



Introduction
Conduct disorder (CD) is generally defined by serious and persistent patterns of behavior that violate the rights of others (i.e., aggressive and rule-breaking behaviors) (APA, 2013). Recently, the Diagnostic and Statistical Manual of Mental Disorders (DSM)-5 introduced the limited prosocial emotions as a specifier to CD (APA, 2013), given the extensive work on callous–unemotional (CU) traits suggesting that the latter feature is associated with a distinct developmental pathway and more severe and persistent antisocial outcomes (Frick, Ray, Thornton, & Kahn, Reference Frick, Ray, Thornton and Kahn2014; Longman, Hawes, & Kohlhoff, Reference Longman, Hawes and Kohlhoff2016). However, a growing body of evidence highlights the fact that children with conduct problems (CP) are a highly heterogeneous population (Fanti, Reference Fanti2018; Hawes, Reference Hawes2014). This further emphasizes the importance of recognizing early manifestations of psychopathologies that may be developmental roots of heterogeneity underlying CP.
Heterogeneity in clinical presentation
The operationalization of clinical criteria for CD may be itself a source of developmental heterogeneity. CP usually include aggressive behaviors (AGG) (i.e., physical fights, cruelty, sexual assault) and nonaggressive delinquent behaviors or rule-breaking behaviors (RB) (i.e., property, theft, violations of rules) (Burt, Donnellan, Iacono, & McGue, Reference Burt, Donnellan, Iacono and McGue2011; Loeber & Stouthamer-Loeber, Reference Loeber and Stouthamer-Loeber1998; Tackett, Krueger, Iacono, & McGue, Reference Tackett, Krueger, Iacono and McGue2005; Tackett, Krueger, Sawyer, & Graetz, Reference Tackett, Krueger, Sawyer and Graetz2003; Tremblay, Reference Tremblay2000, Reference Tremblay2010). However, although the past 25 years of research has considered AGG and RB on a single CP scale (Tremblay, Reference Tremblay2010), it has been argued that these features should not be aggregated together owing to substantial differences in terms of developmental trajectories and risk factors between AGG and RB (Burt et al., Reference Burt, Donnellan, Iacono and McGue2011; Fairchild, Van Goozen, Calder, & Goodyer, Reference Fairchild, Van Goozen, Calder and Goodyer2013; Tremblay, Reference Tremblay2010). While the AGG syndrome seems to be more stable across adolescence and tends to decrease from early childhood to adulthood (Stanger, Achenbach, & Verhulst, Reference Stanger, Achenbach and Verhulst1997; Tremblay et al., Reference Tremblay, Nagin, Séguin, Zoccolillo, Zelazo, Boivin and Japel2004), the RB syndrome appears to increase sharply over the course of adolescence (Moffitt, Reference Moffitt, Lahey, Moffitt and Caspi2003). Moreover, RB is more often associated with environmental risk factors (e.g., low parental education, deviant peers, substance use) (Derzon, Reference Derzon2010; Loeber, Reference Loeber1990), while the AGG component of CD seems to be more closely related to temperamental characteristics (e.g., emotional arousability, depressive and anxiety symptoms [DAS], hyperactive/impulsive traits [H/I]) (Dugré, Dumais, Dellazizzo, & Potvin, Reference Dugré, Dumais, Dellazizzo and Potvin2019; Dugré & Potvin, Reference Dugré and Potvin2020; Garofalo & Velotti, Reference Garofalo and Velotti2017; Loeber, Reference Loeber1990; Lorber, Reference Lorber2004; Rey, Sawyer, & Prior, Reference Rey, Sawyer and Prior2005). Therefore, the distinction between these two core components of CD needs to be taken into account in developmental research in order to tackle the substantial heterogeneity in this population.
Comorbities and subgroups
The heterogeneity in CD may also be observed through manifestations of transdiagnostic features or comorbid disorders. For instance, early signs may include temper tantrum tendencies, impulsivity, and headstrong, which encompass attention deficit–hyperactivity disorder (ADHD) and oppositional-defiant disorder (ODD) (Blair, Leibenluft, & Pine, Reference Blair, Leibenluft and Pine2014). Thus, the heterogeneity in CD is likely to arise from multiple pathways involving distinct features from several psychopathological dimensions. The most prevalent co-occurring features of CD is CU (in 20–50% of cases) (Frick et al., Reference Frick, Ray, Thornton and Kahn2014). However, previous studies have also shown that there are elevated rates of comorbidity between CD and other psychopathologies. More precisely, children with CD are at moderate to high risk for being also diagnosed with anxiety disorders (i.e., odds ratios [OR] 95% confidence interval [CI] = 1.3–5.9), mood disorders (OR 95% CI = 2.1–50.5), ADHD (ADHD; OR 95% CI = 3.7–121.9), and ODD (OR 95% CI = 5.3–17.3) (Angold, Costello, & Erkanli, Reference Angold, Costello and Erkanli1999; Costello, Mustillo, Erkanli, Keeler, & Angold, Reference Costello, Mustillo, Erkanli, Keeler and Angold2003; Frick et al., Reference Frick, Ray, Thornton and Kahn2014; Nock, Kazdin, Hiripi, & Kessler, Reference Nock, Kazdin, Hiripi and Kessler2006). This further suggests that the heterogeneity in CD may arise from comorbities involving four main psychopathological dimensions (i.e., CU traits, anxiety and mood disorders, ADHD, and ODD) (Blair et al., Reference Blair, Leibenluft and Pine2014; Fanti, Reference Fanti2018).
In the past decades, two main developmental pathways underlying the heterogeneity of CD were identified: the CD + CU and the CD + Internalizing subtypes (Fanti, Reference Fanti2018; Frick et al., Reference Frick, Ray, Thornton and Kahn2014; Herpers, Rommelse, Bons, Buitelaar, & Scheepers, Reference Herpers, Rommelse, Bons, Buitelaar and Scheepers2012). While the former is the most prevalent subgroup and is characterized by more severe and persistent antisocial outcomes and impairment in response/recognition of cues to fear (Frick et al., Reference Frick, Ray, Thornton and Kahn2014), the CD + internalizing subgroup is associated with more reactive aggression and antisocial/delinquent behaviors, as well as physiological overarousal in negative situations (e.g., threat-related situations), compared with the CD-only group (Fanti, Reference Fanti2018; Fanti & Henrich, Reference Fanti and Henrich2010; Polier, Vloet, Herpertz-Dahlmann, Laurens, & Hodgins, Reference Polier, Vloet, Herpertz-Dahlmann, Laurens and Hodgins2012). However, to further complicate matters, these two pathways are not mutually exclusive. Compared with children with Interpersonal Callousness-only (i.e., first variant of psychopathy), those characterized by the co-occurrence of interpersonal callousness (i.e., including affective and interpersonal facets of psychopathic traits [IC]) and anxiety (IC + ANX, i.e., secondary variant of psychopathy) showed also ADHD symptoms, DAS, irritability, and anger problems, and were more likely to exhibit drug use, risky behaviors, and suicidal ideation and attempts (Cecil, McCrory, Barker, Guiney, & Viding, Reference Cecil, McCrory, Barker, Guiney and Viding2018; Fanti, Demetriou, & Kimonis, Reference Fanti, Demetriou and Kimonis2013; Goulter, Kimonis, Hawes, Stepp, & Hipwell, Reference Goulter, Kimonis, Hawes, Stepp and Hipwell2017; Huang, Fan, Lin, & Wang, Reference Huang, Fan, Lin and Wang2019; Kahn et al., Reference Kahn, Frick, Youngstrom, Kogos Youngstrom, Feeny and Findling2013; Kimonis, Frick, Cauffman, Goldweber, & Skeem, Reference Kimonis, Frick, Cauffman, Goldweber and Skeem2012; Kimonis, Skeem, Cauffman, & Dmitrieva, Reference Kimonis, Skeem, Cauffman and Dmitrieva2011; Meehan, Maughan, Cecil, & Barker, Reference Meehan, Maughan, Cecil and Barker2017; Vaughn, Edens, Howard, & Smith, Reference Vaughn, Edens, Howard and Smith2009). Furthermore, although some evidence suggest that IC + ANX may exhibit higher levels of AGG (Kahn et al., Reference Kahn, Frick, Youngstrom, Kogos Youngstrom, Feeny and Findling2013; Kimonis et al., Reference Kimonis, Skeem, Cauffman and Dmitrieva2011) and CD (Goulter et al., Reference Goulter, Kimonis, Hawes, Stepp and Hipwell2017; Huang et al., Reference Huang, Fan, Lin and Wang2019; Meehan et al., Reference Meehan, Maughan, Cecil and Barker2017), others did not find significant differences between both subgroups (Cecil et al., Reference Cecil, McCrory, Barker, Guiney and Viding2018).
While these subgroups of children at risk for CD have been relatively well defined in literature, more complex combinations of psychopathological features (resulting in more homogeneous groups of children at risk for CP) have yet to be elucidated. Considering the complexity of the heterogeneity in the CD population, more advanced methodologies, such as longitudinal person-centered approaches, may help disentangle the developmental co-occurrence of psychological factors leading to CD.
Developmental joint- and multitrajectory
Recent advances in statistical analyses on longitudinal data allows the examination of developmental joint- and multitrajectories within a person-centered approach. Multitrajectory analysis (Nagin, Jones, Passos, & Tremblay, Reference Nagin, Jones, Passos and Tremblay2018) or parallel processes growth mixture model (Muthén & Muthén, Reference Muthén and Muthén2009) are multivariate extensions of univariate growth mixture modelling (i.e., identification of trajectories for a single indicator of interest), permitting identification of the interrelationship of multiple processes over time (Muthén & Muthén, Reference Muthén and Muthén2009; Nagin, Reference Nagin2005; Nagin et al., Reference Nagin, Jones, Passos and Tremblay2018). For instance, this technique enables the study of substantial co-occurrence of child psychological factors in a developmental manner. Past longitudinal researches have thus demonstrated that the developmental joint contribution of CU and CP (Fontaine, McCrory, Boivin, Moffitt, & Viding, Reference Fontaine, McCrory, Boivin, Moffitt and Viding2011; Klingzell et al., Reference Klingzell, Fanti, Colins, Frogner, Andershed and Andershed2016), DAS and irritability/anger proneness (Dugré et al., Reference Dugré, Dumais, Dellazizzo and Potvin2019), internalizing and externalizing traits (Fanti & Henrich, Reference Fanti and Henrich2010), and hyperactivity/impulsivity symptoms (H/I) and physical aggression (Fontaine et al., Reference Fontaine, Carbonneau, Barker, Vitaro, Hébert, Côté and Tremblay2008) significantly increased the risk of developing a variety of CP. While these studies observed statistical associations between psychological features (e.g., internalizing traits, IC, H/I symptoms) and behaviors (e.g., physical aggression, CP, externalizing behaviors), there is still very limited literature about how developmental combinations of psychological factors (i.e., IC, H/I, ANX, irritability) – independently from CD – may interact with risk for developing CP symptoms. In other words, is identifying homogeneous developmental combinations of psychological factors sufficient to predict emergence of CP.
To our knowledge, three longitudinal studies have attempted to examine developmental multitrajectory profiles (i.e., multitrajectory based on more than two indicators of interest) in relation with CP. Such method may help address the heterogeneity in CD by studying more complex developmental combination of psychological features. For instance, in a population-based cohort, researchers observed that children with H/I only and H/I + IC traits (i.e., low prosocial behaviors and fearlessness) were significantly associated with CD in adolescence even after controlling for early antisocial problems (Côté, Tremblay, Nagin, Zoccolillo, & Vitaro, Reference Côté, Tremblay, Nagin, Zoccolillo and Vitaro2002). Another study, of 622 children from 3 to 7 years old, Ezpeleta, Granero, de la Osa, and Domènech (Reference Ezpeleta, Granero, de la Osa and Domènech2017) found that the groups characterized by co-occurrence of CU + ODD showed higher levels of CP and AGG than typically developing children at 7 years old. Finally, based on 3,569 children assessed from 5 to 15 years old, we have observed that children following a developmental trajectory characterized by H/I + irritable and H/I + irritable + ANX were, respectively, 6.47 and 7.68 times more likely than their typically developing counterparts to also exhibit childhood aggression (Dugré & Potvin, Reference Dugré and Potvin2020). These studies show an additive effect of psychological features on risk for CP, that is, the more problematic the psychological features, the greater risk children are for exhibiting CP. However, while these studies showed promising results for clarifying the heterogeneity underlying CD, to our knowledge, no study has assessed the developmental profiles based on the four core components that are related to CD (i.e., IC, H/I, ANX, irritability). Furthermore, considering the heterogeneous clinical presentation of CD (i.e., AGG and RB syndromes), there are very limited studies exploring the associations between multitrajectory of psychological patterns and distinct CP symptoms. Overcoming these limitations is therefore crucial for disentangling the clinical heterogeneous developmental pathways of CD and identifying groups of children at most risk for CP and its specific syndromes.
In the current study, we thus aimed to (a) identify developmental combinations of psychological factors of interest (i.e., H/I, DAS, irritability, and IC) from 6 to 12 years old, and (b) assess their longitudinal associations with childhood CP (i.e., AGG and RB syndrome) and adolescence CP (i.e., 15 and 17 years old). Based on previous literature, we argue that multiple combinations of these psychological factors will be differently related to CP. More precisely, multitrajectory groups characterized by high DAS and irritability (i.e., more internalizing traits) would be more likely to exhibit AGG behaviors than their counterparts, while those with problematic levels of H/I (i.e., more externalizing traits) would be associated with more RB. Furthermore, considering the role of IC in CD (Frick et al., Reference Frick, Ray, Thornton and Kahn2014), the observed developmental childhood profiles characterized by those with high-IC will predict both AGG and RB in childhood, and general CP in adolescence even after controlling for early CP. Finally, we argued that an additive effect would be observed, that is, children following more complex multitrajectory (i.e., problematic levels on three and four psychological factors) would predict CP, compared with those following more simpler ones.
Method
Participants
Participants were drawn from the widely known Québec Longitudinal Study of Child Development (QLSCD) (Orri et al., Reference Orri, Galera, Turecki, Forte, Renaud, Boivin and Geoffroy2018; Pagani, Fitzpatrick, Barnett, & Dubow, Reference Pagani, Fitzpatrick, Barnett and Dubow2010; Simard, Nielsen, Tremblay, Boivin, & Montplaisir, Reference Simard, Nielsen, Tremblay, Boivin and Montplaisir2008). Briefly, the QLSCD consists of a representative sample of 2120 infants born in the province of Quebec (Canada) in 1997–1998, whom were followed up to 17 years of age. More detailed information concerning the methodology behind data collection can be found elsewhere (Jetté & Des Groseilliers, Reference Jetté and Des Groseilliers2000). Data was collected every year during childhood (5 months to 8 years of age) and biannually during adolescence (from 10 to 17 years of age) by the Québec Statistics Institute. The QLSCD protocol was approved by the Québec Statistics Institute and the St-Justine Hospital Research Center ethics committees. All primary caregivers provided written informed consent and assented for child participation at each interview. Participants were included if the school teachers completed assessments at a minimum of two time points, in order to adequately estimate the intercept and a linear slope in trajectory analyses, as similarly done in other researches on developmental trajectories (Dugré et al., Reference Dugré, Dumais, Dellazizzo and Potvin2019; Dugré & Potvin, Reference Dugré and Potvin2020). Of the 2120 infants, school teachers from 1,309 participants completed the behavior questionnaire at two time periods when children were 6 (Y6), 8 (Y8), 10 (Y10), and/or 12 year (Y12) of age. While deletion may reduce the representativeness of the sample and/or reduce statistical power, subsequent analyses on excluded participants revealed small differences with the original sample in terms of children's sex (effect size = −0.11), socioeconomic status (effect size = −0.19), and children's verbal IQ (effect size −0.09) (Orri et al., Reference Orri, Galera, Turecki, Forte, Renaud, Boivin and Geoffroy2018).
Measures
Teacher ratings of child psychological factors
School teachers rated child behaviors at Y6, Y8, Y10, and Y12. The behavior questionnaire is a well validated questionnaire that was created in 1994, for the Canadian National Longitudinal Study of Children and Youth (Statistics Canada, 2007), and includes items from the Child Behavior Checklist (Achenbach & Edelbrock, Reference Achenbach and Edelbrock1983) and the preschool behavior questionnaire (Behar, Reference Behar1977). Each item was assessed relatively to the past 6 months and rated on a 3-point Likert scale, ranging from 0 (never) to 2 (often occurring).
H/I symptoms were assessed using six items (e.g., [CHILD] “could not sit still, was restless and hyperactive” and “was impulsive, acted without thinking”). Irritability symptoms were assessed with four items (e.g., “had temper tantrums or hot temper” and “reacted in an aggressive manner when teased”) (Orri et al., Reference Orri, Galera, Turecki, Forte, Renaud, Boivin and Geoffroy2018). IC symptoms were assessed with eight items that included affective and interpersonal callousness (Gorin et al., Reference Gorin, Kosson, Miller, Fontaine, Vitaro, Séguin and Tremblay2019) (e.g., “was unconcerned about the feelings of others” and “didn't seem to feel guilty after misbehaving”). DAS symptoms were assessed with nine items based on past literature (Orri et al., Reference Orri, Galera, Turecki, Forte, Renaud, Boivin and Geoffroy2018) (e.g., “was too fearful or anxious,” “seemed to be unhappy or sad.” Cronbach's alpha showed excellent internal consistencies for all psychological factor (α values ranging between .85 and .91).
Teacher ratings of child CP
School teachers also rated child CP based on eight items at Y6, Y8, Y10, and Y12 from the behavior questionnaire (see above): Including a total score of AGG (three items, e.g., “physically attacked people” and “hit, bit or kicked other children“) and RB (five items, e.g., “stole things” and “damaged or broke things belonging to others”). Cronbach's alpha showed good to excellent internal consistencies for CP total score, AGG, and RB (α values ranging between .76 and .89).
Self-reported adolescent CP
Adolescence CP were assessed using 28 self-reported items derived from the Mental Health and Social Inadaptation Assessment for Adolescents (MIA), spanning DSM-V CD criteria (Côté et al., Reference Côté, Orri, Brendgen, Vitaro, Boivin, Japel and Falissard2017). Each item was answered on a 3-point Likert-scale, ranging from 0 (never true) to 2 (always true). Cronbach's alpha showed good internal consistency at 15 and 17 years of age (i.e., .87 and .94, respectively).
Statistical procedure
Multitrajectory modelling
Latent class growth analysis (LCGA) was used to identify classes of individuals who have a homogeneous developmental trajectory (e.g., normative vs. problematic) from childhood to adolescence (Muthén & Muthén, Reference Muthén and Muthén2000). Briefly, LCGA is a specific type of growth mixture model (GMM), which assumes that all individual growth trajectories within a class are homogeneous in order to identify distinct classes (Jung & Wickrama, Reference Jung and Wickrama2008). Thus, LCGA does not allow between-subject variability within a class and thus fewer parameters need to be estimated (compared to GMMs). Since the complexity of the statistical models to be estimated as well as the limited sample size in this study, the LCGA was preferred over the GMMs to avoid overfitting (van der Nest, Passos, Candel, & van Breukelen, Reference van der Nest, Passos, Candel and van Breukelen2020).
The current study first aimed to use a data-driven technique to distinguish between children following an atypical developmental trajectory from those typically developing (TD) on each psychological factor. Consequently, we estimated a two-trajectory LCGA model for each of the four psychological factors, separately. The goodness of fit was assessed based on several criteria (Nylund, Asparouhov, & Muthén, Reference Nylund, Asparouhov and Muthén2007), such as the smallest class size (>1%) (Jung & Wickrama, Reference Jung and Wickrama2008), the Vuong–Lo–Mendell–Rubin Likelihood Ratio Test (VLMR-LRT), as well as the Lo–Mendell–Rubin Adjusted Likelihood Ratio Test (LMR-LRT; p > .05) (Lo, Mendell, & Rubin, Reference Lo, Mendell and Rubin2001; Vuong, Reference Vuong1989), the entropy (closest to 1.0) (Celeux & Soromenho, Reference Celeux and Soromenho1996), the average posterior class probabilities (AvePP > .70), and the odds of correct classification (OCC > 5.0) (Nagin, Reference Nagin2005).
Second, the resulting parameters (e.g., number of classes, growth factors) were entered in a parallel process GMM (Muthén & Muthén, Reference Muthén and Muthén2009). Briefly, the latter model estimates the probability of individuals being in a class for each of the processes resulting in a cross-classification of the sets of growth mixtures. Children would thus fall into one of 16 multitrajectory classes (24) based on the maximum posterior class probability. The resulting multitrajectories were then kept in further statistical analyses if: (a) the AvePP ≥ .70 and the OCC ≥ 5.0, indicating a good latent class separation and high assignment accuracy and (b) the multitrajectory class comprised a total count larger than 1% of the total sample size. For both LCGA and parallel process analyses, we used a full-information maximum likelihood (FIML) estimator with robust standard errors under the missing-at-random assumption, used in Mplus statistical software (Muthén & Muthén, 1998–2011).
Associations between multitrajectories and childhood CP
Group memberships were then extracted as a categorical variable to further explore the link between groups and longitudinal levels for childhood CP. A generalized estimating equations (GEE) (Liang & Zeger, Reference Liang and Zeger1986) model with a negative binomial distribution and an unstructured working correlation matrix was used to examine the longitudinal associations between multitrajectory classes group membership and teachers ratings of child CP at Y6, Y8, Y10, and Y12. Since parallel process GMM assumes that trajectory-group membership is homogeneous across time (i.e., one cannot switch trajectory over time), multitrajectory group membership was entered as a fixed effect variable. Children's sex and parental socioeconomic status were included as covariates. The multitrajectory model, having the lowest levels of symptoms, was used as the reference group. As post hoc testing, we analyzed the specific associations between multitrajectories and AGG and RB separately, since both behaviors are known to have distinct developmental courses (Tremblay, Reference Tremblay2010).
Prospective predictions of CP in adolescence from childhood multitrajectories
Longitudinal predictions of self-reported CP in adolescence (Y15 and Y17) from childhood multitrajectories were also tested using GEE models with a negative binomial distribution and an unstructured working correlation matrix. Estimates were first provided adjusting for children's sex and parental socioeconomic status. Moreover, to examine whether the childhood multitrajectories predicted adolescent CP over and above early CP (Côté et al., Reference Côté, Tremblay, Nagin, Zoccolillo and Vitaro2002), we adjusted the model's estimates for teachers' ratings of CP at Y6 as an indicator of an early onset of antisocial behaviors.
Results
Multitrajectory modelling
First, two-trajectory LCGA models were estimated for each of the psychological factors, independently. Models showed good to excellent fit indices for DAS (entropy = .76, smallest class size = 20.88%, smallest AvePP = .87, smallest OCC = 5.01, VLMR = p < .0001, LMR-LRT = p < .0001), H/I symptoms (entropy = .90, smallest class size = 18.44%, smallest AvePP = .93, smallest OCC = 11.67, VLMR = p < .0001, LMR-LRT = p < .0001), irritability (entropy = .93, smallest class size = 13.43%, smallest AvePP = .94, smallest OCC = 10.90, VLMR = p < .05, LMR-LRT = p < .05), and IC traits (entropy = .91, smallest class size=15.95%, smallest AvePP = .92, smallest OCC = 13.37, VLMR = p < .0001, LMR-LRT = p < .0001).
Second, by using the parameters of each of the two-trajectory LCGA models, parallel process GMM was estimated in order to extract every possible developmental combination of psychological factors. Therefore, the parallel process GMM, resulting in 16 possible combinations of multitrajectories (24), showed an excellent classification quality (entropy = .89). From these combinations, nine multitrajectory groups met the criteria for high-quality trajectory classes (see Method section) (Figure 1): G0 – typically developing (TD) (67.23% of the total sample, 62.0% of girls); G1 – DAS only (7.79%, 50.0%), G2 – IC only (1.83%, 41.7%); G3 – H/I only (2.6%, 23.5%); G4 – IC and H/I (2.14%, 21.4%), G5 – DAS and H/I (3.29%, 20.9%), G6 – irritable and IC (1.15%, 60.0%), and G7 – irritable, IC, and H/I (2.83%, 29.7%) and G8 – irritable, IC, H/I, and DAS (8.10%, 26.4%). Moreover, these nine groups showed a minimal AvePP value higher than .70 as well as OCC higher than 5 (Nagin, Reference Nagin2005), suggesting good to excellent within-class cohesion (see Supplementary Table 1). The resulting seven groups of multitrajectories that did not meet the selection criteria constituted only 3.04% of the total sample were excluded from subsequent analyses (see Supplementary Table 1).
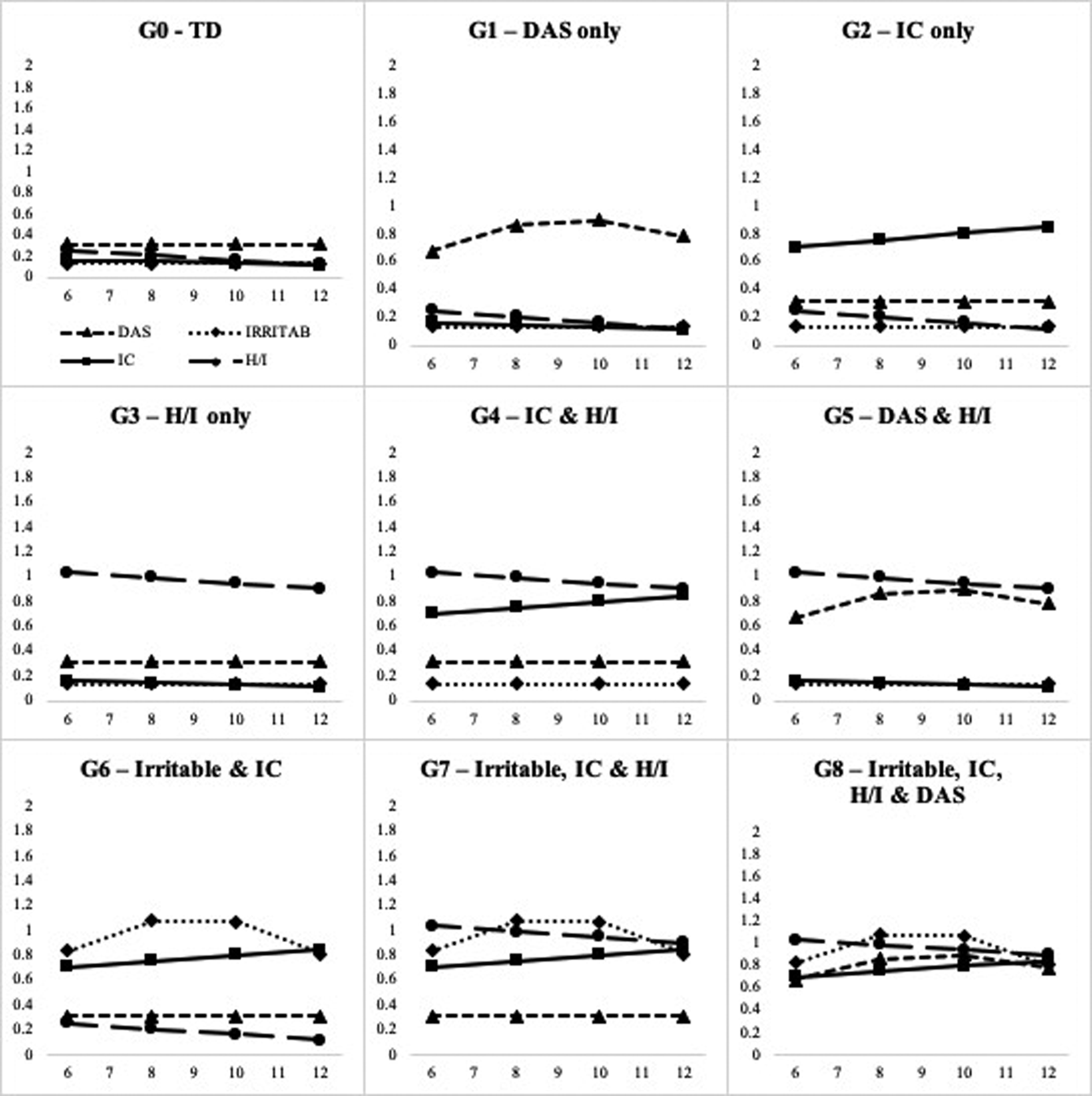
Figure 1. Multitrajectory classes defined by developmental trajectories of depressive and anxiety symptoms (DAS), irritability (IRRITAB), hyperactivity/impulsivity (H/I), and interpersonal callousness (IC), at 6, 8, 10, and 12 years of age. TD = typically developing. G0: AvePP = .94 and OCC = 7.92; G1: AvePP = .79 and OCC = 43.99; G2: AvePP = .74 and OCC = 150.08; G3: AvePP = .70 and OCC = 85.46; G4: AvePP = .78 and OCC = 164.12; G5: AvePP = .72 and OCC = 76.85; G6: AvePP = .76 and OCC = 279.25; G7: AvePP = .73 and OCC = 90.62; G8: AvePP = .85 and OCC = 66.38.
Associations between multitrajectories and childhood CP
Results from the GEE models suggest that children in every multitrajectory class were significantly more likely to exhibit CP in childhood in comparison with their counterparts in the TD group (Table 1). G1 – DAS-only class showed a significant association with CP, while being weaker (OR = 1.63, 95% CI: 1.28–2.09, p < .001). G2 – IC only showed a 4.90-fold association with CP. Moreover, G4 – IC and H/I conferred a risk of 5.15 times higher to display CP than the TD group, with a slight tendency to exhibit more RB than AGG (OR = 7.2 and 5.8, respectively) (See Figure 2). Finally, compared with TD, G6 – irritable and IC, G7 – irritable, IC, and H/I, G8 – irritable, IC, H/I, and DAS were considered the groups at greatest risk of exhibiting CP during childhood (OR = 8.71, 9.30, and 9.62, respectively). Post-hoc analyses on specific CP suggested that while G6, G7, and G8 were significantly more likely to display AGG than other groups, G4 – IC and H/I, G7, and G8 groups were at higher risk for exhibiting RB, compared with other groups, but did not differ between each other (See Figure 2 and Supplementary Material).

Figure 2. Estimates (odds ratios) are adjusted for the effects of time, child's sex, and socioeconomic status. Error bars represent 95% confidence interval. G0 = typically developing (reference group); G1 = anxious–depressive only (aggressive behaviors: OR = 1.42 and rule-breaking behaviors: OR = 1.34), G2 = interpersonal callousness only (5.41 and 4.71, respectively); G3 = hyperactivity/impulsivity only (4.59 and 4.55, respectively); G4 = interpersonal callousness and hyperactivity/impulsivity (5.83 and 7.15, respectively), G5 = anxious–depressive and hyperactivity/impulsivity (4.24 and 4.27, respectively), G6 = irritable and interpersonal callousness (10.64 and 5.40, respectively), G7 = irritable, interpersonal callousness, and hyperactivity/impulsivity (10.01 and 8.59, respectively), and G8 = irritable, interpersonal callousness, hyperactivity/impulsivity, and anxious–depressive symptoms (11.49 and 9.15, respectively). Post-hoc analyses for aggressive behaviors (at p < .005): G8 > G1, G2, G3, G4, G5, G6; G7 > G1, G2, G3, G4, G5; G6 > G1, G2, G3, G5; G5 > G1; G4 > G1; G3 > G1; G2 > G1. Post-hoc analyses for rule-breaking behaviors (at p < .005): G8 > G1, G2, G3, G5, G6; G7 > G1, G2, G3, G5, G6; G6 > G1; G5 > G1; G4 > G1, G2, G3, G5, G6; G3 > G1; G2 > G1.
Table 1. Associations between multitrajectories and childhood conduct problems (n = 1,309)
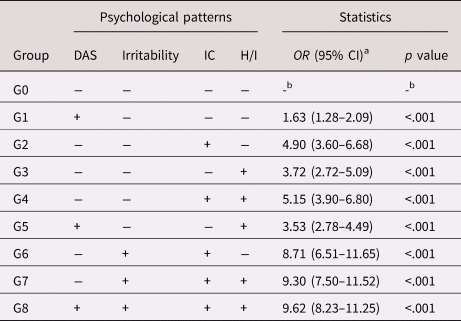
Note. DAS = depressive and anxiety symptoms; IC = interpersonal callousness; H/I = hyperactivity/impulsivity symptoms.
a Adjusted for the effects of time, children's sex and socioeconomic status.
b G0 was used as the reference group.
Prospective predictions of CP in adolescence from childhood multitrajectories
GEE models were conducted to evaluate if the multitrajectory groups predicted adolescence CP longitudinally (i.e., at Y15 and Y17). Of the eight groups compared with the TD, only four remained statistically significant after adjusting for early-onset CP, children's sex, and their socioeconomic status: G2 – IC only (OR = 1.92, 95% CI: 1.41–2.16, p < .001), G4 – IC and H/I (OR = 1.41, 95% CI: 1.04–1.90, p < .001), G6 – irritable and IC (OR = 1.48, 95% CI: 1.01–2.16, p < .001), G8 – irritable, IC, H/I, and DAS (OR 1.40, 95% CI: 1.12–1.74, p < .001) (see Table 2).
Discussion
In the current study, we aimed to disentangle the heterogeneity in the CD population by using a longitudinal person-centered approach in relation with specific subtypes of behaviors underlying CP. To our knowledge, this is the most extensive population-based longitudinal study to examine the developmental combinations of four psychological factors that are known to be involved in childhood CP, namely irritability, IC, DAS, and H/I symptoms. We observed that children from all multitrajectory classes were significantly more likely to also exhibit CP in childhood when compared with their TD counterparts, with ORs ranging between 1.63 and 9.62. For instance, being part of a multitrajectory characterized by at least a combination of IC and irritability, with or without H/I and/or DAS, drastically increased the risk for exhibiting CP during childhood. After adjustments for several important factors, including early CP, four childhood multitrajectory groups (those with IC) prospectively predicted CP in adolescence. These results further demonstrate the importance of studying the developmental co-occurrence of these four factors in relationship with CP.
Investigating the relationship between multitrajectory and subtypes of CP in childhood has revealed significant results. Following past research suggesting a non-negligible overlap in etiological influences between AGG and RB (Burt, Reference Burt2013), we observed that our multitrajectory classes were, in general, at somewhat similar risk for exhibiting AGG and RB, compared with TD. Our results suggested that the co-occurrence of IC and H/I dimensions was mostly associated with an increased risk for RB, while the co-occurrence of IC and irritability heightened the likelihood of AGG. First, these results are in line with past researches suggesting that elevated IC are associated with increased risk for more severe general CP (Frick et al., Reference Frick, Ray, Thornton and Kahn2014). More precisely, our findings indicated that an additive effect of psychological factors (i.e., irritability and H/I) may direct children with high IC towards more precise antisocial behaviors (i.e., AGG and RB). For instance, it is known that risky behaviors in children with ADHD could arise from a disrupted ability to suppress prepotent behavior (i.e., response inhibition) and/or impaired decision making (e.g., immediate over delayed rewards) (Sonuga-Barke, Cortese, Fairchild, & Stringaris, Reference Sonuga-Barke, Cortese, Fairchild and Stringaris2016). While it was postulated that H/I symptoms increase the risk for CP in children already at risk (e.g., those with high IC) (Lynam, Reference Lynam1996), their co-occurrence with IC traits (e.g., callousness, lack of guilt, manipulative) may enhance the risk for goal-oriented or instrumental behaviors, such as RB. As for irritability, this psychological feature may often results in AGG through aberrant threat-detection and/or frustrative nonreward mechanisms (Stringaris, Vidal-Ribas, Brotman, & Leibenluft, Reference Stringaris, Vidal-Ribas, Brotman and Leibenluft2018). Thus, in combination with IC traits (e.g., lack of empathy, lack of guilt), irritability could yield AGG in order to relieve intense negative emotional arousal. Hence, we showed that complex developmental combinations of multiple psychological factors were associated with specific CP subtypes.
Interestingly, although all multitrajectory classes were significantly associated with childhood CP, only those characterized by IC still remained a statistically significant predictor of adolescence CP. As commonly observed in literature on childhood IC, this psychological factor is a crucial predictor of later antisocial behaviors (Frick et al., Reference Frick, Ray, Thornton and Kahn2014; Frick & White, Reference Frick and White2008). More importantly, evidence has further highlighted the stability of IC traits from childhood to adolescence, above and beyond puberty (Burke, Loeber, & Lahey, Reference Burke, Loeber and Lahey2007; Lynam et al., Reference Lynam, Charnigo, Moffitt, Raine, Loeber and Stouthamer-Loeber2009; Salekin, Rosenbaum, & Lee, Reference Salekin, Rosenbaum and Lee2008). As for the other psychological factors, their influence must be considered in light of the strong effects of puberty onset (mean age of 12 years) on child development. Past results indicated that from childhood to late-adolescence, children would usually show moderate decreases in H/I symptoms (Döpfner et al., Reference Döpfner, Hautmann, Görtz-Dorten, Klasen, Ravens-Sieberer and Group2015; Faraone, Biederman, & Mick, Reference Faraone, Biederman and Mick2006; Larsson, Dilshad, Lichtenstein, & Barker, Reference Larsson, Dilshad, Lichtenstein and Barker2011; Nagin & Tremblay, Reference Nagin and Tremblay1999) and significant increases in DAS (Angold & Costello, Reference Angold and Costello2006; Angold, Costello, & Worthman, Reference Angold, Costello and Worthman1998; Bongers, Koot, Van der Ende, & Verhulst, Reference Bongers, Koot, Van der Ende and Verhulst2003). Thus, these opposite shifts in H/I and DAS may likely alter their influence on the propensity towards CP in adolescence, while IC would remain an important and stable predictor of CP throughout adolescence. Researches between DAS and CP have yielded in inconsistent findings (Bubier & Drabick, Reference Bubier and Drabick2009; Cunningham & Ollendick, Reference Cunningham and Ollendick2010; Wolff & Ollendick, Reference Wolff and Ollendick2006). Furthermore, some studies on developmental trajectories have suggested that DAS alone may not be sufficient for predicting risky behaviors including CP (Dugré & Potvin, Reference Dugré and Potvin2020; Ezpeleta et al., Reference Ezpeleta, Granero, de la Osa and Domènech2017; Fanti & Henrich, Reference Fanti and Henrich2010). Instead, these studies have suggested that the risk for CP would be significantly enhanced through an additive effect of DAS with other factors (e.g., irritability, H/I, and IC), similarly to what we observed in the current study.
In the past decades, research on CD has been largely influenced by descriptive and behavioral perspectives (APA, 2013; Crick & Dodge, Reference Crick and Dodge1996; Moffitt, Reference Moffitt1993; Tremblay, Reference Tremblay2010). One major drawback of this approach is the substantial behavioral heterogeneity in CD. While current classifications are usually based on the assumption that subjects within the same class (disorder or behavior) are likely to be homogeneous, it appears that over 32,000 different cross-sectional combinations of behaviors would lead to a CD diagnosis (Nock et al., Reference Nock, Kazdin, Hiripi and Kessler2006). Alternatively, very few studies hypothesized that CP could result from multiple combinations of psychological factors (Côté et al., Reference Côté, Tremblay, Nagin, Zoccolillo and Vitaro2002; Sigvardsson, Bohman, & Cloninger, Reference Sigvardsson, Bohman and Cloninger1987; Tremblay, Pihl, Vitaro, & Dobkin, Reference Tremblay, Pihl, Vitaro and Dobkin1994). In that regard, our multitrajectory framework appears promising as it offers evidence that furthers our understanding of the heterogeneous developmental pathways leading to CP. One novel contribution of the current study is that we observed that specific combinations of psychological factors were associated with distinct pathways towards subtypes of CP (i.e., AGG and RB). Second, children following more complex multitrajectory (i.e., with problematic levels on more than two features) on the psychological factors of interest were significantly more likely to exhibit CP that support evidence on the developmental heterogeneity in CD population. Finally, we showed that specific groups identified based on psychological features (independently of CP) significantly predicted adolescence CP even after adjusting for early CP. This current study shows encouraging results for studying CP through a multidimensional psychological framework (see Figure 3). More importantly, contrarily to the behavioral approach, tailoring preventive strategies for CD, based on psychological patterns, may be more effective when they are adjusted to the needs of specific subgroups (e.g., emotion-regulation; positive reinforcement) (Pardini & Frick, Reference Pardini and Frick2013).
Limitations
Despite the fact that some of our multitrajectory groups remained statistically significant after adjustments for several important indicators, including early CP, the strength of the associations between multitrajectories and CP decreased in adolescence. One explanation is the use of a self-report questionnaire for assessing CP in adolescence. Hence, social desirability response bias (e.g., under-reporting severity/frequency) may have partially altered the associations between psychological features and CP. Another possibility could be that since CP usually peaks during adolescence (15–17 years old) (Moffitt, Reference Moffitt1993), the presence of transient CP during adolescence (i.e., adolescent-limited) in “typically developing” children could have reduced the magnitude of the effects between groups. Second, the two-trajectory model for DAS showed acceptable yet relatively low entropy, suggesting that latent classes are not highly discriminating. However, it is unlikely that this may have influenced the findings since the entropy value was close to 0.80 (Nagin, Reference Nagin2005) and that other metrics, such as AvePP and OCC, suggested good to excellent within-class cohesion. By using more complex models (i.e., higher than a two-trajectory model) would have helped us identify trajectories that are highly discriminating. Moreover, considering the sample size in the current study, a two-trajectory model for each psychological factor was chosen since increasing the number of trajectories would have substantially complexified the models, resulting in overfitted models. Consequently, future research should attempt to replicate our results with much larger data sets and more complex trajectory models. Third, while none of the items qualitatively overlapped between psychological features for trajectory groups (e.g., irritability, H/I symptoms) and CP, some constructs are known to be more closely related to CP than others (e.g., irritability vs. DAS). It remains important to acknowledge that some degree of overlap may have inflated some of the observed associations. Finally, we used the same questionnaire to assess psychological features and childhood CP. Therefore, the common method-variance bias may have affected some results observed in our study.
Conclusion
The current study aimed to investigate the developmental heterogeneity in CD population. Our results clearly suggest that children at risk for CP are a heterogeneous population. More precisely, we showed the importance of studying the developmental co-occurrence of four crucial psychological dimensions (irritability, IC, DAS, and H/I symptoms) in relation with subtypes of CP (e.g., AGG and RB), to tackle the substantial heterogeneity associated with the disorder. While the current conceptual framework of heterogeneity in CD is mostly driven by psychopathic traits (and ANX to a lesser extent), we suggest that irritability and H/I symptoms are also fundamental characteristics required to identify more homogeneous groups at risk for CD, and its subsyndromes. Researches on the equifinality (i.e., diversity of pathways leading to the same outcome) and/or multifinality (i.e., one component/experience leading to a variety of developmental outcome) (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996) of CD should take into account this heterogeneity in order to be confident about the findings. Furthermore, we argue that adopting a multidimensional specifier approach for CD seems promising for stimulating research on treatment and clinical management of children at risk for CD. Therefore, we encourage researchers to examine the multiple developmental pathways of psychological features over the current behavioral classification, as it should enable incremental progress towards unveiling the numerous etiologies underlying CDs. More precisely, we encourage researchers to replicate our findings with different samples (i.e., population-based, clinical) in order to better describe data-driven subgroups at risk for CP. As these homogeneous subgroups may show differential response to treatment, research on data-driven subgroups remains essential as it opens the possibility for targeted prevention strategies and personalized clinical practice for a better case management plan.
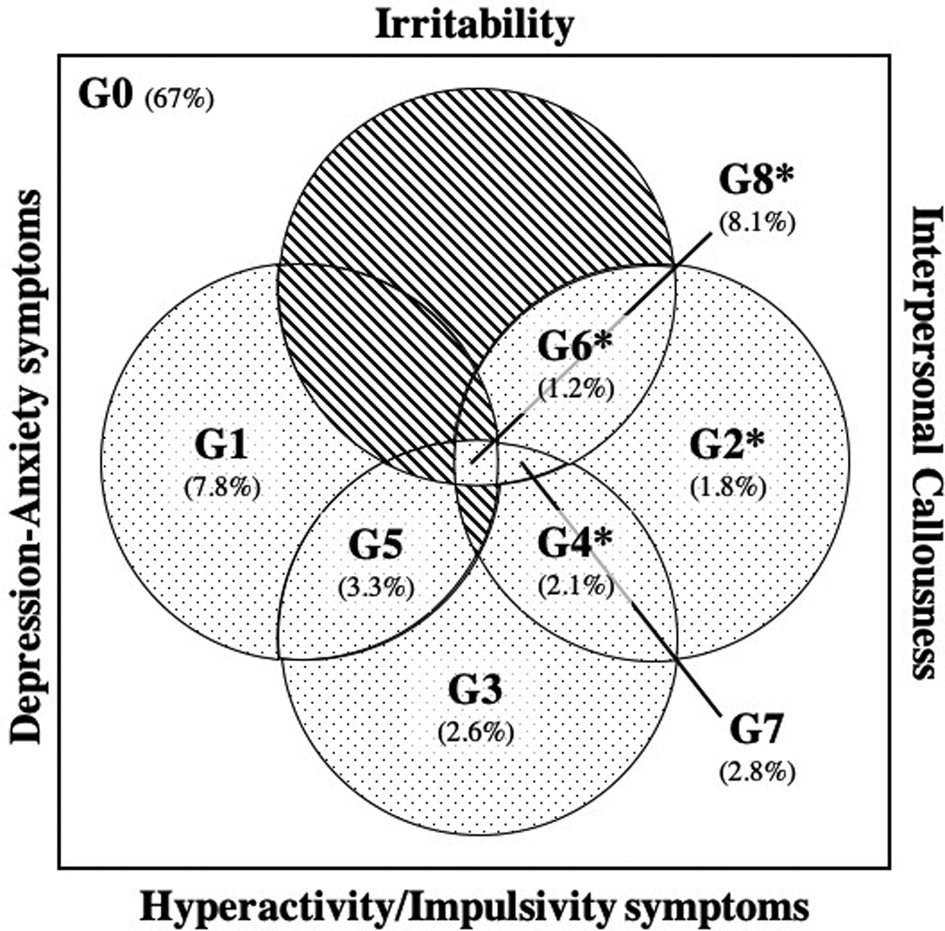
Figure 3. Overlaps between the four psychological features observed in the multitrajectory analysis. G0 = typically developing; G1 = anxious–depressive only, G2 = interpersonal callousness only; G3 = hyperactivity/impulsivity only; G4 = interpersonal callousness and hyperactivity/impulsivity, G5 = anxious–depressive and hyperactivity/impulsivity, G6 = irritable and interpersonal callousness, G7 = irritable, interpersonal callousness, and hyperactivity/impulsivity, and G8 = irritable, interpersonal callousness, hyperactivity/impulsivity, and anxious–depressive symptoms. Overlap not observed in the current study is indicated in a hatched figure.
Table 2. Prospective prediction of conduct problems in adolescence from childhood multitrajectories (n = 1,309)

Note. DAS = depressive and anxiety symptoms; IC = interpersonal callousness; H/I = hyperactivity/impulsivity symptoms.
*p < .05. **p < .01. ***p < .001.
a Group used as reference. Model 1 = adjusted for the effects of time, children's sex, and parental socioeconomic status; Model 2 = adjusted for the effects of time, children's sex, parental socioeconomic status, and conduct problems at 6 years old.
Supplementary Material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579420001650.
Acknowledgments
SP is holder of the Eli Lilly Canada Chair on schizophrenia research. JRD is holder of a scholarship from the Fonds de Recherche du Québec en Santé.
Funding Statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Conflicts of Interest
The authors have declared no conflict of interest.







