



Introduction
Results from randomized clinical trials (RCTs) are the most important instrument we have in research to compare treatment options and are therefore fundamental for the development of guidelines for clinical practice—unfortunately, their limitations (inclusion and exclusion criteria) regarding enrollment and regarding “gold standard” questionnaires may impede the clinical meaningfulness of their results.Reference McGoey 1
A first limitation indeed is the discrepancy between efficacy and effectiveness. Efficacy has been defined as “does a treatment more good than harm when delivered under optimum conditions?” (in narrowly defined target populations used in RCTs); effectiveness has been defined as “does a treatment more good than harm when delivered under real-world conditions?” (in routine clinical practice populations).Reference Greenwald and Cullen 2 , Reference Flay 3 Indeed, it has been shown that due to well-defined inclusion and exclusion criteria in RCTs, only between 8% and 22% of patients in a clinical outpatient setting can be enrolled in trials which limits the generalizability of RCT results. 4-6
And a second limitation is that the most often used depression-specific scales to assess changes during treatment (the observer-rated Hamilton Depression Rating Scale [HAMD] and the Montgomery–Åsberg Depression Rating Scale [MADRS]) only focus on symptoms and not necessarily reflect what matters to patients.Reference Hamilton 7 , Reference Montgomery and Åsberg 8
Indeed, at least two studies show discrepancies between what is comprised in standard questionnaires and what patients expect.Reference Zimmerman, McGlinchey, Posternak, Friedman, Attiullah and Boerescu 9 , Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 10 Patients mainly expect the return of positive mood and of normal functioning: the top five patient expectations were reported to be return of positive mental health (optimism, vigor, and self-confidence); feeling like your usual self; return to usual level of functioning at work, home, or school; feeling in emotional control; and participating in and enjoying relationships with family and friends.Reference Zimmerman, McGlinchey, Posternak, Friedman, Attiullah and Boerescu 9 On the same lines, another study also found that “my life is meaningful” and return of positive affect were the highest ranked patient expectations.Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 10 The latter study showed the important discrepancy between physician and patient expectations in depression treatment and found that this discrepancy negatively influences treatment outcome 6 months later.Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 10
In an attempt to go beyond symptoms and beyond disease-specific measures, the Clinical Global Impression of Improvement (CGI-I) was developed and assesses the clinician’s overall view of patients’ symptoms and functioning.Reference Guy 11 But a study looking at what drives the physician’s score on the CGI-I again showed the strong physician-centered approach: symptoms assessed through interviewing the patient, observer-rating scales, functioning assessed through interviewing, and observed behavior were stronger predictors of CGI-I scores than what patients report on symptoms through self-report scales, or on side effects again reflecting a physician-centered approach.Reference Dunlop, Gray and Rapaport 12 The Patient Global Impression of Improvement (PGI-I) is the self-rated version and hence should better reflect the patient’s view. Unfortunately, correlations between CGI-I and PGI-I have been reported to be low in some studies and high in other studies.Reference Demyttenaere, Desaiah, Petit, Croenlein and Brecht 13 , Reference Mohebbia, Dodd, Dean and Berk 14 In the latter study, correlations between CGI-I and PGI-I varied between 0.67 and 0.82; the correlation between CGI-I and decrease in MADRS score varied between 0.49 and 0.76, while the correlation between PGI-I and decrease in MADRS varied between 0.51 and 0.60.Reference Mohebbia, Dodd, Dean and Berk 14
It should be remembered that Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for major depressive disorder (MDD) do not explicitly refer to lack of positive affect but do refer to anhedonia as a core symptom of depression. But despite the DSM criteria and patient expectations, depression scales (HAMD and MADRS) hardly comprise items on hedonic tone.Reference Hamilton 7 , Reference Montgomery and Åsberg 8 Therefore, the Leuven Affect and Pleasure Scale (LAPS) was developed as a self-rating scale with the aim of better representing patient expectations and with the aim to go beyond symptoms: the 16-item scale comprises three subscales (negative affect, positive affect, and hedonic tone) and four independent items (cognitive functioning, overall functioning, my life is meaningful, and I feel happy).Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 15
Therefore, the present study investigated outcome in patients with MDD after 8 weeks of treatment as assessed with the generic outcome measures CGI-I and PGI-I. The main aim was whether LAPS negative affect, LAPS positive affect, and LAPS hedonic tone have added value (on top of HAMD scores) in predicting the generic outcome measures (CGI-I and PGI-I) and in predicting changes in cognitive functioning, overall functioning, “my life is meaningful,” and “I feel happy.” An additional aim was to investigate whether the LAPS subscales differentiate better between different levels of improvement (CGI-I and PGI-I) than (standard) comparator scales representing depressed mood, negative affect, positive affect, negative affect, hedonic tone, and functioning.
Materials and Methods
Subjects
A total of 109 depressed outpatients were enrolled in the study (Belgium, N = 38; France, N = 10; Ireland, N = 10; and Italy, N = 51). Patients were included when they fulfilled DSM-5 criteria for a major depressive episode, and where a treatment with an antidepressant was indicated and started: patients had to be aged between 18 and 70 years and gave an informed consent. Exclusion criteria were meeting criteria for psychotic depression, bipolar disorder, alcohol or substance abuse, or clinical suspicion of dementia. The choice of the treatment was left to the discretion of the treating psychiatrist: pharmacotherapy as usual and combination with psychological treatment were allowed (resulting in a wide range of prescribed antidepressants sometimes combined with benzodiazepines or antipsychotics). Study duration was 8 weeks with visits and assessments at baseline and after 2, 4, and 8 weeks. At endpoint, 21 patients had dropped leaving 88 patients with data at all visits. Average age was 44.7 ± 13.1 years, 64% of included patients were female, 59% were married or living together, and 23% were on sick leave.
The protocol was approved by the French “Comité consultative sur le traitement de l’information en matière de recherché dans le domaine de la santé” (CCTIRS; No. 15-885, 05/19/2016), the “Ethisch Comité UPC KU Leuven” (EC 2016-290, 3/1/2016), and the “Commissie Medische Ethiek UZ-KU Leuven” (S58943, 3/16/2016). The Belgian Registration Number is B322201628071.
Instruments
In the depressed patient group, the following instruments were administered at each visit (at baseline, and at visit 2 after 2 weeks, visit 3 after 4 weeks, and visit 4 after 8 weeks of treatment): the CGI-I and PGI-I (only from visit 2 onward) both having scores between 1 (very much improved) and 7 (very much worsened), the HAMD 17-item version, and the LAPS.Reference Hamilton 7 , Reference Guy 11 , Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 15 The standard definition of HAMD response was used: a 50% decrease from baseline. The standard definitions of CGI-I response and PGI-I response were used: a score of 1 or 2 (ie, very much improved or much improved). The 16-item LAPS has a subscore for negative affect (sum of scores on items 1-4 divided by 4), positive affect (sum of scores on items 5-8 divided by 4), hedonic tone (sum of scores on items 9-12 divided by 4), and a score for “cognitive functioning,” “overall functioning,” “my life is meaningful,” and “I feel happy” (scores between 0 and 10).Reference Demyttenaere, Mortier, Kiekens and Bruffaerts 15 All subscores get the same weight. As comparator scales for LAPS negative affect, LAPS positive affect, LAPS hedonic tone, and LAPS functioning, the Positive and Negative Affect Scale (PANAS), the Snaith–Hamilton Pleasure Scale (SHAPS), and the Sheehan Disability Scale (SDS) were also administered at each visit. 16-18 The scoring of the SHAPS was (in contrast to the original paper) reversed so that higher scores refer to higher pleasure scores (higher “hedonic tone”), which makes the interpretation in comparison with the LAPS hedonic tone easier. For the other scores where a higher score was a clinically worse score (the LAPS negative affect, the PANAS negative affect, and the SDS), response was also defined as a 50% decrease from baseline. This 50% was chosen to have analogy in the definitions.
Statistics
Descriptive statistics are provided using proportions and means (±standard deviations). Change scores for constructs of interest were calculated for each patient from baseline to the end of treatment (xi = end of treatment i – baseline i). Partial correlations were used to examine the associations between change scores of LAPS and CGI-I and PGI-I controlling the change score of HAMD. To further investigate the incremental predictive utility of the LAPS (negative affect, positive affect, and hedonic tone), we performed a series of stepwise regressions that included the change score of HAMD in step 1 and allowed the LAPS variables to be included (if P < .08) and excluded (if P > .10) in the following steps. This allows us to investigate whether the change in the LAPS constructs explained any significant variance in the change score of the generic outcome measures (CGI-I and PGI-I) and in predicting changes in cognitive functioning, overall functioning, “my life is meaningful,” and “I feel happy.” Response on the CGI-I and PGI-I was defined as a score of 1 or 2 and evaluated using logistic regression. Change scores were used for the LAPS independent items and examined using linear regression. Analysis of variance was performed in order to investigate how the LAPS scores for negative affect, positive affect, hedonic tone, and overall functioning (across all time points) differentiate the different levels of CGI-I and PGI-I compared to the included comparator scales. Since the focus of the study was the relation between the questionnaires, we always performed a completer analysis.
Results
After 8 weeks of treatment, 86% of the patients were HAMD responders, but only 57% were CGI-I or PGI-I responders (Table 1). Response rates were 50% for LAPS negative affect, 28% for PANAS negative affect, and 47%, 48%, and 44% for SDS occupational, social, and family functional impairment, respectively. Response rates for LAPS hedonic tone and SHAPS were 58.9% and 61.2%, respectively.
Table 1. HAMD Response (50% Improvement) and CGI-I or PGI-I Response (Much or Very Much Improved) Rates

Abbreviations: CGI-I, Clinical Global Impression of Improvement; HAMD, Hamilton Depression Rating Scale; PGI-I, Patient Global Impression of Improvement.
The partial correlations (controlling for changes in HAMD score) between the change in LAPS subscores and in LAPS independent single items on one hand and CGI-I and PGI-I on the other hand are listed in Table 2 and clearly show much higher correlations between the LAPS items and the self-rated PGI-I than with the observer-rated CGI-I.
Table 2. Partial Correlations (Controlling for Changes in HAMD Between Baseline and Endpoint) Between Changes in LAPS Subscores (Between Baseline and Endpoint) and CGI-I and PGI-I at Endpoint
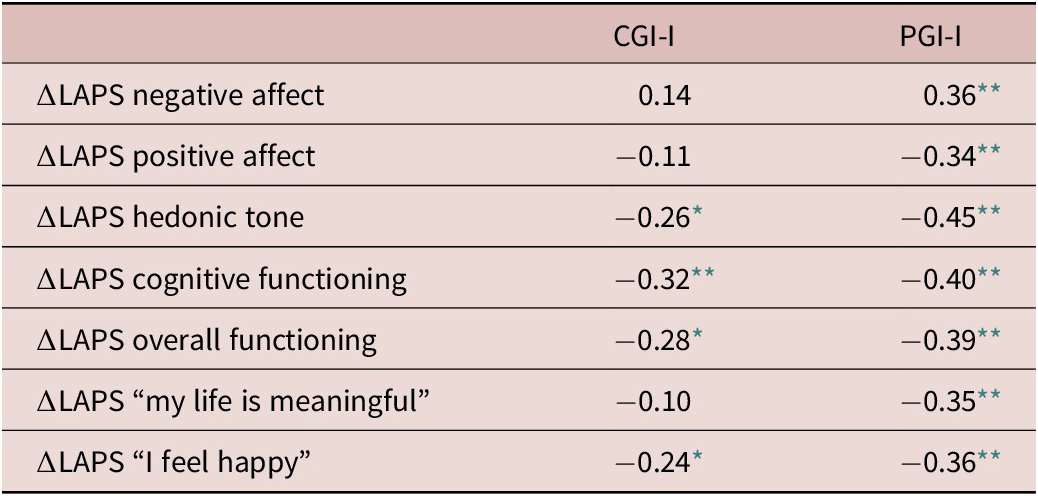
Abbreviations: CGI-I, Clinical Global Impression of Improvement; HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; PGI-I, Patient Global Impression of Improvement.
* P ˂ .05.
** P ˂ .01.
Several regression analyses with a fixed first step (HAMD score) followed by stepwise inclusion and exclusion were performed with the generic outcome measures CGI-I and PGI-I as dependent variables and with the HAMD, LAPS negative affect, LAPS positive affect, and LAPS hedonic tone as independent variables and showed that the LAPS independent scores significantly improved the prediction of the dependent variables. Hence, they clearly show added value on top of the HAMD scores (Table 3). Indeed, 33% of the variance in CGI-I was explained by the change in HAMD, and this increased to 48% when adding the change in LAPS hedonic tone in the prediction model. On the same lines, the 28% of the variance in PGI-I was explained by the change in HAMD, and this increased to 49% when adding the change in LAPS negative affect and LAPS positive affect in the prediction model.
Table 3. Regression Analysis (With Stepwise Elimination) With CGI-I, PGI-I, LAPS functioning, LAPS cognitive functioning, LAPS “My Life Is Meaningful,” and LAPS “I Feel Happy” as Dependent Variables and HAMD, LAPS Negative Affect, LAPS Positive Affect, and LAPS Hedonic Tone as Independent Variables

Abbreviations: CGI-I, Clinical Global Impression of Improvement; HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; PGI-I, Patient Global Impression of Improvement; SE, standard error.
* P ˂ .05.
** P ˂ .01.
*** P ˂ .001.
The same results were obtained when the regression analyses were run with the LAPS single-item variables (cognitive functioning, overall functioning, “my life is meaningful,” and “I feel happy”) as dependent variables. Only 12% of the variance in change in cognitive functioning was explained by the change in HAMD, and this increased to 48% when adding the change in LAPS negative affect and LAPS hedonic tone in the prediction model. And only 18% of the variance in change in overall functioning was explained by the change in HAMD, and this increased to 50% when adding the change in LAPS negative affect and LAPS hedonic tone in the prediction model. Only 21% of the variance in change in LAPS “my life is meaningful” was explained by the change in HAMD, and this increased to 51% when adding the change in LAPS positive affect and the LAPS hedonic tone in the prediction model. Finally, only 16% of the variance in change in LAPS “I feel happy” was explained by the change in HAMD, and this increased to 56% when adding the change in LAPS positive affect in the prediction model.
Analysis of variance was performed in order to investigate how the LAPS scores for negative affect, positive affect, hedonic tone, and overall functioning differentiate the different levels of CGI-I and PGI-I compared to comparator scales (PANAS negative affect compared to LAPS negative affect, PANAS positive affect compared to LAPS positive affect, SHAPS hedonic tone compared to LAPS hedonic tone, and SDS compared to LAPS overall functioning) (Table 4). Compared to the standard comparator scales, the LAPS subscales consistently show numerically higher F values for the different levels of CGI-I; this finding suggests that, in comparison with standard scales, the LAPS subscales better differentiate between the different levels of improvement as assessed with the observer-rated CGI-I. The same trend is seen for the different levels of PGI-I (except for LAPS overall functioning); this finding again suggests that, in comparison with comparator scales, the LAPS subscales better differentiate between the different levels of improvement as assessed with the self-rated PGI-I.
Table 4. F Values Assessing Differences in LAPS Subscale Scores and in Comparator Scale Scores for Clinician-Rated (CGI-I) and Patient-Rated (PGI-I) Levels of Improvement

Abbreviations: CGI-I, Clinical Global Impression of Improvement; HAMD, Hamilton Depression Rating Scale; LAPS, Leuven Affect and Pleasure Scale; PANAS, Positive and Negative Affect Scale; PGI-I, Patient Global Impression of Improvement; SDS, Sheehan Disability Scale; SHAPS, Snaith–Hamilton Pleasure Scale.
Discussion
Response rates were higher for the HAMD than for the other scales (CGI-I, PGI-I, LAPS negative affect, PANAS negative affect, and SDS). This raises the question to what degree the HAMD or the MADRS scale overestimates the “clinical improvement” by focusing on items that are most sensitive to change. Indeed, the HAMD was developed in times where tricyclic antidepressants were the main psychopharmacological treatment for MDD and closely reflects the effects of tricyclics (by including multiple anxiety and sleep items). The MADRS took this even one step further and was presented as “a new depression rating scale designed to be sensitive to change.”Reference Montgomery and Åsberg 8 While sensitivity to change (do the scores change when the clinical status change) is of course an important psychometric characteristic, it becomes somewhat dangerous if we limit our outcome measure to those symptoms where our antidepressants are efficacious since these symptoms are not necessarily the most important ones. It should indeed be remembered that the 10 items of the MADRS were the 10 items of the larger Comprehensive Psychiatric Rating Scale that changed most after treatment with a range of antidepressants.Reference Montgomery and Åsberg 8 And as discussed above, these items are not necessarily the ones that get the highest ranking in patient expectations as shown in two published studies.Reference Zimmerman, McGlinchey, Posternak, Friedman, Attiullah and Boerescu 9 , Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 10
Looking beyond the HAMD, the results show that the partial correlations (controlling for HAMD) between the LAPS variables and the PGI-I are always higher than the correlations with the CGI-I. This could be explained by the fact that the CGI-I is observer-rated, while the PGI-I is self-rated just like the LAPS or by the fact that physicians, in their overall appraisal of change, attach more importance to standard symptoms (as comprised in the standard scales) than to the broader expectations of patients. This has been documented previously, and a naturalistic study already showed that the discrepancy in expectation between physician and patient at baseline significantly negatively influences outcome 6 months later probably explained by the hypothesis that a good concordance between physician and patient influences that part of the improvement that usually is called placebo effect (or a specific effect).Reference Demyttenaere, Donneau, Albert, Ansseau, Constant and van Heeringen 19
Regression analysis showed that the LAPS subscales (LAPS negative affect, LAPS negative affect, and LAPS hedonic tone) significantly increase the percentage of variance in more global outcome measures on top of the percentage explained by the HAMD, suggesting the LAPS is going further than just the standard scale and the LAPS is more patient-centered. This is important since “shared decision making” is getting more and more attention, and outcome measures should better reflect patient expectations. It is remarkable that the added value of the LAPS (on top of the HAMD) is even more pronounced on cognitive functioning (+.36 in adjusted R 2), overall functioning (+.32 in adjusted R 2), “my life is meaningful” (+.30 in adjusted R 2), and “I feel happy” (+.40 in adjusted R 2) than on the CGI-I (+.15 in adjusted R 2) and the PGI-I (+.21 in adjusted R 2) although for all analyses, the added value was statistically significant. A limitation in the interpretation here is that all dependent variables, apart from the CGI-I, were self-rated and the independent variables were also self-rated.
The analysis of variance performed in order to have an estimate of the differentiating power of the LAPS (LAPS negative affect, LAPS positive affect, and LAPS hedonic tone) and of other scales supposed to cover more or less comparable concepts (PANAS negative affect, PANAS positive affect, and SHAPS) showed that the LAPS subscales tend to differentiate better between the different levels of improvement (as assessed with the different scores on the CGI-I or the PGI-I). This again suggests that the LAPS is more sensitive to change than the corresponding standard scales.
A study limitation is the number of patients included in the study: although 88 patients<**> allow the analyses that were performed, they do not allow comparisons between the included countries. In conclusion, treatment with antidepressants shows higher response rates for the HAMD than for more generic measures (CGI-I and PGI-I) or than for more specific scales (LAPS negative affect, PANAS negative affect, and SDS). The partial correlation (controlling for HAMD) between improvement in the self-rated LAPS subscales and the self-rated PGI-I is higher than between the LAPS subscales and the observer-rated CGI-I. The LAPS has added value (on top of the HAMD) in explaining the variance in the changes of more generic outcome measures (CGI-I and PGI-I) as well as of more patient-centered dimensions (cognitive functioning, overall functioning, my life is meaningful, and I feel happy). Finally, the LAPS negative affect as well as the LAPS positive affect and the LAPS hedonic tone differentiate better the scores on the CGI-I and PGI-I than corresponding scales supposed to cover the same domains. Since shared decision making asks among others for concordance between physician and patient expectations and since some studies suggest that meaningfulness of life and return to positive mental health are very important for patients, the LAPS could become a clinically useful tool on top of what the HAMD assesses.
Disclosures
Glenn Kiekens, Philippe Mortier, and Ronny Bruffaerts have nothing to disclose. Koen Demyttenaere has the following disclosures: LivaNova: personal fees, consultant, and speaker’s bureau; Servier: personal fees, consultant, advisory board, and speaker’s bureau; Johnson & Johnson: advisory board. Lorcan Martin received honoraria from Servier in relation to this study. Philip Gorwood received during the last 5 years fees for presentations at congresses or participation in scientific boards from Alcediag-Alcen, Angelini, GSK, Janssen, Lundbeck, Otsuka, SAGE, and Servier. Massimo Di Giannantonio received fees as a consultant/advisor from Servier, Lundbeck, and Otsuka.




