Background
Pulmonary artery slings and vascular rings are very rare congenital anomalies that are associated with significant morbidity and usually present with respiratory distress/dysphagia or both. The presence of both lesions in the same setting is extremely rare and, to our knowledge, has been reported in only one case in literature.Reference Lee, Printz, Hegde, Vargas and Sun 1 We present a case of a toddler who was diagnosed with a left pulmonary artery sling and a vascular ring as part of the screening process for the VACTERL association – co-occurrence of vertebral, anorectal, cardiac, tracheoesophageal, renal, and limb malformations.
Case report
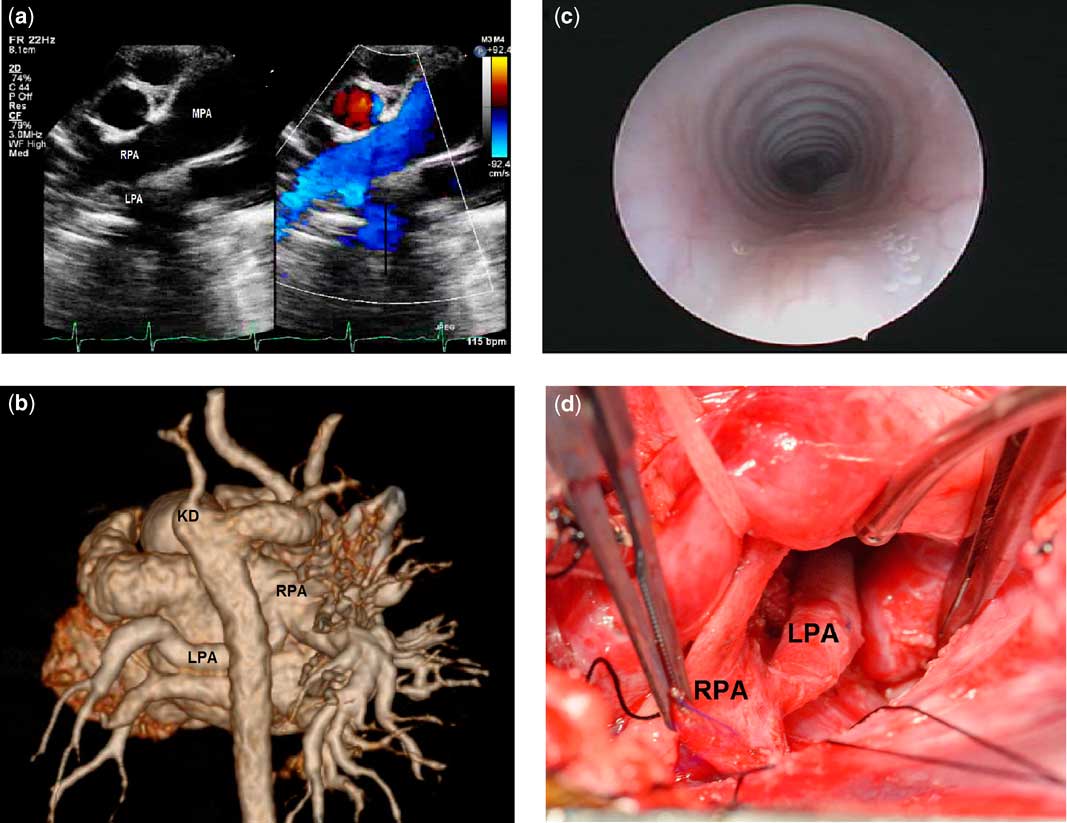
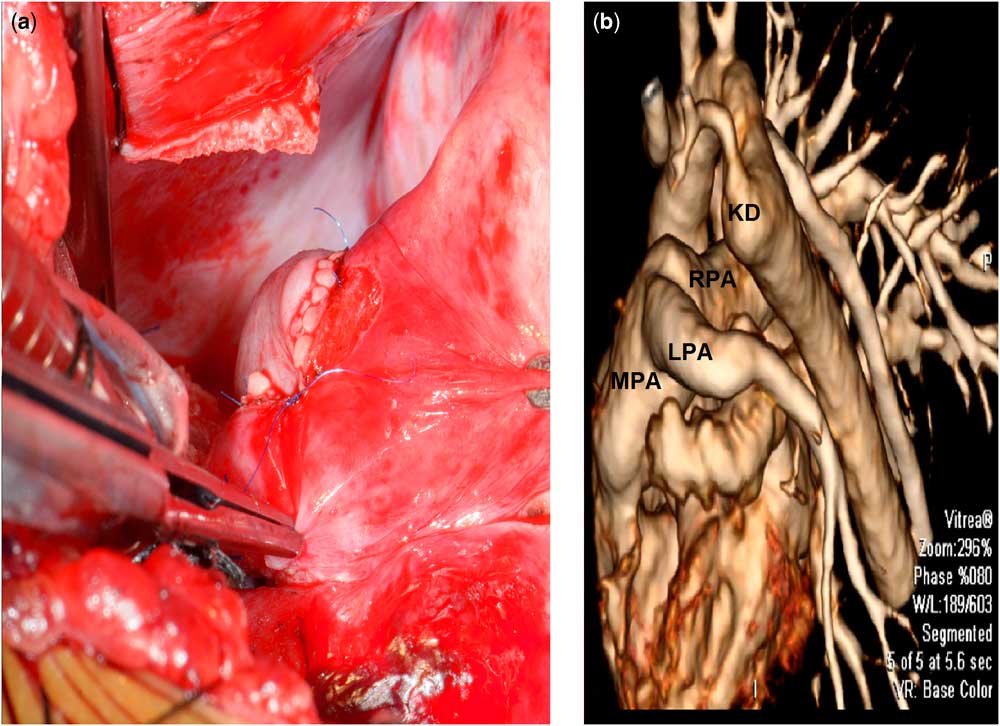
A 21-month-old boy was born at 36 weeks and diagnosed with VACTERL association – vertebral, anorectal, cardiac, tracheoesophageal, genitourinary, and limb malformations – in the form of tethered cord, vertebral anomalies, imperforated anus, and absent left radius and thumb. The chest X-ray showed significant left lung hypoplasia with almost complete mediastinal displacement into the left. An echocardiogram was performed and showed right aortic arch with aberrant left subclavian artery and left pulmonary artery sling (Fig 1a). A flexible bronchoscopy was performed and showed mild (10–20%) impingement of the mid-trachea with no evidence of malacia. A CT angiogram confirmed the presence of a right aortic arch with an aberrant left subclavian artery and a prominent diverticulum of Kommerell. It also showed a left pulmonary artery sling with a diffusely hypoplastic left pulmonary artery originating from the proximal right pulmonary artery, travelling downwards very low in the chest, and associated with left lung hypoplasia (Fig 1b). The trachea showed evidence of complete tracheal rings without significant narrowing. The child was mainly asymptomatic with no feeding issues except for occasional noisy breathing. Because of the presence of a pulmonary sling, he was referred for surgery. A preoperative direct laryngoscopy and bronchoscopy showed almost complete (95%) tracheal rings from the glottis down to almost 2 cm proximal to the carina. There was no tracheal stenosis but some mild anterior compression of the mid-trachea and some posterior compression of the distal trachea (Fig 1c). The findings were confirmed intraoperatively (Fig 1d). The patient underwent division of the vascular ring by dividing the left ligamentum arteriosum, which arose from the distal main pulmonary artery and travelled backwards towards the descending aorta forming the ring, division, and re-implantation of the left pulmonary artery with extensive arterioplasty using autologous pericardial patch via median sternotomy and under cardiopulmonary bypass (Fig 2a). A thorough dissection of the oesophagus and in between the left subclavian and left carotid arteries was carried out in order to release any adhesions or potential fibrous ligaments, allow adequate mobility, and ensure no further compression existed. Flexible bronchoscopy at the end of surgery showed no evidence of compression of the trachea. The child was extubated in the operating room and did well postoperatively. A postoperative CT angiogram was performed and showed a widely patent left pulmonary artery (Fig 2b).
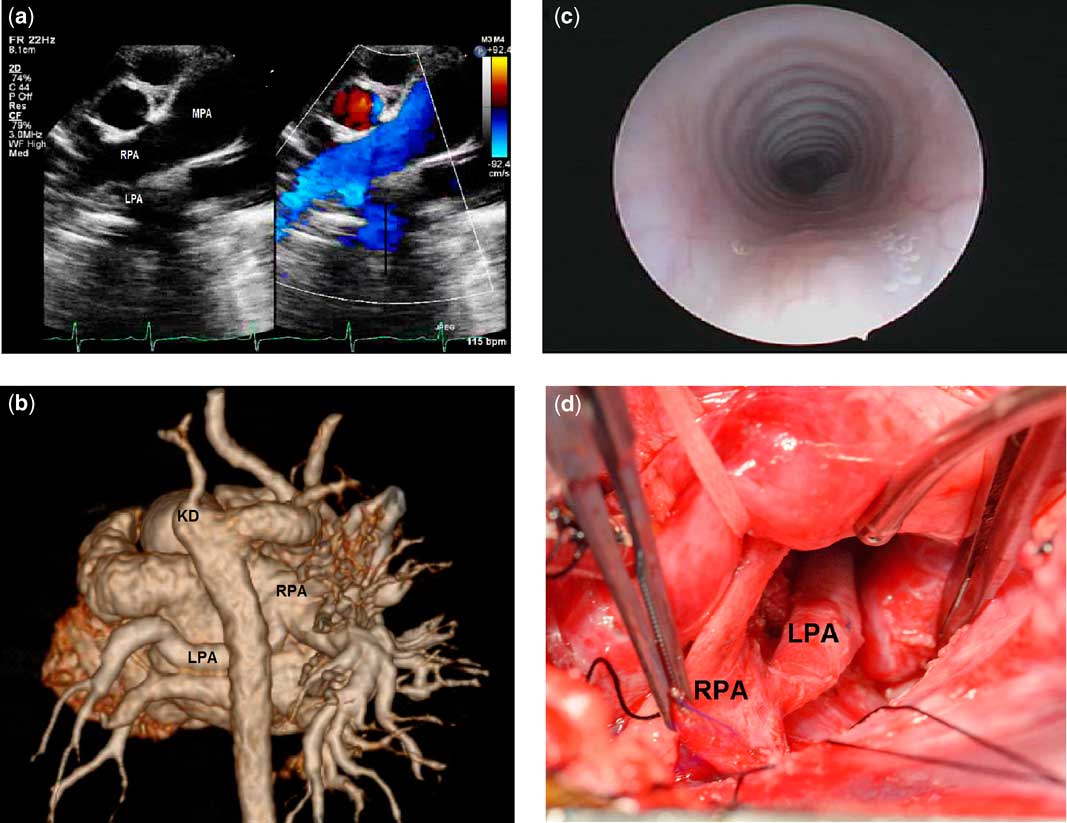
Figure 1 ( a ) A preoperative transthoracic echocardiogram showing the pulmonary artery sling. ( b ) A preoperative CT angiogram showing the right aortic arch, aberrant left subclavian artery, prominent diverticulum of Kommerell, and a left pulmonary artery (LPA) sling with a diffusely hypoplastic left pulmonary artery originating from the proximal right pulmonary artery (RPA). ( c ) A preoperative direct laryngoscopy and bronchoscopy showed almost complete (95%) tracheal rings from the glottis down to almost 2 cm proximal to the carina with no intrinsic stenosis and mild external compression. ( d ) An intraoperative picture showing the LPA coming off the RPA. KD=Kommerell’s diverticulum; MPA=main pulmonary artery.

Figure 2 ( a ) An intraoperative picture showing the re-implanted left pulmonary artery (LPA) after augmenting the vessel with pericardium. ( b ) A postoperative CT angiogram showing a widely patent re-implanted LPA. KD=Kommerell’s diverticulum; MPA=main pulmonary artery; RPA=right pulmonary artery.
Discussion
Pulmonary artery sling by definition is an aberrant left pulmonary artery that originates from the right pulmonary artery and passes leftwards around the right bronchus and between the lower trachea and oesophagus into the left hilum. Embryologically, the distal branch pulmonary arteries arise from the capillaries of their lung buds. Then, each branch pulmonary artery is joined with the ipsilateral sixth aortic arch. If this process fails, a pulmonary sling is formed when the connection between the left pulmonary artery – from the left lung bud – and the right sixth aortic arch – right pulmonary artery – occurs behind the trachea. This might happen as a consequence of the loss of the left sixth aortic arch. The presence of a right aortic arch and an aberrant left subclavian artery are the results of disappearance of the left fourth aortic arch, persistence of the right fourth aortic arch, which becomes the right arch, and loss of the left sixth aortic arch, except for the ductus arteriosus.Reference Lee, Printz, Hegde, Vargas and Sun 1 When the aforementioned developmental processes occur simultaneously, a pulmonary sling and a vascular ring may coexist. In all, 50–65% of left pulmonary artery slings are associated with complete tracheal rings, and of these 70–80% are associated with tracheal stenosis.Reference Fiore, Brown, Weber and Turrentine 2 , Reference Backer, Russell, Kaushal, Rastatter, Rigsby and Holinger 3 The patient described above has complete tracheal rings with no evidence of intrinsic stenosis. For that reason, we elected not to perform any kind of tracheoplasty manoeuvres. In our institution, the presence of complete tracheal rings per se does not necessitate tracheal intervention. On the other hand, an associated intrinsic stenosis would definitely require an intervention in the form of a sliding tracheoplasty, which is our method of choice in dealing with tracheal stenosis. Three main imaging modalities are used for the diagnosis and surgical planning, and these include echocardiogram, CT scan, and bronchoscopy. Intracardiac lesions, the course of the anomalous artery, the extent, and significance of tracheal stenosis must all be clearly delineated before surgery.
Potts et al performed the first surgical repair of a pulmonary artery sling in a 5-month-old patient through a right thoracotomy.Reference Potts, Holinger and Rosenblum 4 Since then, surgical technique has evolved into using cardiopulmonary bypass. The ideal approach for left pulmonary sling repair is through a median sternotomy on cardiopulmonary bypass as opposed to thoracotomy. This would reduce the incidence of postoperative pulmonary stenosis by providing adequate exposure for the proper orientation of the vessel. Nevertheless, there is still more than 50% risk of future stenosis of the re-implanted branched pulmonary artery in the first few months after surgery.Reference Wu, Downing and Mascio 5 To overcome this potential problem and the mild hypoplasia of the native vessel, we elected to augment the re-implanted left pulmonary artery with pericardium. In contrast to slings, the ideal approach for most vascular rings is through thoracotomy. Resecting Kommerell’s diverticulum and re-implanting the aberrant subclavian artery via median sternotomy incision is technically challenging. We elected to avoid doing that for two reasons. First, we had an adequate tissue recoil that we believed to be sufficient in relieving the vascular ring after dividing the ligamentum arteriosum. Second, the external tracheal compression was relieved without resecting the diverticulum. A similar case has been reported in literature that involved the prenatal diagnosis of an left pulmonary artery sling, as well as a right aortic arch with a left ductus arteriosus without Kommerell’s diverticulum resulting in a vascular ring. The infant underwent sliding tracheoplasty, left pulmonary artery re-implantation, and division of the ligamentum arteriosum on day of life 11 and he had residual postoperative left pulmonary artery and tracheal stenosis.Reference Jeong, Han, Hahn and Lee 6 Another case showed the association between pulmonary artery sling with right aortic arch and aberrant left subclavian artery with no ligamentum arteriosum. The child underwent an uneventful left pulmonary artery re-implantation. To our knowledge, this is the first report of a child with VACTERL association that has both an left pulmonary artery sling and a vascular ring.
Acknowledgements
None.
Financial Support
This research received no specific grant from any funding agency, commercial, or not-for-profit sectors.
Conflicts of Interest
None.
Ethical Standards
Permission was granted by the parents to publish the case report.