



Introduction
Public health emergencies put enormous pressure on health care systems while revealing deep structural and functional problems in the organization of care. Reference Krausz, Westenberg, Vigo, Spence and Ramsey1 Developing the infrastructure and mobilizing the human resources are needed to counter a rapidly emerging outbreak of a highly contagious or lethal disease. Reference Agarwal, Nagi and Chatterjee2 In India, all efforts by the Central Government and various state governments are being directed towards augmenting the healthcare infrastructure for COVID-19 patients by converting existing healthcare facilities into dedicated COVID-19 facilities, expeditious commissioning of under construction healthcare projects, conversion of guest houses/hotels/banquet halls/into isolation facilities, conversion of stadiums/convention centers into COVID facilities, and creating makeshift COVID hospitals etc.
The All India Institute of Medical Sciences (AIIMS) located in New Delhi is at the forefront of fighting this pandemic. An under construction Burns and Plastic Surgery Block was completed in a speedy manner to be commissioned as a COVID Emergency Response Centre. Union Minister of Health and Family Welfare, Government of India also took stock of this ERC and expressed satisfaction over the preparations of the institute in fighting the COVID-19 pandemic. 3 A COVID task force comprising of medical professionals from various concerned specialties was also constituted.
Identifying facility for COVID-19 ERC
The Institute Building was constructed 70 years back and it has some upcoming blocks which are under various stages of construction. The COVID-19 Task Force, after surveying the various healthcare facilities (functional as well as buildings that are under construction) decided to convert an existing functional Trauma Centre into a dedicated COVID hospital, and an upcoming Burns and Plastic Surgery Block into a COVID Screening and Emergency Response Centre.
It was decided that the ground floor of Burns and Plastic Surgery Block may be organized as the Screening and Emergency Response Centre for suspected COVID-19 patients. It is an ideal location being away from the main campus (which houses approximately 2000 patients), however, the challenge was to make it operational and aggregate resources as it was an under-construction project (Table 1).
Table 1. Various patient care or support facilities in the Burns and Plastic Surgery Block converted to a COVID hospital

Commissioning COVID hospital under lock down
The task of getting an under-construction block completed and then aggregating resources for making it operational as a COVID hospital was extremely difficult during the complete lock down of the entire country. It was an arduous task to convince and mobilize human resource, as everyone feared the COVID-19 disease. It required exemplary coordination with various external agencies (private and public) and internal agencies i.e., on-ground staff to keep them motivated to carry out the work under the constant fear of acquiring the COVID-19 disease. Numerous letters and requests for movement passes were issued to ensure the movement of staff and resources from various parts of the city, transport vehicles were hired by the contracting firms to transport teams of workers/technicians, and police agencies and police posts at state borders were coordinated with. At times to mobilize materials from neighboring states, personal contacts with local administration/police agencies were harnessed. All the workers were provided counseling and all requisite safety devices/materials to enthuse their confidence. Work progress was ascertained on daily basis by the Project Officer, and multiple site visits by the Chief Executive Officer of the institute. Statutory clearances required from various agencies i.e., civic agencies for electricity connection, water, Delhi Fire Services etc., were expedited by the institute’s administration.
The project consultancy firm deputed an Operations Manager on site to coordinate with various agencies engaged by the consultancy firm and monitor the work progress while the engineering services division of the institute straightened out various issues faced during the completion of the block. Expeditious procurement using emergency clauses as laid out under the Government Financial Regulations were evoked for the timely procurement of required machinery and equipment items, also, resources were also pooled in from other hospitals/centers of the institute. It was decided on March 18, 2020 to commission this block expeditiously and lockdown was enforced from March 22, 2020.
The major challenge faced was the supply of medical oxygen, compressed air, and vacuum. It was decided that the execution should be the same as during a war by mobilizing required equipment (compressors, storage tanks, copper tubes etc.) from another under construction project within the institute. Medical gases that’d be sufficient for the entire COVID hospital was completed by deploying multiple teams (within a month – usual time duration for such work could vary from 6 to 9 months). Centralized oxygen supply was maintained through liquid oxygen tanks from the adjacent COVID center, while a local oxygen cylinder bank and emergency inlets were installed as a backup in the emergency area and various patient care areas on different floors. The OPD waiting area was converted to area for suspect COVID patients requiring medical oxygen (by making additional provision of centralized oxygen supply and suction outlets) (Figure 1).

Figure 1. Emergency triage area (Step 1 and step 2).
Screening area for suspect COVID-19 patients
The screening area for patients suspected of having mild and moderate COVID-19 illnesses was created. Screening was planned to be 2-step process with Triage 1 and Triage 2 stations. Patients having suspect severe COVID-19 illnesses or needing medical oxygen would be sent directly to the emergency area. A waiting area with physical distancing was created, having a dedicated washroom, hand washing and drinking facility, and educational materials which were displayed in the waiting hall (Figure 1).
First Triage
Patients having mild and moderate illnesses have to undergo a basic screening by administering a checklist (high risk group, contact history, symptoms, temperature and oxygen saturation) devised for the purpose, while those with flu-like symptoms requiring further evaluation will be sent to Triage 2, and the other patients will be discharged with proper advice. Triage 1 will be done by a doctor and a paramedic.
Second Triage
A detailed physical examination and vital monitoring along with innovative use of point of care ultrasound will be performed to detect any signs suggestive of Influenza like illnesses/acute lung injury. All those patients who will require further medical care will be sent inside the emergency department. This station will be manned by a doctor, a nurse and a paramedic. Patients would be tested as per the guidelines issued by the Ministry of Health and Family Welfare, Government of India.
Sampling booth
A sampling booth was created adjacent the triage area to be used for sampling the suspected patients for the COVID-19 illness, it was fitted with a system for changing gloves and an audio system to communicate with the patient standing outside for sampling (Figure 2). It had been designed and fabricated in-house with the help of the Central Workshop and Engineering Services Division; to not only prevent the exposure of personnel collecting samples to suspected COVID-19 patients, but also save Personal Protective Equipment (PPE). The items required for sampling i.e., swab stick, viral transport medium etc., will be kept outside on a ledge, and the area outside the sampling booth can be disinfected after each sampling. Collected samples (Nasal and Oropharyngeal swab) were stored locally in a fridge, and were sent to the Virology Department of the institute for nucleic acid extraction. These sampling stations will be disinfected after each patient to prevent cross transmission, and all steps and guidelines issued by the Ministry of Health and Health Family Welfare, Government of India will be adhered to.

Figure 2. Sampling booth for collection of nasal and oropharyngeal swab of suspected COVID-19 patients.
Sampling booths increase the patients’ access to the screening clinics and adequately protects healthcare personnel while reducing the consumption of personal protective equipment. It can also increase the number of people tested by 9–10 fold. However, there is a risk of cross- infection at each stage of the screening treatment, including the booths, and adverse reactions with disinfection of the booths. The good news is that it is possible to overcome these limitations by increasing the number of booths, reducing booth volume for sufficient and rapid ventilation, and using an effective, harmless, and certified environmental-friendly disinfectant. Reference Kim and Lee4
In-patient care areas
Various inpatient areas i.e., emergency area, wards and intensive care unit were created for handling COVID-19 patients (Figure 3). The emergency area has been divided into the red (patients requiring ventilatory support) and yellow area (patients requiring oxygen support). The ICU and 2 wards have each been prepared for admitting COVID-19 patients requiring inpatient care. Changing areas, donning areas, doffing areas, shower areas, etc., were also created on each floor for better infection control practices. This hospital is connected to the adjacent COVID hospital through a connecting bridge which can be used for movement of patients, staff and supplies.

Figure 3. Various patient care areas (emergency, observation area, wards, isolation rooms and ICU).
Various inpatient care areas have been divided into 3 zones i.e. clean area, contaminated area, and intermediate zone depending on the risk of exposure to the COVID-19 pathogen, and level of personal protective equipment requirement for these areas. Staff working in the contaminated areas need to don appropriate PPE as recommended by the Hospital Infection Control Committee guidelines issued by the Institute. Reference Kumar, Killedar and Singh5 A division between clean and contaminated areas has been maintained by using physical barriers and having separate air conditioning – the clean and contaminated areas were clearly labeled to prevent any crisscross movement of healthcare workers or materials which may pose as a threat to patient safety.
It is particularly important to identify circulation areas for movement of dirty and clean supplies. The first lift lobby has 3 lifts, lift 1 was earmarked as the contaminated lift lobby, the second was earmarked for moving dead bodies and dirty utility items, and the last lift was earmarked for moving patients. A separate lift lobby was earmarked as a clean lift for the movement of staff and clean supplies. Similarly, clean and contaminated staircase lobbies were distinctly identified and segregated, and adequate safeguards using 1-way doors, deploying security personnel, using access control etc., were put in place to prevent the crisscross movement of healthcare workers from clean to contaminated areas without wearing appropriate PPEs and vice versa.
Air conditioning of patient care and support areas
Air conditioning guidelines for COVID facilities issued by the American Society of Heating, Refrigerating and Air Conditioning Engineers (ASHRAE) suggests negative pressure in isolation areas. 6 Air conditioning in the existing healthcare facility have the provisioning of separate air handling units and ceiling suspended units for patient care and support areas respectively. Each ward and emergency area has a separate air handling unit having 6 air changes per hour with recirculated air and pre-filters in the air handling unit. The supply duct of AHU has a PHI (Photohydroionisation) Cell installed which helps in the destruction of microbes using patented technology. Reference Fink and Ellis7 Intensive care units have 100 percent fresh air with 12 air changes per hour with pre-filters, fine filters and HEPA filters at the air handling unit level. The ICU has been designed as individual patient care cubicles, and has cooled air coming through laminar air flow system, while the return air is goes out mechanically through exhaust ducts installed in the cubicle. Support and staff areas have separate air handling units for air conditioning and supplying recirculated air. Duct openings/closures were modified to prevent air mixing, and for ensuring better infection control.
Equipping patient care areas
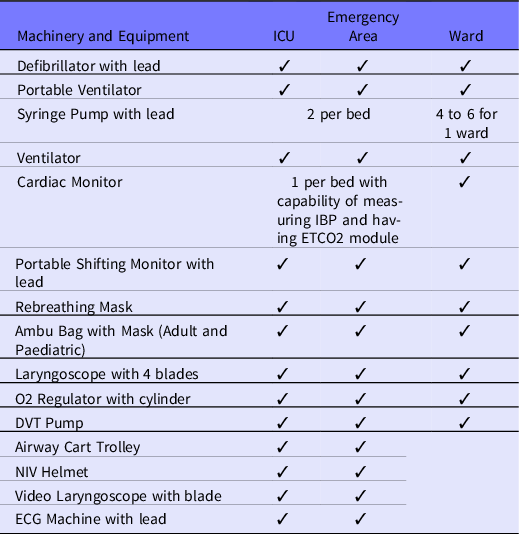
In an epidemic situation, it is ideal to have separate rooms for suspected and confirmed cases. Reference Ameli8,Reference Siegel, Rhinehart, Jackson and Chiarello9 Hence, it has been planned to keep 1 ICU and ward for suspected COVID-19 patients or patients exposed to confirmed COVID-19 cases. The ICUs on 2 floors were prepared by procuring and pooling the existing resources from various other hospitals under the administrative control of AIIMS, New Delhi (Table 2). Different levels of PPE kits assembled in-house have been planned for use depending on the type of patient care area or procedure being performed. Reference Siegel, Rhinehart, Jackson and Chiarello9 Various detailed SOPs were prepared for dealing with various hospital processes and infection control measures, i.e., screening of patients, traffic flow (men and material) in the hospital and patient care areas, donning and doffing of PPEs, decontamination of used linen (patient and staff), decontamination of used goggles, face shields and slippers, etc.
Table 2. Machinery and equipment and consumables required for equipping patient care areas
Conclusion
It was extremely challenging and required exemplary teamwork from all concerned stakeholders to transform an under construction building of a Burns and Plastic Surgery Block into a COVID emergency response center equipped to handle COVID emergencies and critically ill patients. Stress was laid on the provision of adequate machinery and equipment to handle critically ill patients, oxygen gas supplies on each hospital bed, segregation of hospital areas into various zones for better infection control, and preventing the transmission of infection. Mobilizing resources (machinery, manpower especially labor, consumables, etc.) during the lockdown required commitment from top leadership, virtuous motivated teams, expeditious procurements, coordination with multiple agencies, coordination with police agencies, arranging vehicles for the transportation of staff and labor, etc.
Acknowledgement
All the authors express their deep gratitude and acknowledge the efforts put in by Mr. Manjul Rastogi, the Superintending Engineer, AIIMS and his entire Engineering Services Division team, Mr. Narender Kumar and Ms. Archana Sharma, Stores Officer, AIMS and their entire team, Ms. Meera Kar, Deputy Nursing Superintendent, AIIMS and her entire team, Mr. Sunil Kumar, OTA In-charge for their exemplary work in the preparation of this COVID-19 Emergency Response Centre.





