


Introduction
Congenital cholesteatoma is a rare entity. It arises from aberrant epithelial remnants left after closure of the neural groove, which occurs between the third and fourth weeks of embryonic life. Congenital cholesteatoma may present as hearing impairment or ear pain. Other presentations include vertigo (if the semicircular canals are eroded) or facial palsy (if the facial canal is eroded). Headache and fever indicate intracranial complications.Reference Mahanta, Uddin, Mohan and Sharp 1
Ear examination shows a pearly white mass medial to an intact tympanic membrane, in the antero-superior quadrant.Reference Kazahaya and Potsic 2
Levenson et al. have proposed the following diagnostic criteria for congenital cholesteatoma: (1) a normal pars tensa and pars flaccida; (2) no history of prior otorrhoea; and (3) no history of prior otological procedures.Reference Levenson, Parisier, Chute, Wenig and Juarbe 3
The pathogenesis of congenital cholesteatoma is poorly understood, with multiple theories reported in the literature. Teed has noted the presence of an ectodermal epithelial thickening which develops in proximity to the geniculate ganglion, medial to the neck of the malleus, and which undergoes involution to become the lining of the mature middle ear; if such involution fails, this may constitute the source of congenital cholesteatoma.Reference Teed 4 Alternatively, Michaels et al. have noted epidermoid formation in the antero-superior wall of the developing middle-ear cleft, failure of which to involute may be the basis for development of cholesteatoma in the anterior meso-tympanum.Reference Levenson, Michaels and Parisier 5
In this paper, we present congenital cholesteatoma presenting in two identical twins (brothers), an occurrence not previously reported in the world literature.
Case reports
Case one
An eight-year-old, Omani boy (‘twin one’) attended the ENT out-patient clinic with a history of right ear discharge. He had previously been treated at his local hospital for recurrent episodes of otitis media, with topical and oral antibiotics and decongestants.
On examination, the left ear was normal. Examination of the right ear showed a small, postero-superior perforation through which cholesteatoma flakes could be seen; a whitish mass was seen behind the remaining, intact pars tensa.
Paediatric audiometry showed mild conductive hearing loss in the right ear.
A high resolution computed tomography (CT) scan of the temporal bones revealed a soft tissue mass in the right middle ear, and opaque mastoid air cells (Figure 1).

Fig. 1 Axial, high resolution computed tomography scan of twin one's temporal bones, showing a soft tissue mass in the right middle-ear cavity, together with opaque mastoid air cells. L = left
The child underwent right mastoid exploration. Cholesteatoma was found to occupy the whole of the middle ear medial to the tympanic membrane, including the malleus, attic and aditus up to the fossa; the chorda tympani nerve was engulfed in the cholesteatoma sac. While the malleus was present, the incus and stapes superstructure were absent. The footplate was covered by the cholesteatoma sac lining. The facial canal and mastoid cells were intact.
The cholesteatoma was excised completely and a modified radical mastoidectomy was performed.
Post-operatively, the child did well.
Case two
Twin one's brother, also an eight-year-old Omani boy (‘twin two’), was brought to the ENT clinic by his father who was curious as to whether the child could have the same problem as twin one. Twin two had no prior history of otorrhoea, ear procedures or local trauma.
On examination, the left ear was normal (Figure 2a) but the right ear showed a pearly white mass behind an intact tympanic membrane (Figure 2b).
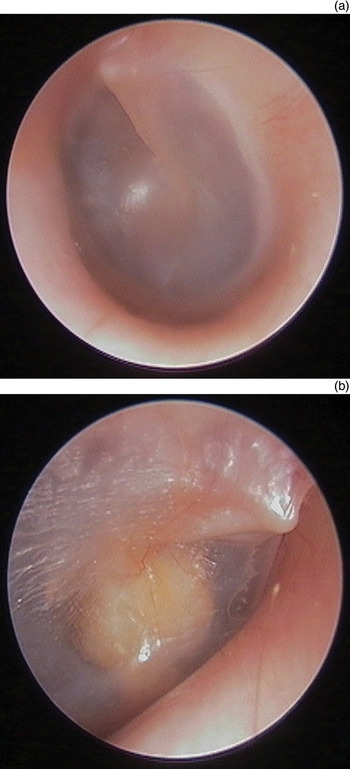
Fig. 2 Oto-microscopic view of twin two's ears, showing (a) a normal, intact left tympanic membrane, and (b) a pearly white mass behind the intact right tympanic membrane.
Paediatric audiometry showed mild conductive hearing loss in the right ear.
High resolution CT showed opacification of the right middle ear, aditus and antrum (Figure 3).

Fig. 3 Axial, high resolution computed tomography scans of twin two, showing opacification of the right middle-ear cavity.
Twin two underwent right mastoid exploration. The tympanic membrane was intact but a whitish mass could be seen beyond it in the middle ear. Cholesteatoma was found in the attic and in the anterior mesotympanum extending to the oval window, and extending medially to the incus and malleus up to the fossa incudis, eroding the anterior crura of the stapes and covering the footplate.
An atticotomy was performed via an endaural approach. All disease was removed. The incus (which was interposed between the footplate and the malleus handle) was removed and the head of the malleus nipped off.
Post-operatively, twin two did well.
Discussion
Congenital cholesteatoma may present at any age from infancy to adulthood, with a mean presentation age of 4.5 years. The male to female ratio is 3:1. The typical presentation is a pearly white mass behind an intact tympanic membrane.Reference Kojima, Miyazaki, Tanaka and Shiwa 6
Clinical symptoms are diverse and depend on the location and extent of the lesion. They may be completely absent, or alternatively may include conductive hearing loss, sensorineural hearing loss, ear fullness, labyrinthitis, facial palsy, tinnitus, vertigo and intracranial complications.
Representative aetiological hypotheses include a tympanic ring defect, epidermoid formation, epithelial metaplasia and epithelial implantation.Reference Friedberg 7 – Reference Michaels 9
Derlacki and Clemis have defined congenital cholesteatoma as an embryonic rest of epithelial tissue in the ear, without a tympanic membrane perforation nor any history of ear infection.Reference Derlacki and Clemis 10 However, this definition has been challenged by McGill et al., who have reported that approximately 70 per cent of children will have at least one episode of otitis media.Reference McGill, Merchant, Healy and Friedman 11
In the present report, twin one had been treated initially at his local hospital for recurrent episodes of otitis media.
Acquired cholesteatoma has previously been reported in families and in non-identical twins. However, there have been no previously published reports of congenital cholesteatoma arising in identical twins.
Homoe and Rosborg claimed to have published the first report of an affected family, with a mother and three of seven children having cholesteatoma, in Greenland.Reference Homoe and Rosborg 12
Prinsely reported a cluster of three families affected by cholesteatoma over several generations, in the East Anglia region of the UK.Reference Prinsely 13 In the first of these families, the affected members included non-identical twins aged five years, one presenting with bilateral and one with unilateral cholesteatoma.Reference Prinsely 13
Podoshin et al. studied the prevalence of chronic otitis media and cholesteatoma in 3056 members (10 years of age and older) of the kibbutzim in the northern part of Israel, and reported that 64 per cent of cholesteatoma patients had a family history of the condition.Reference Podoshin, Fradis, Ben David, Margalit, Tamir and Epstein 14
-
• Congenital cholesteatoma is rare
-
• This report describes congenital cholesteatomata in identical twins
-
• The clinical presentation of congenital cholesteatoma may vary
House and Sheehy have stated that the possibility of congenital cholesteatoma should be considered in patients with unilateral conductive hearing loss and without a clear diagnosis of unilateral otitis media with effusion, regardless of the patient's age.Reference House and Sheehy 15 Cholesteatoma in children is widely considered to be a more aggressive disease than in adults, for two major reasons: (1) extensive disease is found in children; and (2) higher rates of residual and recurrent disease have been documented in children.Reference House and Sheehy 15
The management of cholesteatoma is surgical. Early surgical intervention decreases the extent of the disease and reduces the risk of complications and recurrence. Both our reported cases were managed surgically.
Conclusion
Congenital cholesteatoma may present in various ways, from an incidental finding to conductive hearing loss, ear discharge, ear pain, facial palsy, vertigo and mastoid abscess. In the present paper, we report congenital cholesteatoma in identical twins, a previously unreported occurrence.



