Attention deficit hyperactivity disorder (ADHD) symptoms often emerge in the preschool years (Faraone et al., Reference Faraone, Perlis, Doyle, Smoller, Goralnick, Holmgren and Sklar2005) and persist into middle childhood, putting the child at risk for multiple negative outcomes such as social dysfunction, academic difficulties, and family dysfunction (Barkley, Reference Barkley2014; Breaux & Harvey, Reference Breaux and Harvey2018). ADHD symptoms can persist into adolescence and adulthood, and are associated with functional impairments over time, such as school dropout, low employment, antisocial behaviors, and drug use (Barkley, Murphy, & Fischer, Reference Barkley, Murphy and Fischer2010; Sasser, Kalvin, & Bierman, Reference Sasser, Kalvin and Bierman2016). Given these negative consequences, it is important to identify the factors associated with ADHD symptoms in order to develop evidence-based prevention programs. Furthermore, prevention in childhood is important considering the persistence of some impairments associated with ADHD (e.g., lower education) into adolescence and adulthood despite declining ADHD symptoms (Barkley, Reference Barkley2016). Among factors that can be targeted by prevention efforts, parenting practices and child temperament have been shown to be associated with ADHD symptoms (Abulizi et al., Reference Abulizi, Pryor, Michel, Melchior, van der Waerden and Grp2017; Breaux & Harvey, Reference Breaux and Harvey2018; Einziger et al., Reference Einziger, Levi, Zilberman-Hayun, Auerbach, Atzaba-Poria, Arbelle and Berger2018; Tung, Brammer, Li, & Lee, Reference Tung, Brammer, Li and Lee2015). Studies have also repeatedly shown that the interaction between parenting practices and child temperament can predict children's adjustment (Slagt, Dubas, Dekovic, & van Aken, Reference Slagt, Dubas, Dekovic and van Aken2016). However, research on the interaction between temperament and parenting in the prediction of children's ADHD symptoms specifically is lacking. Research on those interactions is important because it allows the identification of children most and least likely to benefit from prevention programs. Accordingly, the purpose of the present study is to examine the interaction between parenting practices and the temperament dimension of inhibitory control in order to predict ADHD symptoms, while considering theoretical models that can explain these interactions.
Parenting Practices and ADHD Symptoms
Environmental factors such as the family have an important role in the development of ADHD symptoms, and understanding the way in which parents can help their children regulate their behavior is crucial to understanding the diverse developmental trajectories of ADHD symptoms. Several longitudinal studies showed that negative parenting practices predict children's ADHD symptoms (Breaux & Harvey, Reference Breaux and Harvey2018; Demmer, Puccio, Stokes, McGillivray, & Hooley, Reference Demmer, Puccio, Stokes, McGillivray and Hooley2018; Hawes, Dadds, Frost, & Russell, Reference Hawes, Dadds, Frost and Russell2013; Keown, Reference Keown2012; Tung et al., Reference Tung, Brammer, Li and Lee2015). For example, parents’ (90% mothers) corporal punishment measured when children were between 5 and 10 years of age predicted higher levels of offspring ADHD symptoms 2 years later (Tung et al., Reference Tung, Brammer, Li and Lee2015). Another study showed that overreactive parenting, such as expressions of anger, meanness, and irritability, positively predicted ADHD symptoms across the preschool years (Breaux & Harvey, Reference Breaux and Harvey2018).
As for positive parenting, several studies have found that higher levels of parental involvement, maternal warmth/sensitivity, and observed praise are associated with lower levels of ADHD symptoms (Cussen, Sciberras, Ukoumunne, & Efron, Reference Cussen, Sciberras, Ukoumunne and Efron2012; Ellis & Nigg, Reference Ellis and Nigg2009; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013; Keown, Reference Keown2012; Tung et al., Reference Tung, Brammer, Li and Lee2015; Ullsperger, Nigg, & Nikolas, Reference Ullsperger, Nigg and Nikolas2016). One study of 4- to 10-year-old children found that higher levels of maternal warmth/involvement were associated with lower levels of hyperactivity and inattention 12 months later, but only for younger children (age 5) and not for older children (age 6.5 and age 8; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013). However, cross-sectional studies found negative associations between parenting and ADHD at later ages. For example, a study of 6- to 9-year-old children (average age 7.5) found that parental warmth was associated with less ADHD symptoms (Cussen et al., Reference Cussen, Sciberras, Ukoumunne and Efron2012). Similarly, a study of 6- to 12-year-old children (average age 9.5) found that maternal involvement was associated with lower ADHD symptoms (Ellis & Nigg, Reference Ellis and Nigg2009).
It is also important to consider how parenting is assessed. Although observational measures are known to be the gold standard for assessing parent behaviors (Hawes & Dadds, Reference Hawes and Dadds2006), among the above studies, parenting practices were mainly measured using mother-reported questionnaires. In contrast, the constructs most frequently assessed using observational measures include dimensions of responsive caregiving such as contingent responsiveness or sensitivity (Lotzin et al., Reference Lotzin, Lu, Kriston, Schiborr, Musal, Romer and Ramsauer2015). Positive parent behaviors such as scaffolding, structuring, and encouraging are also better assessed by observational tools (Lotzin et al., Reference Lotzin, Lu, Kriston, Schiborr, Musal, Romer and Ramsauer2015). In the few instances when observational measures were used in the studies reviewed above, they were limited to a few contexts (e.g., 5-min play and clean-up task; Breaux & Harvey, Reference Breaux and Harvey2018). Knowing that ADHD symptoms reflect difficulties that impair the children's ability to regulate and organize their behavior in different situations (Barkley, Reference Barkley1997, Reference Barkley2003), it is important to measure parenting practices across multiple contexts that require parent–child interactions. Still, although observational measures are more reliable, their advantages are lessened when the construct is difficult to observe or occurs at a very low frequency (Gardner, Reference Gardner2000). Understandably, coercive parenting is more difficult to observe as the parent can knowingly avoid using this type of practice during the observation period and establishing contexts to elicit coercive parenting would not be ethical or acceptable. Therefore, observations of parenting in multiple contexts are ideal, but parent reports are more likely to be representative of daily negative parenting practices than daily positive parenting practices.
Temperament and ADHD Symptoms
Although parenting has been shown to predict ADHD symptoms, there are both individual and environmental factors that can contribute to their development. Among individual factors, temperament could be key in understanding and preventing the development of ADHD symptoms. Temperament traits are thought to have some genetic basis and influence children's experiences and behaviors (Goldsmith et al., Reference Goldsmith, Buss, Plomin, Rothbart, Thomas, Chess and McCall1987; Rothbart, Ahadi, & Evans, Reference Rothbart, Ahadi and Evans2000). They refer to relatively stable individual differences in reactivity and self-regulation emerging early in life. The reactivity domain represents differences in responsivity to environmental changes and variations in the arousal level of affective, motor, and sensory response systems. Self-regulation refers to neural and behavioral processes that can either increase or decrease reactivity (Rothbart, Ahadi, Hershey, & Fisher, Reference Rothbart, Ahadi, Hershey and Fisher2001).
Effortful control is a dimension of self-regulation defined as the ability to inhibit a dominant response in order to perform a subdominant response. Although effortful control is often examined in studies, its subdimensions should be examined as it has been shown that they may be related differently to ADHD symptoms (De Pauw & Mervielde, Reference De Pauw and Mervielde2010) and that specific dimensions of temperament may be more developmentally informative than more general dimensions (Clifford, Lemery-Chalfant, & Goldsmith, Reference Clifford, Lemery-Chalfant and Goldsmith2015; Rioux, Castellanos-Ryan, Parent, & Séguin, Reference Rioux, Castellanos-Ryan, Parent and Séguin2016). One subdimension of effortful control is inhibitory control, which is the capacity to plan and suppress inappropriate actions under instructions or in novel or uncertain situations (Rothbart et al., Reference Rothbart, Ahadi and Evans2000, Reference Rothbart, Ahadi, Hershey and Fisher2001). Regarding ADHD, it has been suggested that children who are low in inhibitory control, and thus have difficulty voluntarily restraining their impulsivity, may be most vulnerable to develop ADHD symptoms (Derryberry & Rothbart, Reference Derryberry and Rothbart1997; Nigg, Goldsmith, & Sachek, Reference Nigg, Goldsmith and Sachek2004). Although the present study focuses on inhibitory control, literature on effortful control will also be reviewed, as few studies have focused specifically on inhibitory control.
Empirical research supports the suggested association between inhibitory control and ADHD symptoms. Several cross-sectional studies have shown that inhibitory control is negatively associated with ADHD symptoms during childhood (Auerbach et al., Reference Auerbach, Berger, Atzaba-Poria, Arbelle, Cypin, Friedman and Landau2008; Foley, McClowry, & Castellanos, Reference Foley, McClowry and Castellanos2008; Gagne, Saudino, & Asherson, Reference Gagne, Saudino and Asherson2011; Gomez, Kyriakides, & Devlin, Reference Gomez, Kyriakides and Devlin2014; Herzhoff, Tackett, & Martel, Reference Herzhoff, Tackett and Martel2013; Samyn, Roeyers, & Bijttebier, Reference Samyn, Roeyers and Bijttebier2011). Although fewer longitudinal studies have been conducted, there is also prospective evidence that inhibitory control (Lemery, Essex, & Smider, Reference Lemery, Essex and Smider2002) and effortful control (Einziger et al., Reference Einziger, Levi, Zilberman-Hayun, Auerbach, Atzaba-Poria, Arbelle and Berger2018; Willoughby, Gottfredson, Stifter, & Family Life Project Investigators, Reference Willoughby, Gottfredson and Stifter2017) play a role in the prediction of ADHD symptoms.
Interactions Between Temperament and Parenting
Although multiple studies have shown the predictive role of parenting practices and temperament in the development of ADHD symptoms, the interaction between parenting and temperament can also predict children's developmental outcomes (Slagt et al., Reference Slagt, Dubas, Dekovic and van Aken2016). In other words, some children can be more or less sensitive to parenting behaviors depending on their temperament traits. A meta-analysis by Slagt et al. (Reference Slagt, Dubas, Dekovic and van Aken2016) reviewed longitudinal and experimental studies focused on child temperament as a moderator of the association between parenting and diverse developmental outcomes, including externalizing problems, with ADHD being considered a form of externalizing problems (Castellanos-Ryan et al., Reference Castellanos-Ryan, Struve, Whelan, Banaschewski, Barker and Bokde2014; Forns, Abad, & Kirchner, Reference Forns, Abad, Kirchner and Levesque2011). Moderation of parenting not only by difficult temperament but also by specific temperament dimensions including effortful control was reviewed. Results showed that while effortful control did not moderate the association between parenting and positive child adjustment, it significantly moderated the association between parenting and negative child adjustment. However, effortful control moderated positive parenting only, and not negative parenting. The significant effects showed that positive parenting was more strongly associated with externalizing problems when effortful control was low (Slagt et al., Reference Slagt, Dubas, Dekovic and van Aken2016). However, studies did not examine inhibitory control specifically. Furthermore, no study has tested this interaction in the prediction of ADHD symptoms during childhood. It is important to examine this interaction because ADHD symptoms have unique behavioral and cognitive aspects differentiating them from other externalizing behaviors such as aggression and conduct problems (Nigg, Hinshaw, & Huang-Pollock, Reference Nigg, Hinshaw, Huang-Pollock, Cicchetti and Cohen2015). Examining this interaction is also essential for a better understanding of the etiology of ADHD, which can lead to optimized prevention and intervention approaches adapted to the particularities of this developmental syndrome.
Temperament × Parenting Interactions: Theoretical Models
The concept that individuals can respond differently in the same environment is broadly documented in the literature and well demonstrated through multiple theoretical models positing that children vary in their sensitivity to parenting, specifically in terms of their temperament traits (e.g., Kiff, Lengua, & Bush, Reference Kiff, Lengua and Bush2011; Kim & Kochanska, Reference Kim and Kochanska2012; Ramchandani, van IJzendoorn, & Bakermans-Kranenburg, Reference Ramchandani, van IJzendoorn and Bakermans-Kranenburg2010; Rioux, Castellanos-Ryan, Parent, Vitaro, et al., Reference Rioux, Castellanos-Ryan, Parent, Vitaro, Tremblay and Séguin2016; Van Zeijl et al., Reference Van Zeijl, Mesman, Stolk, Alink, van IJzendoorn, Bakermans-Kranenburg and Koot2007). Three theoretical models can explain how individual characteristics (e.g., inhibitory control) moderate the influence of negative and positive environments (e.g., negative and positive parenting). The diathesis-stress model (Monroe & Simons, Reference Monroe and Simons1991; Zuckerman, Reference Zuckerman1999) posits that some individuals show an increased vulnerability to adverse environments exclusively. For example, if this model is supported, negative parenting may be associated with higher ADHD symptoms for children with certain levels of inhibitory control only. The vantage sensitivity model posits that some individuals show an increased sensitivity to positive environments exclusively (Pluess & Belsky, Reference Pluess and Belsky2013). If this model is supported, positive parenting may be associated with lower ADHD symptoms for children with certain levels of inhibitory control only. Finally, the differential susceptibility model suggests that some individuals show an increased susceptibility to both positive and negative environments (Belsky & Pluess, Reference Belsky and Pluess2009, Reference Belsky and Pluess2013). Thus, it represents both diathesis-stress and vantage sensitivity as a function of the same individual and environmental factors (Pluess, Reference Pluess2015). For example, if this model is supported, children with a certain level of inhibitory control would show higher ADHD symptoms compared to other children when exposed to negative parenting and lower ADHD symptoms compared to other children when exposed to positive parenting.
The meta-analysis by Slagt et al. (Reference Slagt, Dubas, Dekovic and van Aken2016) examined these models, but interactions between effortful control and parenting in the prediction of externalizing problems did not support any of the three models. However, only four reviewed studies examined effortful control as a potential sensitivity marker in the prediction of externalizing behaviors, and the results from the literature were mixed (Slagt et al., Reference Slagt, Dubas, Dekovic and van Aken2016). Furthermore, as previously mentioned, no study has examined these interactions with inhibitory control and in the prediction of ADHD symptoms specifically. Decomposing and analyzing these interactions according to the diathesis-stress, vantage sensitivity, and differential susceptibility models can lead to a better understanding of ADHD symptoms etiology through a theoretical explanation.
The Structure of ADHD Symptoms
Although a majority of the research cited above looked at ADHD globally, the etiology and consequences of ADHD can differ by subtype. Of note, children with the hyperactivity-impulsivity subtype were shown to have more externalizing problems and to experience more peer problems while those with the inattention subtype were shown to experience more academic and learning impairments, and to be more socially withdrawn (Garner et al., Reference Garner, O'Connor, Narad, Tamm, Simon and Epstein2013; Gaub & Carlson, Reference Gaub and Carlson1997; Hodgens, Cole, & Boldizar, Reference Hodgens, Cole and Boldizar2000). Multiple models have been proposed to account for the multidimensionality of ADHD symptoms, and several studies have shown that the model with the best fit for these symptoms was a bifactor model (e.g., Gibbins, Toplak, Flora, Weiss, & Tannock, Reference Gibbins, Toplak, Flora, Weiss and Tannock2012; Martel, von Eye, & Nigg, Reference Martel, von Eye and Nigg2010; Normand, Flora, Toplak, & Tannock, Reference Normand, Flora, Toplak and Tannock2012; Toplak et al., Reference Toplak, Sorge, Flora, Chen, Banaschewski, Buitelaar and Faraone2012; Willoughby, Blanton, & Family Life Project Investigators, Reference Willoughby and Blanton2015), in which symptoms load both on a general ADHD factor and on specific hyperactivity-impulsivity and inattention factors. This model thus allows the simultaneous examination of risk factors related to the general ADHD factor, or the common variance shared across all symptoms, as well as risk factors predicting variance specific to hyperactivity-impulsivity or inattention symptoms.
Some studies have already shown that these three ADHD factors (i.e., general ADHD, specific hyperactivity-impulsivity, and specific inattention) are predicted by different risk factors (e.g., Gomez et al., Reference Gomez, Kyriakides and Devlin2014; Martel, Roberts, Gremillion, von Eye, & Nigg, Reference Martel, Roberts, Gremillion, von Eye and Nigg2011; Ogg, Bateman, Dedrick, & Suldo, Reference Ogg, Bateman, Dedrick and Suldo2016). In terms of the variables of interest for the present study, research on the association between the common and unique variance of hyperactivity-impulsivity and inattention with parenting is lacking, but their association with inhibitory control and effortful control has been examined. One study of children found that low effortful control was associated with the general ADHD factor and the specific hyperactivity-impulsivity factor, but not with the specific inattention factor (Martel et al., Reference Martel, Roberts, Gremillion, von Eye and Nigg2011), and one study of adults showed that low inhibitory control was only associated with the specific hyperactivity-impulsivity factor (Gomez et al., Reference Gomez, Kyriakides and Devlin2014). A study looking at a clinical measure of inattention, hyperactivity-impulsivity, and their combination, but without extracting their unique and common variance, also suggested that inhibitory control predicts overall ADHD as well as unique hyperactivity-impulsivity symptoms in childhood (Herzhoff et al., Reference Herzhoff, Tackett and Martel2013).
Objectives of the Present Study
The objective of the present study was to examine whether the interaction between parenting practices and inhibitory control predicts the common and/or unique variance of hyperactivity-impulsivity and inattention, and whether this interaction supports the diathesis-stress, vantage sensitivity, or differential susceptibility model. More specifically, we tested whether inhibitory control, measured at 6 years of age, moderates the link between parenting (positive parenting observed at 4 years of age and negative parenting reported at 5 years of age) and hyperactivity-impulsivity and inattention measured at 7 years of age.
Method
Participants
Participants come from a longitudinal study on the social, psychological, and cognitive development of children in Québec, Canada (Santé Québec, Desrosiers, & Tremblay, Reference Santé Québec, Desrosiers and Tremblay1997). One thousand French-speaking and English-speaking families from urban areas and varied socioeconomic backgrounds were randomly selected from the Québec birth registry in 1996–1997, with 572 families participating at the first assessment when the children were 5 months old. The participants were followed annually. From this sample, 293 francophone families from the region of Montreal, Québec, were solicited to participate in laboratory observations when the children were 4 years old. In total, 195 mothers participated in these observations with their child (56.4% girls) and form the sample of the present study. Among mothers who accepted to participate in the laboratory observations, more had girls than among those who declined (B = 0.61, SE = 0.26, p = .02), but there were no differences among those who accepted and declined on other sociodemographic variables (mother education, family income, mother age at first child, or family structure, p = .24 to .43). In the final sample, 9.4% of mothers had not completed high school, 30.7% had a university degree, 20.6% had a family income under 30,000 CAD$ and 5.1% were single parents. Of the participants, 96.9% were Caucasian. Informed parent consent was obtained at the first assessment and renewed at each follow-up. Following attrition, loss to follow-up. and year-to-year variations in participation rates, 175 mothers participated when their children were 5 years old, 134 participated when their children were 6 years old, and 128 participated when their children were 7 years old. The University of Montreal, the Louis-Hippolyte Lafontaine, and the CHU Ste-Justine Research Center ethics committees approved this project.
Procedure
Mothers filled out questionnaires annually from when their children were 5 months to 7 years of age. In the context of the broader longitudinal study, negative parenting (assessed with a coercive parenting scale) was assessed at age 5, temperament was assessed at age 6, and hyperactivity-impulsivity/inattention was assessed at age 7. At age 4, mothers and their children made a visit to the laboratory where they participated in four videotaped activities where mothers’ positive parenting skills in various contexts could be assessed. For each context, an activity that would be enticing for children while also requiring mothers’ help was administered. Furthermore, activities that were expected to be more and less familiar for mothers were chosen in order to represent adequately the different challenges they encounter when helping their children. The order of participation in the various contexts was counterbalanced.
The first context was a joint reading activity. Joint reading activities are often used to observe parent–child interactions (e.g., Barnes & Puccioni, Reference Barnes and Puccioni2017; Bennetts, Mensah, Westrupp, Hackworth, & Reilly, Reference Bennetts, Mensah, Westrupp, Hackworth and Reilly2016; Bergin, Reference Bergin2001; Crain-Thoreson, Dahlin, & Powell, Reference Crain-Thoreson, Dahlin and Powell2001; de Jong & Leseman, Reference de Jong and Leseman2001; Moretti, Shaw, & Fox, Reference Moretti, Shaw and Fox2003). Three storybooks and an alphabet book were presented to the dyad. The mother was invited to choose the storybook that would be most interesting for their child and was asked to read the chosen storybook and the alphabet book to the child like she would do at home. No time constraint or book order were given, and the experimenter stepped out of the room while the mother and child completed the activity.
The second context was a joint story-telling activity where the dyad had to complete stories introduced by the experimenter. The stories were from the MacArthur Story Stem Battery (Bretherton, Oppenheim, Buchsbaum, Emde, & MacArthur Narrative Work Group, Reference Bretherton, Oppenheim, Buchsbaum, Emde, Emde, Wolf and Oppenheim2003; Warren, Emde, & Sroufe, Reference Warren, Emde and Sroufe2000). Four stories were introduced with toys representing a child (from the same sex as the child participating in the study), mother, father, brother or sister, best friend, and a baby, as well as various objects. Each story introduced an emotional theme, and the mother and child were asked to complete the story using the toys (“Show me and tell me what happens next”). Each story was on a different theme, aiming to elicit specific emotions: (a) gift to mom or dad—theme of pride and preference for one parent; (b) fight with a friend—theme of anger management; (c) climbing the rock—theme of pride and cautiousness; and (d) the cookie jar—theme of conflict between loyalty to the parent and loyalty to the sibling. No time constraint was given to complete each story, and the order of the stories was counterbalanced (except for the first one, which was used as a warm-up story).
The third context was a numbered dot-to-dot drawing activity (see Caron, Parent, Normandeau, Tremblay, & Séguin, Reference Caron, Parent, Normandeau, Tremblay and Séguin2008). Three choices of dot-to-dot drawings of equivalent difficulty (20 to 25 numbers dispersed in such a way that the figure cannot be guessed in advance) were presented to the child, who could choose his or her favorite. The child was then instructed to complete the drawing by connecting the numbers in order, starting by 1, and the mother was told to help the child as she deemed necessary. No time constraint was given, and the experimenter stepped out of the room while the mother and child completed the activity. This observational context was used in previous research, and the task presents a good challenge to 4-year-olds (Caron et al., Reference Caron, Parent, Normandeau, Tremblay and Séguin2008).
The fourth and last context was a number-to-image matching activity called Mystero (Lyons & Lyons, Reference Lyons and Lyons1999). This game includes 40 clue cards of increasing difficulty with nine squares. Eight of those squares include a clue for a number between 1 and 9. The ninth square has a question mark and is the “mystery number,” which is the last number remaining when the 8 clues have been paired with their corresponding number. The dyads completed the first 2 clue cards. Mothers were asked to help their child like they would normally do while playing with them. No time constraint was given, and the experimenter stepped out of the room while the mother and child completed the activity. This observational context was also used in previous research, and the task presents a good challenge to 4-year-olds (Caron et al., Reference Caron, Parent, Normandeau, Tremblay and Séguin2008).
Measures
Hyperactivity-impulsivity and inattention
When the children were 7 years old, mothers answered four items on hyperactivity-impulsivity and four items on inattention. These items are from the Social Behavior Questionnaire (Tremblay et al., Reference Tremblay, Loeber, Gagnon, Charlebois, Larivee and Leblanc1991) and were used in several other large-scale longitudinal studies (e.g., Quebec Newborn Twin Study—Boivin et al., Reference Boivin, Brendgen, Dionne, Dubois, Perusse, Robaey and Vitaro2013; Ontario Child Health Study—Boyle et al., Reference Boyle, Offord, Hofmann, Catlin, Byles, Cadman and Szatmari1987; EMIGARDE cohort—Charrois et al., Reference Charrois, Côté, Japel, Séguin, Paquin, Tremblay and Herba2017; Quebec Longitudinal Study of Child Development—Jetté, Desrosiers, Tremblay, & Thibault, Reference Jetté, Desrosiers, Tremblay and Thibault2000; Montreal Longitudinal and Experimental Study—McCord, Tremblay, Vitaro, & Desmarais-Gervais, Reference McCord, Tremblay, Vitaro and Desmarais-Gervais1994; National Longitudinal Survey of Children—Statistics Canada, 1995). They were shown to have good convergent and discriminant validity (Boyle et al., Reference Boyle, Offord, Racine, Sanford, Szatmari and Fleming1993; Leblanc et al., Reference Leblanc, Boivin, Dionne, Brendgen, Vitaro, Tremblay and Pérusse2008), and to be related to several developmental outcomes, including academic achievement (Pingault et al., Reference Pingault, Tremblay, Vitaro, Carbonneau, Genolini, Falissard and Côté2011; Salla et al., Reference Salla, Michel, Pingault, Lacourse, Paquin, Galéra and Côté2016), criminality (Pingault, Côté, Lacourse, et al., Reference Pingault, Côté, Lacourse, Galéra, Vitaro and Tremblay2013), and substance abuse (Pingault, Côté, Galéra, et al., Reference Pingault, Côté, Galéra, Genolini, Falissard, Vitaro and Tremblay2013). All items referred to the past year and were answered on a 3-point scale (1 = never, 2 = sometimes, 3 = often). The scales were modeled using confirmatory factor analysis (see Data Analysis section).
Parenting
Positive parenting was assessed at 4 years from laboratory observations of mother–child interactions in four contexts (see Procedure section). Six scales were rated from these observations: (a) quality of guidance (i.e., the extent to which the mother dynamically adjusts her cognitive guidance to child needs); (b) supportive presence (i.e., the emotional support offered by the mother to her child); (c) effective structure and limit setting (i.e., the mother's ability to structure and appropriately limit the child's behavior during the task); (d) acceptation of the child (i.e., the way the mother responds to her child's reactions or initiatives, the degree to which she accepts these reactions, and the degree to which she accepts her child in general); (e) respect for child's autonomy (i.e., the extent to which the mother acts in a manner that aims to recognize and respect her child's individuality, motivations, and perceptions during the task); and (f) low hostility (i.e., low levels of anger, denigration, or rejection of the child by the mother). These scales are based on Oppenheim, Emde, and Wamboldt (Reference Oppenheim, Emde and Wamboldt1996; scales a and d) and Erickson, Sroufe, and Egeland (Reference Erickson, Sroufe and Egeland1985; all other scales), and are frequently used to assess the quality of parenting behaviors (e.g., Corapci, Benveniste, & Bilge, Reference Corapci, Benveniste and Bilge2018; de Jong & Leseman, Reference de Jong and Leseman2001; Gini, Oppenheim, & Sagi-Schwartz, Reference Gini, Oppenheim and Sagi-Schwartz2007; Lawler, Koss, & Gunnar, Reference Lawler, Koss and Gunnar2017; Lucassen et al., Reference Lucassen, Kok, Bakermans-Kranenburg, van Ijzendoorn, Jaddoe, Hofman and Tiemeier2015; Shlafer, Raby, Lawler, Hesemeyer, & Roisman, Reference Shlafer, Raby, Lawler, Hesemeyer and Roisman2015; Stoltz, Beijers, Smeekens, & Dekovic, Reference Stoltz, Beijers, Smeekens and Dekovic2017). Details regarding ratings for each scale are provided in the online-only Supplementary Materials. Twenty percent of observations were randomly selected to be rated by two coders. Intraclass correlation coefficients (ICCs) were calculated using SPSS Version 24 based on a one-way random effects model. Among the 20 scales across the four contexts, 8 showed excellent reliability (ICC > .90), 10 showed good reliability (.90 > ICC > .75), and 2 showed moderate reliability (.75 > ICC > .65). Preliminary analyses showed that the different scales and contexts interacted similarly with inhibitory control in the prediction of ADHD symptoms. Thus, as done in previous research examining overall positive parenting with similar observation scales (e.g., de Jong & Leseman, Reference de Jong and Leseman2001; Stoltz et al., Reference Stoltz, Beijers, Smeekens and Dekovic2017), standardized scores of the scales across all four contexts were averaged to obtain a general positive parenting index (α = 0.90, 90% CI [0.88, 0.92]).
Negative parenting was assessed at 5 years with a coercive parenting scale composed of questions from the Parent Practices Scale (Strayhorn & Weidman, Reference Strayhorn and Weidman1988) that were used in the first cycle of the National Longitudinal Survey of Children and Youth (Statistics Canada, 1995). Mothers answered seven questions (e.g., “How often do you raise your voice, scold, or yell at him/her?”). Each item was rated on a 5-point scale (1 = never, 5 = many times each day, or all the time). As done in previous research using this scale (e.g., Rioux, Castellanos-Ryan, Parent, Vitaro, et al., Reference Rioux, Castellanos-Ryan, Parent, Vitaro, Tremblay and Séguin2016; Romano, Tremblay, Boulerice, & Swisher, Reference Romano, Tremblay, Boulerice and Swisher2005), the sum of the items was used to form the scale (M = 14.50, SD = 3.18; skewness = 0.37; kurtosis = –0.40; α = 0.71).
Inhibitory control
When the children were 6 years old, mothers completed the Children's Behavior Questionnaire (Rothbart et al., Reference Rothbart, Ahadi, Hershey and Fisher2001), which includes six items on inhibitory control (e.g., “When told that a place is dangerous, he/she goes there slowly and carefully”). Each item was rated on a 7-point scale (1 = extremely inaccurate, 7 = extremely accurate). As done in previous research using this scale (e.g., Gartstein, Putnam, & Kliewer, Reference Gartstein, Putnam and Kliewer2016; Rioux, Castellanos-Ryan, Parent, Vitaro, et al., Reference Rioux, Castellanos-Ryan, Parent, Vitaro, Tremblay and Séguin2016; Szabo, Dubas, & van Aken, Reference Szabo, Dubas and van Aken2012), the sum of the items was used to form the scale (M = 30.26, SD = 5.48; skewness = –0.49; kurtosis = –0.23; α = 0.62, 95% CI [0.51, 0.71]). Because three items (i.e., “has trouble sitting still when told to”; “has difficulty waiting in line for something”; and “can wait before entering new activity if asked to”) were similar in wording to the hyperactivity-impulsivity items (see Figure 1), a scale was computed with the three remaining items (i.e., “is good at following instructions”; “can easily stop an activity when told no”; and “when told that a place is dangerous, approaches it slowly and cautiously”; M = 15.55, SD = 2.73; skewness = –0.39; kurtosis = –0.39) in order to reduce the possibility of confounded results. Significant interactions were similar with both scales. All results presented in the remainder of the paper used the three-item scale. For results with the original scale, see the online-only Supplementary Materials.

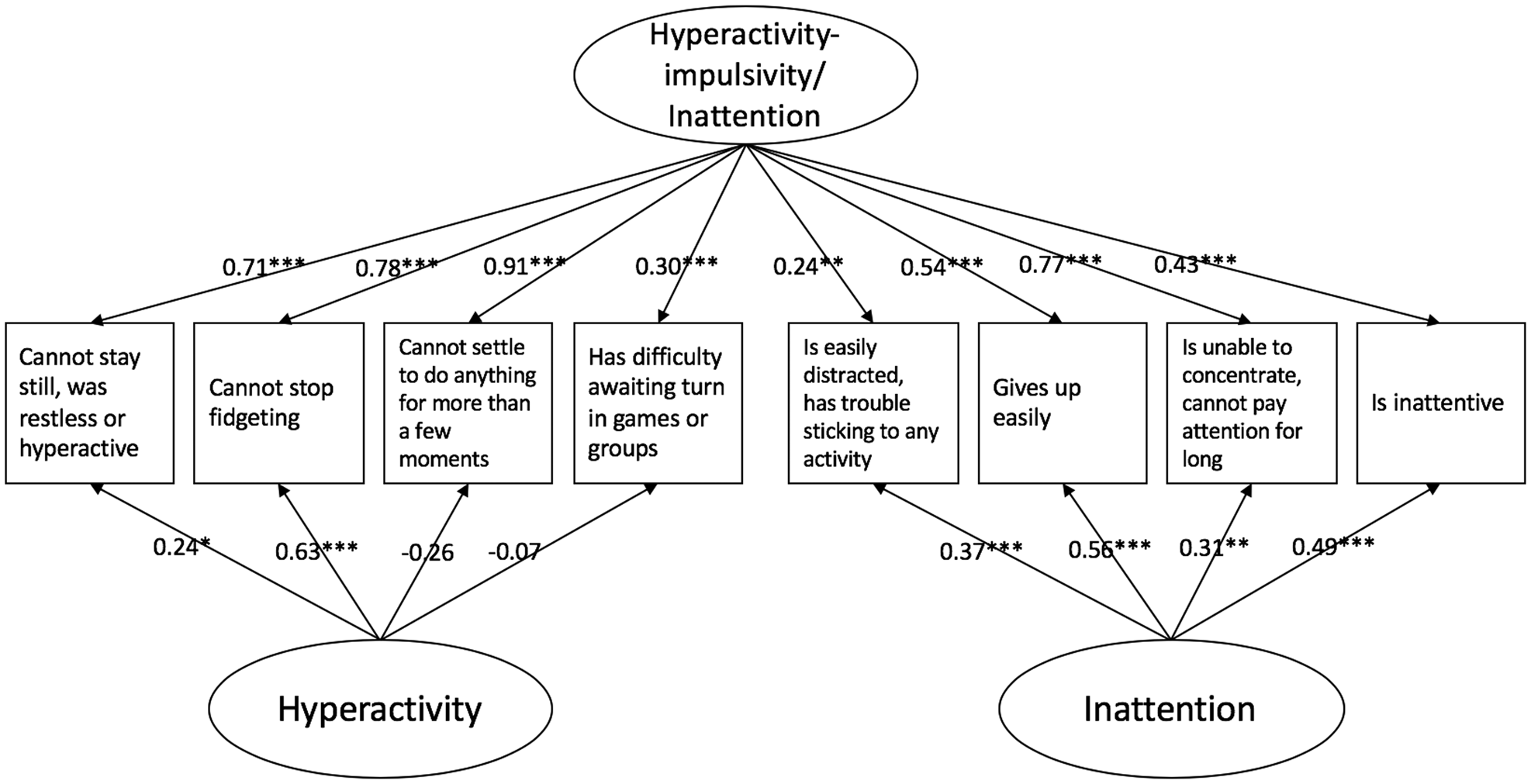
Figure 1. Bifactor model of hyperactivity-impulsivity and inattention. The common hyperactivity-impulsivity/inattention factor captures variance from all the items. The specific inattention factor captures variance from the four inattention items. The specific hyperactivity factor only captures variance from the items specific to hyperactive motor activity. Model fit: χ2 (13) = 8.58; RMSEA = .00 (95% CI [0.00, 0.06]); SRMR = .03; TLI = 1.03; CFI = 1.00. *p < .05. **p < .01. ***p < .001.
Control variables
A measure of socioeconomic status (SES) at 5 months was included as a covariate using the sum of the standardized scores of maternal educational level, family income, and maternal age at the birth of their first child. An index of conduct problems (physical aggression, opposition, and nonaggressive behavioral problems) rated by the mother at 7 years was also included as a covariate. Correlations between all study variables are provided in the online-only Supplementary Materials.
Data analysis
Analyses were conducted using Mplus version 7.0 (Muthén & Muthén, Reference Muthén and Muthén1998–2012). Maximum likelihood with robust standard errors estimation, which is robust to deviations from normality (Kaplan, Kim, & Kim, Reference Kaplan, Kim, Kim, Millsap and Maydeu-Olivares2009), was used. Analyses were conducted with all 195 participants, and full information maximum likelihood was used to account for missing data. Sex, age of the mother at birth, family income, mother education, family structure, and temperament at 5 months were examined as potential predictors of missingness for the variables and assessments of the present study (i.e., potential predictors of the missing-at-random mechanism; Graham, Reference Graham2009) and found to be nonsignificant predictors of missingness (p > .05).
Factor analyses
In order to examine predictors of the common and unique variance of hyperactivity-impulsivity and inattention, a bifactor model was conducted. Prior to using this model, it was compared with alternative models for goodness of fit (i.e., with a one-factor model, a correlated factors model, and a higher order model). Confirmatory factor analyses showed that the bifactor model was the best fit for the data (see the online-only Supplementary Material), as suggested by previous research (e.g., Gibbins et al., Reference Gibbins, Toplak, Flora, Weiss and Tannock2012; Martel et al., Reference Martel, von Eye and Nigg2010; Normand et al., Reference Normand, Flora, Toplak and Tannock2012; Toplak et al., Reference Toplak, Sorge, Flora, Chen, Banaschewski, Buitelaar and Faraone2012; Willoughby et al., Reference Willoughby and Blanton2015). In a bifactor model such as the one retained, all hyperactivity-impulsivity and inattention items load on a single common latent factor, and they also load on specific latent factors that explain variance unique to the respective hyperactivity-impulsivity or inattention items that is not shared with the other set of items (i.e., unique variance that is over and above the common variance shared among all items captured by the common factor). Thus, the common factor represents what is shared among hyperactivity-impulsivity and inattention, while the two specific factors represent what is unique to hyperactivity-impulsivity and inattention beyond what is shared among them. Thus, the bifactor model results in three factors that were examined as outcomes (i.e., a specific hyperactivity-impulsivity factor, a specific inattention factor, and a common hyperactivity/inattention factor). As can be seen in Figure 1, all items loaded significantly and positively on the common hyperactivity-impulsivity/inattention factor, all inattention items loaded significantly on the unique inattention factor, but only two of the four hyperactivity-impulsivity items loaded significantly on the specific hyperactivity-impulsivity factor, indicating that this factors reflected variance unique to the hyperactive motor activity dimension (and not the variance unique to the impulsive dimension). Thus, this factor is referred to as the unique hyperactivity factor (and not the hyperactivity-impulsivity factor).
Moderation analyses
Moderation analyses were then conducted to examine whether the interaction between inhibitory control and parenting predicts hyperactivity, inattention, and/or hyperactivity-impulsivity/inattention. These moderation analyses built on the bifactor model detailed above by entering the predictors to this bifactor model in Mplus. That is, the three estimated latent factors were used as outcomes, and analyses were conducted with one main effects step and one interaction effects step where all three factors (i.e., common hyperactivity-impulsivity/inattention, specific hyperactivity, and specific inattention) were regressed on the predictors in the same model. SES, conduct problems (covariates), positive parenting, coercive parenting, and inhibitory control were first included to test main effects, followed by the interaction terms between inhibitory control and positive parenting and between inhibitory control and coercive parenting. Predictor and moderator variables were standardized before computing interaction terms and entering variables in the analysis. Testing for diathesis-stress, differential susceptibility, and vantage sensitivity requires the predictor and moderator to be independent from each other (Belsky & Pluess, Reference Belsky and Pluess2009). Because there was a small correlation between coercive parenting and inhibitory control (r = –.18, p < .05), coercive parenting was regressed on inhibitory control and the coercive parenting residual score was used in analyses, as is often done in other studies testing these models (Rioux, Castellanos-Ryan, Parent, & Séguin, Reference Rioux, Castellanos-Ryan, Parent and Séguin2016). Positive parenting was not significantly correlated with inhibitory control (r = .14, p > .10). When significant interactions were found, the estimated values of ADHD symptoms as a function of parenting was plotted at lower and higher levels of inhibitory control (+/–1 SD) and followed by simple slope tests to determine the nature of the interaction. Following recommendations for interpreting continuous moderators (Aiken & West, Reference Aiken and West1991; Frazier, Tix, & Barron, Reference Frazier, Tix and Barron2004), simple slopes represent the effect of parenting on ADHD symptoms when the model with the interaction effects was rerun with inhibitory control recoded so its mean would be at +/–1 SD instead of zero. Interactions were probed with inhibitory control at +/–1 SD as this is the most commonly used metric to represent low and high levels on variables without a clinical or otherwise meaningful cut-off (Frazier et al., Reference Frazier, Tix and Barron2004).
To test for diathesis-stress, vantage sensitivity, and differential susceptibility, the nature of significant interactions was further examined using regions of significance analyses and the proportion of interaction (PoI) index (Roisman et al., Reference Roisman, Newman, Fraley, Haltigan, Groh and Haydon2012). The regions of significance were examined using the Johnson–Neyman technique, which identifies at what level in the parenting continuum children who are higher or lower on inhibitory control differ in their levels of hyperactivity-impulsivity/inattention, hyperactivity, and/or inattention. If they differ at both the low and high ends of the parenting variable, results support the differential susceptibility model. If they only differ at the low end of positive parenting or the high end of coercive parenting, results support the diathesis-stress model. If they only differ at the high end of positive parenting or the low end of coercive parenting, results support the vantage sensitivity model. However, because region of significance testing is dependent on sample size, further quantification of the interaction using the PoI index has been proposed (Roisman et al., Reference Roisman, Newman, Fraley, Haltigan, Groh and Haydon2012). The PoI index measures the proportion of the total area of the interaction attributable to the positive environment. A prototypical differential susceptibility model has a PoI of .50, a prototypical diathesis-stress model has a PoI of 0, and a prototypical vantage sensitivity model has a PoI of 1. Proposed criteria are that a PoI = .20–.80 supports differential susceptibility (Del Giudice, Reference Del Giudice2017), with a PoI under .20 supporting diathesis-stress and a PoI over .80 supporting vantage sensitivity.
Results
Bivariate associations between the predictors and the three ADHD factors are presented in Table 1. The common hyperactivity-impulsivity/inattention factor was negatively predicted by SES, positive parenting, and inhibitory control, and positively predicted by conduct problems and coercive parenting. A marginally significant effect (p = .051) showed that the specific inattention factor was negatively predicted by inhibitory control.
Table 1. Bivariate associations between predictors and outcomes

Note: SES, socioeconomic status. †p < .06. *p < .05. **p < .01. ***p < .001.
Results of the moderation analyses are presented in Table 2. When SES, conduct problems, and all main predictors were taken into account, the common hyperactivity-impulsivity/inattention factor was negatively predicted by positive parenting and inhibitory control, and positively predicted by conduct problems. Only one significant interaction was found: an interaction between positive parenting and inhibitory control predicting the common hyperactivity-impulsivity/inattention factor. The effect of positive parenting was not significant when inhibitory control was low, but was significant and negative when inhibitory control was high (see Figure 2). The regions of significance analysis showed that children higher or lower on inhibitory control differed on hyperactivity-impulsivity/inattention only at higher levels of positive parenting, with a higher bound of significance at 0.1 SD. The PoI index was .97. Thus, all indices indicated that this interaction supported the vantage sensitivity model.

Figure 2. Age 4 positive parenting by age 6 inhibitory control interaction predicting the common hyperactivity-impulsivity/inattention factor at age 7. Positive parenting range showed: –2 SD to +2 SD. Sample distribution: low inhibitory control (below −1 SD) 11.9%, mean inhibitory control (between − 1 SD and + 1 SD) 73.9%, high inhibitory control (above +1 SD) 14.2%.
Table 2. Main and interaction effects of parenting and inhibitory control on the unique and common variance of hyperactivity-impulsivity and inattention at 7 years

Note: SES, socioeconomic status. Model fit main effects model: χ2 (38) = 55.04; CFI = .96, TLI = .93, RMSEA = .05 (95% CI [.01, .07]), SRMR = .04. Model fit interaction model: χ2 (48) = 72.70; CFI = .94, TLI = .90, RMSEA = .05 (95% CI [.02, .07]), SRMR = .04. *p < .05. **p < .01. ***p < .001.
Multigroup analyses were conducted to verify whether effects differed according to sex. Results of the chi-square difference tests showed no significant differences between boys and girls, including for the interaction between positive parenting and inhibitory control predicting the common hyperactivity-impulsivity/inattention factor (χ2 = 0.326, df = 1, p = .57).
Discussion
Although inhibitory control and parenting are both associated with ADHD symptoms, examining their interaction is important because it can help identify intervention targets as well as children most likely to benefit from interventions. Accordingly, the present study examined whether the common and/or unique variance of hyperactivity-impulsivity and inattention were predicted by the interaction between parenting practices and child inhibitory control. More precisely, we tested if inhibitory control, a temperament dimension of effortful control measured at 6 years old, moderated the link between parenting practices (positive parenting observed at 4 years old and self-reported coercive parenting measured at 6 years of age) and the common and/or unique variance of hyperactivity-impulsivity and inattention at 7 years old. We also tested whether such interactions supported the diathesis-stress, vantage sensitivity, or differential susceptibility model.
Main effects indicated that higher levels of positive parenting at 4 years were associated with lower levels of hyperactivity-impulsivity/inattention at 7 years. These results are coherent with past cross-sectional and longitudinal studies that show an association between dimensions of positive parenting and lower levels of ADHD symptoms during childhood (Cussen et al., Reference Cussen, Sciberras, Ukoumunne and Efron2012; Ellis & Nigg, Reference Ellis and Nigg2009; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013; Keown, Reference Keown2012; Tung et al., Reference Tung, Brammer, Li and Lee2015; Ullsperger et al., Reference Ullsperger, Nigg and Nikolas2016). These studies found that positive parenting was associated with hyperactivity-impulsivity (Ellis & Nigg, Reference Ellis and Nigg2009; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013; Ullsperger et al., Reference Ullsperger, Nigg and Nikolas2016) and inattention (Ellis & Nigg, Reference Ellis and Nigg2009; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013; Ullsperger et al., Reference Ullsperger, Nigg and Nikolas2016), as well as with a general ADHD symptoms score (Cussen et al., Reference Cussen, Sciberras, Ukoumunne and Efron2012; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013; Keown, Reference Keown2012; Tung et al., Reference Tung, Brammer, Li and Lee2015). Our results extend these previous findings by showing that positive parenting predicted the common hyperactivity-impulsivity/inattention factor, but not the specific hyperactivity and inattention factors, which suggests that the associations found in previous studies may be driven by what is common among hyperactivity-impulsivity and inattention and not what is unique to them. Moreover, inhibitory control negatively predicted the common hyperactivity-impulsivity/inattention factor, but did not predict the specific inattention factor after controlling for the other predictors, and did not predict the specific hyperactivity factor. These findings are inconsistent with previous studies showing that children's low inhibitory control and effortful control are associated with general ADHD symptoms and specific hyperactivity-impulsivity, but not with inattention (Herzhoff et al., Reference Herzhoff, Tackett and Martel2013; Martel et al., Reference Martel, Roberts, Gremillion, von Eye and Nigg2011). This inconsistency might be due to the fact that in our study we used three out of six inhibitory control items because the three remaining ones were very similar to hyperactivity-impulsivity items and would have reduced the independence of the moderator to the dependent variables. We replicated the results of those previous studies when analyses were run using the original inhibitory control scale, which predicted both the common hyperactivity-impulsivity/inattention factor and the specific hyperactivity factor (see online-only Supplementary Materials). This raises the possibility that some of the previous findings regarding specific associations between inhibitory control/effortful control and hyperactivity-impulsivity could be due overlap between measures. Unfortunately, the previous studies cited above did not provide details regarding the overlap between their inhibitory control/effortful control measures and their hyperactivity-impulsivity measure, making it difficult to confirm whether this was the case. These previous studies also used a clinical measure of ADHD, which could also account for the discrepancies in results.
Regarding the main objective, an interaction between positive parenting and inhibitory control was found in the prediction of the common hyperactivity-impulsivity/inattention factor, but no interactions were found in the prediction of the unique hyperactivity and inattention factors. The significant interaction showed that positive parenting at 4 years significantly predicted lower levels of hyperactivity-impulsivity/inattention at 7 years only when child inhibitory control was higher at 6 years. This could be explained by the fact that children high on inhibitory control are better able to direct their attention to stimuli from the environment, which would allow them to process information more easily and deeply, thus exhibiting more sensitivity to their environment (Aron, Aron, & Jagiellowicz, Reference Aron, Aron and Jagiellowicz2012). According to Aron et al. (Reference Aron, Aron and Jagiellowicz2012), inhibiting a behavior can allow children to be more responsive to the environment because they take a pause to observe environmental cues instead of ignoring them. Thus, through the inhibition of predominant responses, children with higher inhibitory control can direct their attention on their parents’ demands, leading them to benefit more from positive parenting practices. These theoretical explanations behind our results are in agreement with the vantage sensitivity model, which posits that certain individuals show an increased sensitivity to positive experiences exclusively (Pluess & Belsky, Reference Pluess and Belsky2013). Children with higher inhibitory control seem to be more sensitive only to positive parenting practices in the prediction of hyperactivity-impulsivity/inattention as all statistical indices supported the vantage sensitivity model and interactions were not detected with coercive parenting practices.
Vantage-sensitivity factors can lead to a reduction in developmental problems and/or enhance positive adjustment (Pluess & Belsky, Reference Pluess and Belsky2013). In the present study, a positive environment was associated with low levels of negative adjustment for children high on inhibitory control. Future studies could examine whether children high on inhibitory control show not only low levels of developmental problems in positive environments but also high levels of positive adjustment. This would allow a better understanding of the role of inhibitory control as a vantage-sensitivity factor. Regarding the development of vantage-sensitivity factors, it has been suggested that this sensitivity only to positive environments would not be innate, but would rather be influenced by the early environment. According to this hypothesis, infants with a genetic predisposition for environmental sensitivity may be sensitive to both positive and negative environments, but their sensitivity would become more pronounced toward positive environments when they grow up in a positive environment (Pluess, Reference Pluess2015). This suggests that high inhibitory control in middle childhood may already be a reflection of the interaction between genetic sensitivity and the child's early environment. Furthermore, it also suggests that earlier temperament may interact differently with the environment in the prediction of ADHD symptoms. Both propositions should be examined in future studies, which would help refine our current understanding of the development of environmental sensitivity and their relation to ADHD symptoms.
The interaction identified in the present study also suggests that there could be two different pathways regarding the development of hyperactivity-impulsivity/inattention (i.e., one pathway through lower inhibitory control and one pathway through lower positive parenting). A lower inhibitory control was associated with higher levels of hyperactivity-impulsivity/inattention regardless of levels of parenting behaviors. Still, a higher inhibitory control was also associated with high levels of hyperactivity-impulsivity/inattention, but only when positive parenting practices were low. Furthermore, analyses showed that when positive parenting practices were low, levels of hyperactivity-impulsivity/inattention did not differ, and thus were equally high for children low and high on inhibitory control. Inhibitory deficits have traditionally been the focus of causal models of ADHD (e.g., Nigg et al., Reference Nigg, Goldsmith and Sachek2004; Sonuga-Barke, Reference Sonuga-Barke2005), and environmental factors are often only considered for their potential to influence symptoms in children who are at risk for the disorder because of their personal characteristics (Campbell, Halperin, & Sonuga-Barke, Reference Campbell, Halperin, Sonuga-Barke, Lewis and Rudolph2014). Thus, results of the present study highlight the possibility that there would be a pathway rarely considered in the prediction of ADHD symptoms, which is through less optimal parenting, but for children not presenting the personal characteristics associated with risk for ADHD. This pathway should be examined in future research to help determine whether it should be integrated into the current etiological models of ADHD.
Clinical implications
A better understanding of the etiology of inattention and hyperactivity-impulsivity can help develop targeted interventions in order to reduce the risk of developing ADHD symptoms. If replicated in future research, including clinical research, the developmental pathways outlined above could help adapt prevention and intervention efforts according to children's characteristics. Interventions targeting parenting practices would be prioritized for children with higher inhibitory control while interventions aimed at improving children's inhibitory control would be favored for those with lower inhibitory control. Regarding parenting interventions, a meta-analytic review explored which program components were associated with better outcomes in parent training programs for prevention and/or reduction of early childhood behaviors problems (Kaminski, Valle, Filene, & Boyle, Reference Kaminski, Valle, Filene and Boyle2008). Larger effects were reported for programs using strategies to increase positive parent–child interactions, emotional communication, and parenting consistency, which are aspects that are associated with positive parenting as measured in the present study. Regarding inhibitory control, previous research showed that physical activity interventions were promising in increasing inhibitory control through executive function. Interventions that involved exercise with both aerobic and motor skills components showed beneficial effects on response inhibition in children with ADHD (Chang, Hung, Huang, Hatfield, & Hung, Reference Chang, Hung, Huang, Hatfield and Hung2014; Pan et al., Reference Pan, Tsai, Chu, Sung, Huang and Ma2019; Ziereis & Jansen, Reference Ziereis and Jansen2015). Thus, it seems that physical activity may be an important component in interventions for children with low inhibitory control. Moreover, considering our findings, improving children's inhibitory control may in turn help them become more sensitive to the protective effects of positive parenting practices.
Strengths and limitations
The interaction between effortful control and parenting practices in the prediction of child adjustment outcomes such as externalizing problems has been tested in a few studies (Slagt et al., Reference Slagt, Dubas, Dekovic and van Aken2016). Although these studies examined effortful control globally, its subdimensions can be associated differently with developmental outcomes (De Pauw & Mervielde, Reference De Pauw and Mervielde2010). This suggests that it is important to study its subdimensions, such as inhibitory control, which was the focus of the present study. Furthermore, to our knowledge, no study has examined the interaction between dimensions of effortful control and parenting in the prediction of hyperactivity-impulsivity and inattention specifically. Hence, the present study is the first to do so, in addition to testing whether this interaction supports the diathesis-stress, vantage sensitivity, or differential susceptibility model. Another strength of this study is the stringent testing of these models. In addition to following recommended statistical criteria for the models, both positive and negative environmental influences were examined. Furthermore, positive parenting practices were measured using structured observations in several contexts, which allowed for an objective and exhaustive evaluation.
However, some limitations should be noted. The sample is urban, francophone, and mostly Caucasian, which limits the generalization of results. Thus, more studies are needed to determine whether these findings apply to other populations. Coercive parenting was measured through self-report, which is susceptible to bias, notably social desirability. Nonetheless, self-reports are often used and considered reliable in assessing negative parenting practices, especially considering that they focus on behaviors that are difficult to observe (Gardner, Reference Gardner2000). Furthermore, the current study examined parenting practices of mothers only, and the effect might be different with fathers. Thus, it would be important to conduct research with fathers’ parenting practices or both parents’ practices to verify whether the results are invariant or differ across parents. In addition to parenting, mothers also reported on ADHD symptoms and temperament, raising the possibility that shared method variance may account for a portion of the associations. As the present study focused on inhibitory control, future studies are also needed to determine whether results differ for effortful control globally, and/or for other dimensions of effortful control. Further, the present study used nonclinical measures of hyperactivity-impulsivity and inattention. Thus, studies are needed to examine how these results apply to clinical ADHD symptoms and diagnosis. A few studies showed a bidirectional relationship between parenting practices and ADHD symptoms (Breaux & Harvey, Reference Breaux and Harvey2018), which was not tested in the present study. Consequently, it would also be important for future studies to examine how bidirectional effects between parenting and ADHD are moderated by children's characteristics such as inhibitory control. Finally, this study is prospective and correlational, and therefore describes a possible developmental sequence but does not show causal relationships between parenting, inhibitory control, hyperactivity-impulsivity, and inattention. Studies looking at longitudinal associations with repeated measurements of ADHD would strengthen conclusions regarding the developmental sequence. Furthermore, randomized intervention studies testing the vantage sensitivity model could clarify the causal chain. Randomized controlled trials have already shown support for vantage sensitivity when looking at moderation of parenting intervention effects by genes in the prediction of externalizing behaviors (see Bakermans-Kranenburg & van IJzendoorn, Reference Bakermans-Kranenburg and van IJzendoorn2015; de Villiers, Lionetti, & Pluess, Reference de Villiers, Lionetti and Pluess2018, for reviews), and when looking at moderation of parenting intervention effects by temperament in the prediction of attachment security (Cassidy, Woodhouse, Sherman, Stupica, & Lejuez, Reference Cassidy, Woodhouse, Sherman, Stupica and Lejuez2011) and oppositional behaviors (Scott & O'Connor, Reference Scott and O'Connor2012). Similar experimental studies could be conducted to increase confidence in the causality of the effects found in the present study by looking at the moderation of parenting interventions by inhibitory control in the prediction of ADHD symptoms.
Some limitations and characteristics of the present study may also explain why interactions were found for positive parenting, but not negative parenting. While the measure of positive parenting was general, a more specific coercive parenting scale was used as a proxy for negative parenting. Beyond coercive parenting, other facets of negative parenting, such as overreactive parenting, inconsistent discipline, and intrusiveness, have been shown to be associated with ADHD symptoms (Breaux & Harvey, Reference Breaux and Harvey2018; Demmer et al., Reference Demmer, Puccio, Stokes, McGillivray and Hooley2018; Hawes et al., Reference Hawes, Dadds, Frost and Russell2013; Keown, Reference Keown2012; Tung et al., Reference Tung, Brammer, Li and Lee2015) and could be moderated by inhibitory control. Positive and coercive parenting were also measured using different methods and at different ages. Thus, there is the possibility that the different results for positive and coercive parenting would be confounded by the measurement method and/or developmental effects. Future studies comparing positive and negative parenting practices with more similar measurement approaches and at the same age would strengthen conclusions regarding these interactions. Furthermore, the sample is normative, and effects may be different for higher risk samples. However, coercive parenting remains a risk factor in this sample because it was shown to be associated with substance use (Rioux, Castellanos-Ryan, Parent, Vitaro, et al., Reference Rioux, Castellanos-Ryan, Parent, Vitaro, Tremblay and Séguin2016).
Conclusion
The present study found that positive parenting and inhibitory control interact in the prediction of the common variance of hyperactivity-impulsivity and inattention. Children with low inhibitory control exhibited higher levels of hyperactivity-impulsivity/inattention regardless of parenting practices. Children with high inhibitory control had similar levels of hyperactivity-impulsivity/inattention as those with low inhibitory control when exposed to lower levels of positive parenting, but had lower levels of hyperactivity-impulsivity/inattention when exposed to higher levels of positive parenting. This interaction supported the vantage sensitivity model, which posits that some individuals show an increased sensitivity to positive experiences exclusively. The findings of this study suggest that a targeted prevention approach could be particularly efficient to reduce the risk of developing ADHD symptoms. Inhibitory control would be the intervention target when it is low, but when it is high, parenting would be the intervention target. This highlights that it is essential to consider how risk factors work together in order to have the best outcomes from prevention programs.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0954579419000774.
Acknowledgments
The authors are grateful to Charles-Édouard Giguère, Amélie Rivest, and Maria Rosa for data management, and to their partner, the Institut de la Statistique du Québec. The authors thank all the parents and children for their generous participation in the study.
Financial Support
This study was funded by the Fonds de Recherche du Québec–Santé through a scholarship (to C.R.), a fellowship (to C.R.), a research career award (to N.C.R.), and Grants 991027 and 981055; the Fonds de Recherche du Québec–Société et Culture through Grant 2002-RS-79238; the Canadian Institute of Health Research through a fellowship (to C.R.) and Grant 44072; the Social Sciences and Humanities Research Council of Canada through Grants 412-2000-1003 and 839-2000-1008; Valorisation Recherche Québec through Grant 2200-026; the National Science Foundation through Grant SBR 9513040; and the Canadian Language & Literacy Research Network through Grant 27040500.