Introduction
Many patients with ear issues complain of ‘feeling plugged’, ‘clogging sensations’ or ‘pressure feelings’ in the ear, suggestive of ear fullness.Reference Sevilla, Goody, Baguley and Kasbekar1,Reference Park, Lee, Kang, Ryu, Lee and Yeo2 The feeling of ear fullness is a highly subjective symptom often found in middle-ear diseases, especially in effusion Eustachian tube dysfunction.Reference Park, Lee, Kang, Ryu, Lee and Yeo2 A feeling of ear fullness is reported by 77.0 per cent of patients with otitis mediaReference Shimotakahara, Ruby and Lampe3 and by 85.9 per cent of patients with chronic simple suppurative otitis media.Reference Baba, Yagi and Fujikura4 In particular, a feeling of ear fullness occurs frequently in patients with sensorineural hearing loss (SNHL), in 68 per cent of subjects with Ménière's disease,Reference Levo, Kentala, Rasku and Pyykko5 in 41.1 per cent of patients with acute low tone SNHLReference Park, Kim, Kim and Yeo6 and in 83.7 per cent of patients with sudden deafness.Reference Sakata and Kato7
For patients with major hearing loss or vertigo, tinnitus and dizziness, feelings of ear fullness are often ignored by the individual and physicians. But in patients with a feeling of ear fullness as the main complaint, long-term and severe ear fullness can cause anxiety, depression and other negative emotions, leading to patient isolation, autistic tendencies and reduced socialising.Reference Levo, Kentala, Rasku and Pyykko5 However, little is known about the characteristics, prognosis, severity assessments and mechanism of the feeling of ear fullness in sudden SNHL patients.
This study investigated the clinical characteristics and prognosis of patients with a feeling of ear fullness, and the relationship between a feeling of ear fullness and hearing loss in those with unilateral all-frequency sudden SNHL.
Materials and methods
Inclusion and exclusion criteria
This study used a prospective controlled research protocol. Patients with a diagnosis of unilateral all-frequency sudden SNHL, with or without ear fullness, were included in this study.
The inclusion criteria were as follows. Patients met the diagnostic criteria of the Chinese Medical Association Guidelines for the diagnosis and treatment of sudden deafness (2015),8 defined as acute idiopathic hearing loss of 20 dB or more, at all frequencies from 0.25 to 8 kHz, occurring within 72 hours. Patients had no history of sudden SNHL or otological surgery. A feeling of ear fullness was the presenting symptom in sudden SNHL patients or was the initial symptom of this disease, and patients had not received any treatments from onset to admission. Patients co-operated with objective audiology examinations and provided complete subjective severity assessments of ear fullness.
Patients with any history of external- and middle-ear related diseases, rheumatic-related disease, superior semi-circular canal dehiscence syndrome, Ménière's disease, auditory neuropathy, acoustic neuroma, nasal sinus related diseases, temporomandibular joint disorder related diseases, cardiovascular diseases or psychiatric diseases were excluded.
Patients and follow up
Initially, 121 patients with unilateral all-frequency sudden SNHL diagnosed at the Hunan Provincial People's Hospital between June 2016 and June 2019 were enrolled. We then excluded 17 patients based on the above exclusion criteria, including 3 patients with successive onset of binaural hearing loss, 1 patient with auditory nerve occupying lesions detected by internal auditory magnetic resonance imaging (MRI), 2 patients with chronic rhinosinusitis, 3 patients with cardiovascular disease, and 8 patients with incomplete objective audiology examination or follow up data. Thus, a total of 104 patients were recruited and followed up.
All patients were followed up for one month using the WeChat messaging mobile phone application. Patients who failed to attend timely out-patient follow-up examinations were contacted by telephone.
Examination and treatments
The following data were collected for all patients: subjective grading and visual analogue scale (VAS) for feeling of ear fullness, uniform ear endoscopy, pure tone hearing threshold, acoustic anti-Eustachian tube function test, otoacoustic emission (transient evoked otoacoustic emissions, distortion product otoacoustic emissions), auditory brainstem response (ABR), and MRI of the inner ear. Pure tone hearing threshold values and feeling of ear fullness VAS scores were collected after one week and one month of treatment. The data collected at one month of treatment were taken as the final recovery results.
Based on guideline recommendations, the main treatment strategy for patients was intravenous injection of ginkgo biloba extract and dexamethasone over a course of 10 days: ginkgo biloba extract at 20 ml/day over 10 days; and dexamethasone at 10 mg/day over 5 days, reduced to 10 mg/day for 3 days, and then reduced to 5 mg/day for 2 days before withdrawal.8 All patients received concomitant hyperbaric oxygen treatment for 10 days. Defibrinogen drugs were not used.
Hearing threshold grading and treatment evaluation
Hearing threshold grades were based on standards issued by The World Health Organization's Programme for the Prevention of Deafness and Hearing Impairment (1997),Reference Smith9 which used a pure tone average of four frequencies (0.5 kHz, 1.0 kHz, 2.0 kHz and 4.0 kHz). Specifically, a pure tone average of 81 dB HL or higher represents ‘extremely severe’ hearing loss, 61–80 dB HL reflects ‘severe’ hearing loss, 41–60 dB HL represents ‘moderate’ hearing loss, 26–40 dB HL reflects ‘slight’ hearing loss, and 25 dB HL or lower represents ‘normal’ hearing. If the patient did not respond to the maximum output of the audiometer, values were assigned to each frequency according to Table 1.
Table 1. Assigned hearing threshold values for each frequency when no response to maximum audiometer output

We evaluated treatment outcomes with reference to the Chinese guidelines for the diagnosis and treatment of sudden deafness (2015): ‘healed’ reflects pure tone thresholds, in patients with previously impaired hearing, reaching those thresholds of the normal unaffected ear; ‘significant’ reflects pure tone thresholds of impaired hearing patients improving by 30 dB or higher; ‘effective’ reflects pure tone thresholds of impaired hearing patients improving by 15 dB or higher, but less than 30 dB; and ‘ineffective’ reflects pure tone thresholds of impaired hearing patients improving by less than 15 dB.8
Ear fullness grading and treatment evaluation
Visual analogue scales have been used in many studies, but the exact nature of how patients make evaluations using these scales is unknown. Similarly, it is unclear how surgeons responding to questionnaires measure ear fullness.Reference Levo, Kentala, Rasku and Pyykko5,Reference Zhai, Zhang, Zhang, Steyger and Dai10,Reference Peng11
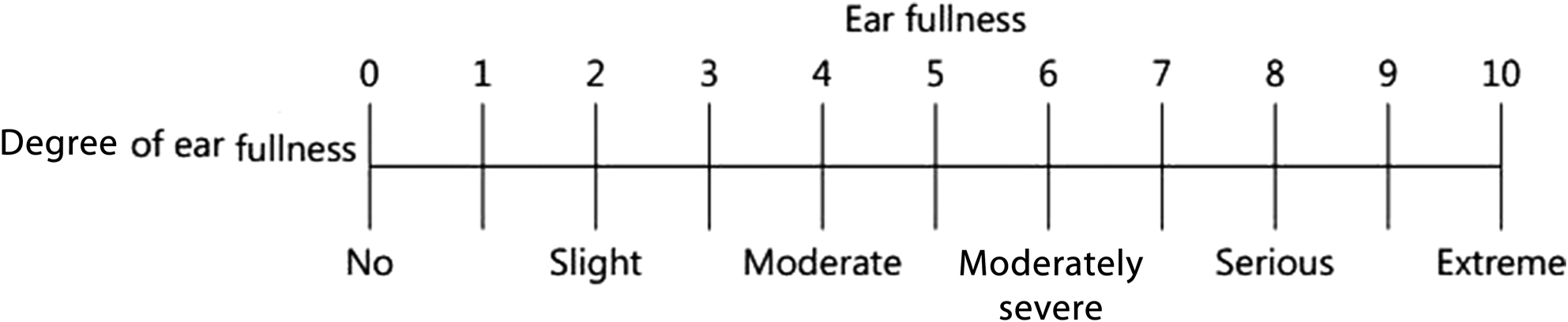
From this relevant literature, we summarised clinical experiences, patient complaints and VAS scores to classify ear fullness over five grades, using a points system (Figure 1): ‘slight’ (1–2 points) for slight ear fullness or haziness, not affecting patient mood or daily activities, with no therapy required; ‘moderate’ (3–4 points) for ear fullness, slightly affecting mood and socialising, but the patient is not actively seeking therapy; ‘moderately severe’ (5–6 points) for obvious ear fullness, affecting mood, socialising and work, for which the patient is actively seeking therapy; ‘serious’ (7–8 points) for obvious irritating ear fullness, distress and upset, affecting mood, socialising and work, for which the patient is seeking immediate therapy; and ‘extremely serious’ (9–10 points) for obvious irritating ear fullness, depression, irritability and anxiety, because of which the patient cannot work or socialise, and has a very strong desire to seek therapy.
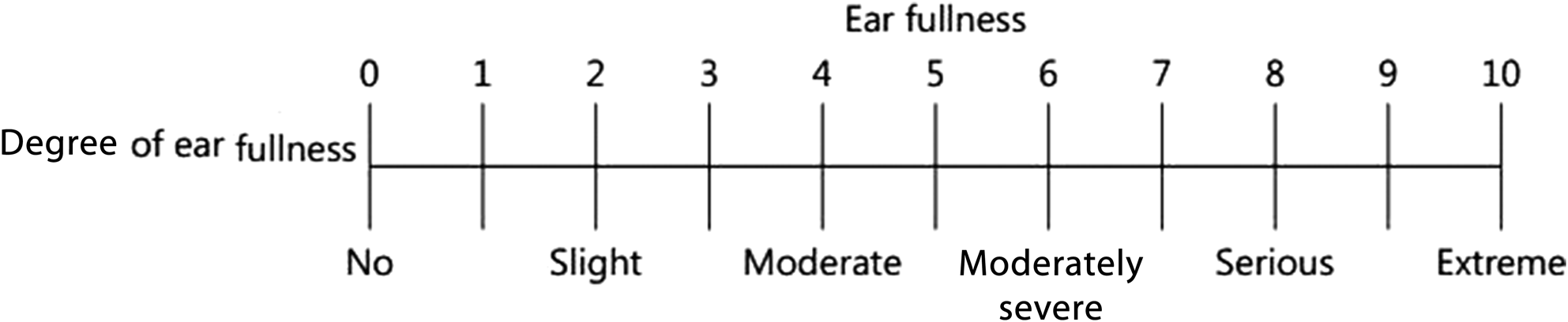
Fig. 1. Visual analogue scales for ear fullness.
Changes in ear fullness symptoms were categorised according to four grades: ‘healed’ meant that feeling of ear fullness had totally disappeared; ‘significant’ indicated that the VAS score had improved by 4 points or more; ‘effective’ suggested that the VAS score had improved by 2 points or more but less than 4 points; and ‘ineffective’ reflected that the VAS score had improved by less than 2 points.
Statistical methods
All statistical analyses were performed using SPSS® software (version 13.0). Statistical analyses were conducted using Mann–Whitney tests, t-tests, chi-square tests and Spearman correlation tests. All reported p-values were two-sided, and those less than 0.05 were considered statistically significant.
Results
Patient information
In total, 104 patients with unilateral all-frequency sudden SNHL were included in the study, with 53 left ears (51 per cent) and 51 right ears (49 per cent), with a left-to-right ear ratio of 1.04:1. Our study included 50 males (45 per cent) and 54 females (55 per cent), with a male-to-female ratio of 0.93:1. Patients had a mean age of 46.2 ± 16.1 years (range, 23–65 years). The mean disease duration was 4.1 ± 3.3 days (range, 1–9 days). The degree of hearing loss was mild in 5 patients (4.8 per cent), moderate in 24 (23.1 per cent), severe in 43 (41.4 per cent) and extremely severe in 32 (30.8 per cent).
A total of 56 patients with unilateral all-frequency sudden SNHL accompanied by ear fullness were enrolled into the ‘ear fullness group’, and 48 patients without ear fullness were included in the ‘without ear fullness group’. No significant differences were observed between groups in terms of: age (t = 1.566), gender (χ2 = 0.001), duration of disease (t = 0.057), side of affected ear (χ2 = 0.033), grade of hearing threshold (Z = −0.180) or ABR results (χ2 = 0.001) (all p > 0.05) (Table 2).
Table 2. General comparisons between patient groups

M = males; F = females; L = left; R = right; SD = standard deviation
Ear fullness grading and hearing threshold
Positive correlations were observed between the subjective grading of ear fullness and hearing thresholds in patients with unilateral all-frequency sudden SNHL accompanied by a feeling of ear fullness (r = 0.599, p < 0.001) (Table 3).
Table 3. Relationship between hearing loss and ear fullness

Hearing recovery and ear fullness
No significant differences were observed in total effective rates of hearing recovery between all-frequency sudden SNHL patients accompanied by ear fullness and patients without ear fullness, after one month of treatment (Z = −0.641, p = 0.521) (Table 4).
Table 4. Relationship between hearing recovery and ear fullness

*The statistical test values for total hearing recovery efficiency for the group with ear fullness when compared to the group without ear fullness are: Z = −0.641 and p = 0.521
Ear fullness recovery
After one week of treatment, 43 per cent of patients (24 out of 56) showed complete recovery from ear fullness, 43 per cent (24 out of 56) showed partial recovery and 14 per cent (8 out of 56) showed no change.
After one month of treatment, 86 per cent of patients (48 out of 56) showed complete recovery from ear fullness, 7 per cent (5 out of 56) showed partial recovery and 5 per cent (3 out of 56) showed no change. Of the three patients who showed no change, two complained of hearing threshold fluctuations, and occasionally experiencing aggravated hearing loss and feeling of ear fullness; the other patient's hearing threshold improved by approximately 30 dB HL but they still experienced ear fullness.
Overall, patients showed greater improvement in ear fullness after one month of treatment compared with one week (Z = −4.474, p < 0.001) (Table 5).
Table 5. Ear fullness recovery

Ear fullness recovery and hearing improvement
There was no correlation between feeling of ear fullness recovery and hearing recovery (r = 0.040, p = 0.769) (Table 6).
Table 6. Relationship between hearing recovery and ear fullness recovery

Discussion
The feeling of ear fullness is a common symptom in patients with sudden SNHL. Long-term, severe ear fullness can have a negative impact on emotions and quality of life, and may lead to a prognosis of sudden deafness.Reference Levo, Kentala, Rasku and Pyykko5,Reference Kim, Min, Lee, Park and Choi12 Multicentre studies have shown that 55 per cent of patients with sudden SNHL and 55 per cent with all-frequency sudden SNHL complain of ear fullness.13 The feeling of ear fullness often occurs on the same side as hearing loss, although small numbers of patients have mild ear fullness on the normal hearing side.
As specified by Chinese and German guidelines, sudden SNHL patients are categorised into subgroups; the variation in audiographic features may indicate that different disease mechanisms are in play.8,Reference Michel14 In order to avoid the mutual interference of binaural hearing loss and the varying mechanisms underlying different audiograms, which may affect the characteristic feeling of ear fullness, we selected only those patients with unilateral all-frequency sudden SNHL for inclusion in the study. A total of 56 patients with unilateral all-frequency sudden SNHL accompanied by a feeling of ear fullness were enrolled. The patients consisted of 27 males and 29 females (a male-to-female ratio of 0.93:1), with 53 left ears (51 per cent) and 51 right ears (49 per cent), and 3 ears with mild feeling of ear fullness on the healthy side. No significant differences were observed between the two groups in terms of: age, gender, side of affected ear, duration of disease, deaf ears, degree of hearing loss or auditory brainstem evoked potential results (Table 2). This suggests that none of these factors were predictors for the feeling of ear fullness.
The feeling of ear fullness is a subjective sensation that is difficult to evaluate by objective indicators. Equally, exact qualitative and quantitative assessments of ear fullness are lacking in clinical practice. Zhai et al. asked participants to use a 1–10-point VAS to assess the presence or absence and annoyance levels of ear fullness.Reference Zhai, Zhang, Zhang, Steyger and Dai10 These authors acquired data on how ear fullness changed after intratympanic gentamicin injection in patients with intractable Ménière's disease. In another study, the severity of ear fullness in subjects with Ménière's disease was divided into five levels: 0 = no fullness, 1 = weak, 2 = moderate, 3 = strong and 4 = very strong.Reference Levo, Kentala, Rasku and Pyykko5 In order to assess levels of ear fullness in patients with temporomandibular joint disorder, a three-level grading system was established by Peng et al. based on patients’ perception of symptoms, whereby 1 = mild, 2 = moderate and 3 = severe.Reference Peng11 Treatment was considered effective if the ear fullness grade was reduced by at least 1. A grade reduction of less than 1 or the recurrence of ear fullness was indicative of ineffective treatment. However, the exact nature of how patients make evaluations using these scales is unknown, and it was not stated how surgeons who responded to the questionnaires measured ear fullness.
The current study summarised clinical experiences, patient complaints and literature VAS scores in order to classify ear fullness into five grades: ‘slight’, ‘moderate’, ‘moderately severe’, ‘serious’ and ‘extremely serious’. Similarly, changes in ear fullness symptoms were categorised at four grading levels: ‘healed’, ‘significant’, ‘effective’ and ‘ineffective’.
In this study, the feeling of ear fullness severity in patients with all-frequency sudden SNHL was mainly concentrated in the moderate and serious ear fullness grading categories (43 out of 56). In the study by Peng et al., 75 per cent of patients with temporomandibular joint disorder suffered moderate ear fullness, and 17 per cent of patients suffered severe ear fullness.Reference Peng11 Levo et al. observed ear fullness in 68 per cent of subjects with long-standing Ménière's disease, with 30 per cent of subjects considering their ear fullness moderate or severe.Reference Levo, Kentala, Rasku and Pyykko5 These subjects felt that the feeling of ear fullness affected their daily lives; they did not watch television, go shopping alone, do household tasks, help others or contact friends. Similar to these two studies, our study also identified that patients with all-frequency sudden SNHL accompanied by a severe feeling of ear fullness had restricted their participation, motility and communication, leading to isolation, even though other cardinal symptoms (i.e. mainly vertigo attacks, hearing loss and tinnitus) were considered more important.
In this study, the grading of hearing loss in patients with all-frequency sudden SNHL was mainly concentrated in the severe and extremely severe categories (40 out of 56). Positive correlations were observed between the subjective grading of ear fullness and hearing thresholds. Sakata et al. showed that the feeling of ear fullness in patients with acute SNHL was not associated with either the audiogram shape or the hearing threshold at the first medical examination when it appears, and it appears in a qualitative manner like an on/off switch.Reference Sakata, Higuchi, Ueno and Nakagawa15 Levo et al. found that hearing loss and vertigo were not predictors of ear fullness. However, neither of these studies reported on the relationship between ear fullness severity and hearing threshold, which remains a topic for further study.Reference Levo, Kentala, Rasku and Pyykko5,Reference Sakata, Higuchi, Ueno and Nakagawa15 Additionally, there may be relationships between the degree of hearing loss, subjective grading of ear fullness and bad mood. The development of improved reliability scales for subjective grading of the feeling of ear fullness will require further exploration.
The mechanisms underlying ear fullness are unknown. Abnormalities in any part of the auditory pathway, from the external ears to the inner ear to the auditory cortex, as well as other organ abnormalities to innervations of the ear, can produce ear fullness symptoms.Reference Park, Lee, Kang, Ryu, Lee and Yeo2,Reference Ugalde, Anjum, Lo Presti and Tolentino16 Park et al. showed that ear fullness was a symptom most frequently diagnosed as a middle-ear disease (55 per cent), followed by an inner-ear disorder (22 per cent).Reference Park, Lee, Kang, Ryu, Lee and Yeo2 In addition, 13.4 per cent of patients could not be definitively diagnosed. We excluded patients with middle-ear disease based on medical history, physical examination, otoscopy, acoustic impedance, Eustachian tube function measurement and thin-slice computed tomography.
In our study, the total effective rate of hearing recovery in patients with all-frequency sudden SNHL was 61 per cent (63 out of 104). No significant differences were observed in the effectiveness of hearing recovery between patients with and without a feeling of ear fullness. These findings are consistent with Wang et al., and suggest that the feeling of ear fullness is not a prognostic indicator for all-frequency sudden SNHL.Reference Wang, Liu, Xie, Ren, Yin and Ren17
Ninety-five per cent of patients (53 out of 56) showed partial recovery or complete recovery, and 86 per cent (48 out of 56) showed complete recovery of ear fullness, after one month of treatment. This demonstrates a good prognosis for those with a feeling of ear fullness accompanied by all-frequency sudden SNHL, which is in agreement with a recent multicentre report.13
Most patients with hearing recovery had normal ear sensation restored. Some patients with unrecovered hearing had complete recovery from the feeling of ear fullness, whereas a few patients with complete hearing recovery showed no relief from the feeling of ear fullness. Non-parametric Spearman's rank correlation coefficient tests revealed no correlation between the feeling of ear fullness recovery and hearing recovery.
Ugalde et al. reported the onset of myocardial infarction with ear fullness as an initial symptom in one patient.Reference Ugalde, Anjum, Lo Presti and Tolentino16 In this case, stimulation of the heart nerve branch of the vagus nerve entering the spinal tract nucleus near the medulla caused referred ear fullness by the auricular nerve branch of the vagus nerve (also entering the spinal tract nucleus), based on the convergence-projection theory.Reference Keniston, Henderson and Meredith18 This theory suggests that the central nervous system cannot differentiate between stimuli that converge on common sensory pathways.
Sakata et al. suggested the that feeling of ear fullness in acute SNHL may originate from modulations of somatosensory abilities rather than organic lesions of the cochlea.Reference Sakata, Higuchi, Ueno and Nakagawa15 With the emergence of hearing loss, modulation of the auditory pathway may somehow affect the somatosensory pathway on a cortical or subcortical level.Reference Lall19 If modulation of the auditory pathway produces a stimulatory action in the somatosensory pathway, the somatosensory cortex may become excited, resulting in the feeling of ear fullness.Reference Sakata, Higuchi, Ueno and Nakagawa15 Data from this study may suggest that recovery from the feeling of ear fullness is not entirely consistent with improved hearing.
In this study, 48 patients showed complete recovery of the feeling of ear fullness after treatment for one month(Table 5), whereas 24 patients with a residual feeling of ear fullness showed complete recovery after treatment for one week. We speculate that the disappearance of the feeling of ear fullness in more patients after one month of treatment may be related to the natural habituation to the feeling of ear fullness along with a relatively steady audiogram, as occurs for tinnitus.Reference Cima20
Two patients complained of hearing fluctuations and occasionally experienced aggravated hearing loss and feeling of ear fullness, and one patient showed a hearing threshold improvement of about 30 dB but still felt ear fullness after one month of treatment. We followed these three patients for six months and found that the feeling of ear fullness gradually disappeared over time, but no follow-up audiograms were obtained. We speculate that a feeling of ear fullness which has not recovered after one month of treatment may be related to an unstable audiogram and the lack of adaptation to ear fullness. Perhaps the adaptation to ear fullness has a certain prompting effect on the stability of hearing, but further observation and exploration are needed.
• Hearing loss was positively correlated with ear fullness in patients with all-frequency sudden sensorineural hearing loss (SNHL) and ear fullness
• The presence of ear fullness was not a prognostic sign of hearing for all-frequency sudden SNHL patients
• The likelihood of ear fullness recovery is good, but is poorly associated with hearing recovery
Conclusion
Studies on the feeling of ear fullness related to sudden SNHL are limited, and the mechanism underlying the feeling of ear fullness has yet to be clarified. Similarly, an improved reliability scale for the subjective grading of the feeling of ear fullness is also lacking.
Our study generated three insights regarding the feeling of ear fullness in all-frequency sudden SNHL. First, the degree of hearing loss was positively correlated with the degree of ear fullness in patients with all-frequency sudden SNHL accompanied by a feeling of ear fullness. Second, the presence of the feeling of ear fullness was not a prognostic sign of hearing for all-frequency sudden SNHL patients. Third, the likelihood of recovery from the feeling of ear fullness was good, but it showed no correlation with hearing recovery.
Acknowledgements
The authors thank the patients who participated in this study. We thank the Hunan Province Technology Innovation Guidance Program – Clinical Medical Technology Innovation Guidance Project for funding the study (project number: 2018SK50705).
Competing interests
None declared