low positive parenting. However, the same was true for the CD/LCU group, although only positive parenting differed significantly between the CD/HCU and CD/LCU groups.
Table 3. Group differences in parenting (mean [95% confidence intervals of the mean])

Note: Groups with different superscript indices differ significantly in post hoc comparisons (p < .05, Bonferroni corrected). Regressing out variance associated with IQ, sex, pubertal status, and site of data collection did not change the pattern of significant group differences. Those marked with an asterisk represent groups that no longer differed significantly after regressing out variance associated with family structure in addition to IQ, sex, pubertal status, and site of data collection. CD/HCU, conduct disorder with high levels of callous–unemotional traits. CD/LCU, conduct disorder with low levels of callous–unemotional traits. TD, typically developing. APQ, Alabama Parenting Questionnaire.
Angle-GMLVQ classifier performance
Angle-GMLVQ model performance is shown in Table 4. All models performed significantly better than chance, as hypothesized (binomial tests, p < .001). The HCU-TD model demonstrated the best performance (MCER = 0.26), followed by the Mixed-TD model (MCER = 0.29) and then the LCU-TD model (MCER = 0.33). Although the HCU-LCU model was significantly above chance, it did not perform well (MCER = 0.42). This pattern of performance indicates considerable overlap in the parenting experiences of youths with CD/HCU and CD/LCU. Furthermore, performance for the LCU-TD model was significantly worse than for the Mixed-TD model, indicating that splitting the CD/mixed group into CD/HCU and CD/LCU groups was beneficial only to the CD/HCU group in terms of classifier performance. This reflects greater overlap between the CD/LCU and TD groups than between the CD/HCU and TD groups. Our final hypothesis––that both HCU-TD and LCU-TD classifiers would outperform the Mixed-TD classifier––was thus not supported.
Table 4. Angle-GMLVQ model performance (mean [95% confidence intervals of the mean])

Note: Groups with different superscript indices differ significantly in post hoc comparisons (p < .05, Bonferroni corrected). Note that the HCU-LCU model (column 6) was not included in statistical tests as comparisons between this and other models were not relevant to hypotheses. Mixed-TD, model classifying youths with conduct disorder with mixed levels of callous–unemotional traits and typically developing youths. HCU-TD, model classifying youths with conduct disorder with high levels of callous–unemotional traits and typically developing youths. LCU-TD, model classifying youths with conduct disorder and low levels of callous–unemotional traits and typically developing youths. PPV, positive predictive value. NPV, negative predictive value. TPR, true positive rate. TNR, true negative rate. MCER, macro-averaged classification error rate.
Feature relevance
Feature relevance scores for the HCU-TD, LCU-TD, and HCU-LCU models are displayed in Figure 1. The pattern of relevance scores generally supported our hypotheses, that is, that a combination of positive and negative parenting would be relevant to the HCU-TD model, negative parenting would be more relevant to the LCU-TD model, and positive parenting would be more relevant to the HCU-LCU model. The exception to this was positive reinforcement, which was consistently low in relevance across all models. Despite this, youths with CD/LCU were distinguished from TD youths almost entirely by negative parenting, and from youths with CD/HCU almost entirely by positive parenting and poor supervision.

Figure 1. Feature relevance for (a) HCU-TD, (b) LCU-TD, and (c) HCU-LCU models. Bars show percentage of resamplings in which feature relevance was in the top 20% of relevance scores across all resamplings with macro-averaged classification error rate ≤ 0.40.
Discussion
This study addressed differences in exposure to positive and negative parenting in youths with CD/HCU, youths with CD/LCU, and TD youths. We first investigated differences at the group level, hypothesizing that youths with CD/HCU would experience high levels of negative parenting and low levels of positive parenting relative to TD youths, while youths with CD/LCU would be characterized mainly by high levels of negative parenting. This hypothesis was partially supported, as youths with CD/LCU as well as those with CD/HCU experienced more negative and less positive parenting than TD youths (although only positive parenting differed significantly between the CD/HCU and CD/LCU groups). Next, we used Angle-GMLVQ classifiers to assess the extent to which positive and negative parenting was predictive of the diagnostic status of youths at the individual level. As predicted, all models performed at above chance levels. Contrary to our next hypothesis, splitting the CD/mixed group into CD/HCU and CD/LCU subtypes resulted in improved classification only for youths with CD/HCU. Finally, as hypothesized, both positive and negative parenting behaviors were highly relevant when distinguishing youths with CD/HCU from TD youths, while youths with CD/LCU were distinguished from TD youths almost exclusively by negative parenting and from youths with CD/HCU almost exclusively by higher positive parenting and lower levels of poor supervision.
Group-level differences in positive parenting
At the group level, youths with CD/HCU experienced significantly lower levels of parental involvement and positive reinforcement than youths with CD/LCU, who in turn experienced lower levels than TD youths. Thus, in terms of group-level differences, low positive parenting was more strongly associated with CD/HCU than with CD/LCU. These findings fit with previously observed associations between low positive parenting and CU traits (e.g., Waller et al., Reference Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Hyde2016). However, in the current sample, differences between the CD/LCU and TD groups were reduced to nonsignificance after controlling for family structure. This indicates that low levels of positive parenting might in part reflect caregiver absence, rather than parenting quality per se, and this distinction might be especially important for youths with CD/LCU. In this context, it is also interesting to note that poor supervision varied in line with positive parenting rather than negative parenting in the current sample.
Numerous studies have reported similar associations between low positive parenting and CD/HCU or CU traits (e.g., Elizur & Somech, Reference Elizur and Somech2018; Hyde et al., Reference Hyde, Waller, Trentacosta, Shaw, Neiderhiser, Ganiban and Leve2016; Muratori et al., Reference Muratori, Lochman, Lai, Milone, Nocentini, Pisano and Masi2016; Pardini et al., Reference Pardini, Lochman and Powell2007; Pasalich et al., Reference Pasalich, Dadds, Hawes and Brennan2011; Ray et al., Reference Ray, Frick, Thornton, Wall Myers, Steinberg and Cauffman2017; Waller et al., Reference Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Hyde2016, Reference Waller, Hyde, Klump and Burt2018; Waller, Shaw, & Hyde, Reference Waller, Shaw and Hyde2017; Waller, Shaw, Neiderhiser, et al., Reference Waller, Shaw, Neiderhiser, Ganiban, Natsuaki, Reiss and Hyde2017; but cf. Falk & Lee, Reference Falk and Lee2012). In early childhood, positive parenting has been associated with better empathy and pro-sociality via more enjoyable parent–child interactions and desire to comply with the parent (Kochanska et al., Reference Kochanska, Forman, Aksan and Dunbar2005). It is plausible that a similar mechanism occurs in adolescence (see, e.g., Ray et al., Reference Ray, Frick, Thornton, Wall Myers, Steinberg and Cauffman2017). Alternatively, adolescents might continue to benefit from positive parenting experienced earlier in life. As punishment seems to be less effective at high levels of CU traits (Blair et al., Reference Blair, Colledge and Mitchell2001), reciprocally warm and committed relationships are likely to be an especially important protective factor throughout childhood and adolescence, even if positive parenting is most effective in infancy.
There are other, noncausative factors that likely contribute to the observed associations between low positive parenting and CD/HCU. Genetic similarity between parent and child is an obvious candidate, given the high heritability of CU traits (Viding et al., Reference Viding, Blair, Moffitt and Plomin2005). It seems likely that CU traits in parents would manifest as lack of warmth and interest toward the child. Nonetheless, it is clear from adoption studies that positive parenting is associated with reductions in CU traits and related behavior even in the absence of a genetic relationship between parent and child (Hyde et al., Reference Hyde, Waller, Trentacosta, Shaw, Neiderhiser, Ganiban and Leve2016; Waller et al., Reference Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Hyde2016; Waller, Shaw, Neiderhiser, et al., Reference Waller, Shaw, Neiderhiser, Ganiban, Natsuaki, Reiss and Hyde2017). Furthermore, positive parenting interventions have proved efficacious for young children (Elizur & Somech, Reference Elizur and Somech2018), suggesting a causal relationship in addition to shared genetic effects. Gene–environment correlations, and in particular evocative gene–environment correlations, are another relevant consideration here. For example, associations with parenting are bidirectional; child temperament (partially genetic) influences parenting (an environmental influence) as well as vice versa (Muñoz et al., Reference Muñoz, Pakalniskiene and Frick2011; Salihovic, Kerr, Ozdemir, & Pakalniskiene, Reference Salihovic, Kerr, Özdemir and Pakalniskiene2012). Thus, while low positive parenting is likely causally linked to CD/HCU, there are additional factors that plausibly contribute to the observed associations between low positive parenting and CD/HCU.
Group-level differences in negative parenting
Youths with both CD/HCU and CD/LCU reported higher levels of negative parenting than TD youths, but unlike positive parenting, exposure to negative parenting did not differ significantly in CD/HCU versus CD/LCU. The literature is divided on the relative importance of negative parenting in these subtypes. There are reports of potential insensitivity to negative parenting in CD/HCU (Wootton et al., Reference Wootton, Frick, Shelton and Silverthorn1997) as well as high levels of negative parenting (Barker, Oliver, Viding, Salekin, & Maughan, Reference Barker, Oliver, Viding, Salekin and Maughan2011; Fontaine et al., Reference Fontaine, McCrory, Boivin, Moffitt and Viding2011) and a role for negative parenting (harshness) in both aggression and CU traits (Waller et al., Reference Waller, Hyde, Klump and Burt2018). The associations between negative parenting, CD/HCU, and CD/LCU observed here do not warrant conclusions about causation, and it is already clear that relationships are bidirectional (Flom et al., Reference Flom, White, Ganiban and Saudino2019; Hawes et al., Reference Hawes, Dadds, Frost and Hasking2011; Larsson et al., Reference Larsson, Viding and Plomin2008; Muñoz et al., Reference Muñoz, Pakalniskiene and Frick2011; Pardini et al., Reference Pardini, Lochman and Powell2007; Pisano et al., Reference Pisano, Muratori, Gorga, Levantini, Iuliano, Catone and Masi2017). However, in the current sample at least, negative parenting did not appear to be a specific risk factor for CD/HCU over and above the risk for CD generally.
The relative importance of positive and negative parenting behaviors for classifying individuals
There were very clear differences between classifier models in the relative importance of positive and negative parenting behaviors. Overall, positive parenting was highly relevant when distinguishing individuals who differed substantially on CU traits (HCU-TD and HCU-LCU models), while negative parenting was highly relevant when distinguishing individuals who differed substantially on CD symptoms (HCU-TD and LCU-TD models). It is especially interesting to note that positive parenting was very low in relevance in the LCU-TD model, despite significant differences in both positive and negative parenting at the group level. This implies that even when exposure to positive parenting is low, negative parenting is a much more reliable indicator of CD/LCU. This pattern of relevance aligns with previous research indicating that negative parenting is linked to conduct problems and CU traits while low positive parenting is linked primarily to CU traits (e.g., Waller et al., Reference Waller, Gardner, Viding, Shaw, Dishion, Wilson and Hyde2014). Of note, however, positive reinforcement was low in relevance across all models. This was unexpected, and suggests that when the broader parenting context is taken into account, low positive reinforcement is not strongly indicative of CD/HCU or CD/LCU. However, it is interesting to note that the APQ positive reinforcement subscale includes items assessing material rewards (“your parents reward or give something extra to you for behaving well”) as well as warmth (e.g., “your parents hug or kiss you when you have done something well”). In previous studies linking CU traits to low positive parenting, warmth, rather than material rewards, has often been a key measure (e.g., Waller et al., Reference Waller, Gardner, Viding, Shaw, Dishion, Wilson and Hyde2014). The effects of warmth and praise versus provision of material incentives will be an interesting topic for future research on parenting and CD subtypes.
Finally, it should be noted again here that relevance scores were derived only from the higher performing models. This ensured that relevance scores were not influenced by models that failed to distinguish between groups. However, in the case of the poorly performing HCU-LCU model, it also means that relevance scores are not necessarily reflective of the full CD sample. While positive parenting was key to classifying those youths who could be distinguished, many youths with CD/HCU could not be distinguished from those with CD/LCU based on parenting. Thus, although positive parenting clearly differs between CD/HCU and CD/LCU at the group level, and between many individuals in these groups, positive parenting is far from a universally distinguishing factor between CD/HCU and CD/LCU. This suggests a fairly high level of heterogeneity within CD, even after accounting for differences in CU trait levels.
Heterogeneity within CD/HCU and CD/LCU
Although youths with CD/HCU and CD/LCU exhibit differences in their experiences of parenting, as well as their presentations more generally, it is clear that both subtypes still contain considerable heterogeneity. There are multiple sources for this heterogeneity. For example, there are likely to be sex differences in the importance of environmental influences in CD. Specifically, it appears that environmental factors might be relatively more important in the development of CU traits in females than in males (e.g., Fontaine, Rijsdijk, McCrory, & Viding, Reference Fontaine, Rijsdijk, McCrory and Viding2010). In our sample, it appeared that females with CD experienced more negative and less positive parenting than males with CD, while in TD youths, this pattern was reversed. This pattern of sex differences might plausibly reflect a greater environmental contribution to CD in females, although interactions were often not significant in the current sample.
In addition to sex differences, comorbid disorders, such as attention-deficit/hyperactivity disorder, anxiety, and depression, are likely to contribute to heterogeneity within CD/HCU. The CD/HCU and CD/LCU groups in the current sample differed significantly on the presence of these comorbidities. Perhaps most important, we did not distinguish youths with CD/HCU and comorbid internalizing disorders from those with CD/HCU alone. This distinction might reflect different aetiological pathways, and thus contribute to sample heterogeneity; it is thus a potentially important distinction for future research (Cecil, McCrory, Barker, Guiney, & Viding, Reference Cecil, McCrory, Barker, Guiney and Viding2018).
Strengths and limitations
This study has several strengths, including the large and well-characterized sample, the combination of parent- and child-report parenting measures and the use of both univariate and multivariate techniques. In particular, the use of a multivariate classification technique is novel, and demonstrates for the first time the relative importance of different dimensions of parenting when they are considered in a holistic (i.e., multivariate) context. This differs from univariate methods, where each dimension of parenting is considered only in isolation, and complex interactions between the different dimensions cannot be detected. However, the study also has several weaknesses, particularly in terms of sample heterogeneity. First, our sample spanned a very large age range (9–18 years), and was considerably older than those from much of the more recent literature (e.g., Hyde et al., Reference Hyde, Waller, Trentacosta, Shaw, Neiderhiser, Ganiban and Leve2016; Waller et al., Reference Waller, Trentacosta, Shaw, Neiderhiser, Ganiban, Reiss and Hyde2016). Although our findings align with those from these younger samples, it seems likely that the relative contribution of parenting to CD will change throughout childhood. For example, exposure to community violence might be particularly relevant during the adolescent years (Kersten et al., Reference Kersten, Vriends, Steppan, Raschle, Praetzlich, Oldenhof and Martinelli2017). Replication of the current classification analyses in younger children would be an interesting direction for future research. Second, the measure of CU traits used in the current sample was limited to parent-report data only. Although parent-report data might be more informative than self-report data, a combination of different informants is ideal (Docherty, Boxer, Huesman, O'Brien, & Bushman, Reference Docherty, Boxer, Huesmann, O'Brien and Bushman2017). Third, we used sample-specific (tertile) cutoff points as the criteria for allocation to the CD/HCU and CD/LCU groups. A clinical cutoff, designed to match the DSM criteria, has recently been published; however, this is currently based on self-report data only (Frick, Reference Frick2019). Fourth, we relied on parent and child reports of parenting, which though meaningful are not necessarily objective. These reports would ideally have been complemented with observational data. Fifth, we were not able to obtain information on family structure for the complete sample, although this appeared to be a potential source of variation in parenting experience for our sample.
Summary and conclusions
In summary, CD/HCU and CD/LCU were distinguished from TD by both positive and negative parenting at the group level, while negative parenting was more relevant for distinguishing CD/LCU from TD at the individual level. CD/HCU was distinguished from CD/LCU primarily by positive parenting, at both the group and individual levels. This adds to a growing body of literature suggesting that parenting is associated with both CD/HCU and CD/LCU, but that the specific parenting practices associated with CD and CU traits are somewhat different. We suggest that future research should further distinguish between different parenting behaviors (e.g., verbal praise and affection vs. provision of material incentives), as well as multiple types of externalizing behavior (e.g., proactive vs. reactive aggression, hyperactive-impulsive, etc.). Making such distinctions will hopefully contribute to the development of more targeted parenting interventions in the future.
Supplementary material
Supplementary material available online at https://doi.org/10.1017/S0954579420000279
Acknowledgments
We would like to thank Allan White for his advice on statistics, and Kamlesh Patel for assistance in implementing the Angle-GMLVQ method. We would also like to thank all members of the FemNAT-CD consortium for their contributions to the project. In particular, we thank Marietta Kirchner for her work on the imputation of missing data. Finally, we would like to thank our participants, their families, and the numerous teachers, clinicians, social workers, foster carers, and other professionals who gave their time generously to assist with recruitment and participate in the study.
Financial support
The present study is part of the FemNAT-CD consortium (Neurobiology and Treatment of Adolescent Female Conduct Disorder: The Central Role of Emotion Processing, coordinator Christine M. Freitag). This collaborative project is funded by the European Commission under the 7th Framework Health Program with Grant Agreement no. 602407. Ruth Pauli is a PhD student funded by the Biotechnology and Biological Sciences Research Council's Midlands Integrative Biosciences Training Partnership. Stephane A. De Brito was supported by a research fellowship from the Swiss National Science Foundation (SNSF PA00P1_139586).
Conflict of Interest
Christine M. Freitag receives royalties for books on attention-deficit/hyperactivity disorder and autism spectrum disorder. She has served as consultant to Desitin and Roche. No other authors report any conflicts of interest.







