


Introduction
Dermoid cysts are lesions consisting of displaced ectodermal structures positioned along lines of embryonic fusion. The cyst wall is characterised by epithelium-lined connective tissue, including skin appendages. The head and neck region is frequently involved, but intralingual dermoid cysts are extremely rare.Reference Dimtsas, Theologie-Lygidakis and Iatrou1–Reference Miles, Naidoo and Reddy3
Clinically, the lesion may grow slowly with an intact capsule, or may rupture with discharge of its contents. Keratin, sebum and hair may be present inside the cyst, and various radiological manifestations have been observed. The lesion may present as a solid mass or may contain liquid and/or fatty tissue.Reference Islam and Hoffman4
This case report discusses the challenges and clues leading to diagnosis, and gives a short review of the literature. The presented case demonstrates that, although rare, lingual dermoid cysts may present with a congenital discharging sinus and may mimic a lipoma radiologically.
Case report
History and clinical presentation
A 35-year-old man presented complaining of recurrent swelling of the floor of the mouth, with intermittent abnormal secretion from a congenital dorsum sinus. The symptoms had become more prominent in the past eight years, prompting the patient to seek treatment. The patient reported no significant pain, numbness or functional disturbance.
Physical examination revealed a mucosal orifice located in the midline of the central third of the tongue dorsum (Figure 1), which was found to be approximately 5 mm in depth on probing. No prominent excretion was elicited with pressure. The mouth floor was swollen, with the mucosa soft and non-tender on palpation. Routine blood tests revealed no remarkable findings.

Fig. 1 Clinical photograph of the lingual dorsum sinus. Note that the opening of the sinus (arrow) is located in the central middle third of the midline, far from the foramen caecum.
Imaging
Computed tomography (CT) images showed an oval, encapsulated, well demarcated mass approximately 6 × 5 × 4 cm in size, located in the midline of the tongue within the genioglossus muscle and above the geniohyoid muscles (Figure 2a to 2c). The mass was homogeneous and the attenuation was approximately −120 Hounsfield units.
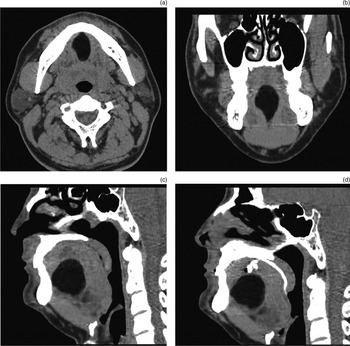
Fig. 2 (a) Axial, (b) coronal and (c) sagittal computed tomography (CT) images showing a well circumscribed lesion located within the genioglossus muscle and above the geniohyoid muscles, with a low attenuation value of approximately –120 Hounsfield units. (d) Sagittal CT sinograph showing a tract extending to the superior border of the cyst wall.
Computed tomography sinography was performed immediately after contrast media (Iopamiro, 370 mg l/ml; Bracco, Milan, Italy) had been injected through the dorsum orifice. The sinograph showed that the sinus tract extended to the superior margin of the capsule (Figure 2d).
Ultrasonography showed that the thyroid gland was present in the normal position.
Surgical management
As this lesion was clinically diagnosed as benign in nature, an intraoral excision was performed. En bloc resection of the mass and the sinus tract was performed under general anaesthesia. The mass was well circumscribed and easily dissected from the adjacent soft tissue. The mass was encapsulated by a dense, fibrous capsule. Yellowish, mucous sebum was present in the mass.
The course of recovery was uneventful.
Histopathological examination
The specimen was fixed in 10 per cent buffered formalin and embedded in paraffin for routine haematoxylin and eosin staining. Microscopically, the cyst wall was seen to be composed of keratinising, stratified squamous epithelium, with keratin present in the cyst cavity. Abundant sebaceous glands were present in the cyst wall. None of the major components showed any pleomorphism or immaturity (Figure 3).
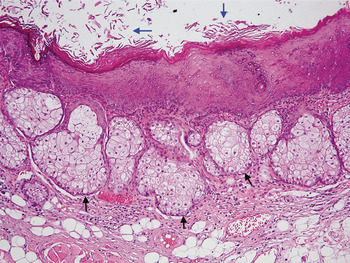
Fig. 3 Photomicrograph of the dermoid cyst showing the squamous epithelial cyst wall, which includes abundant sebaceous glands (black arrows); keratin is also seen within the cyst cavity (blue arrows). (H&E; ×200)
The final diagnosis of dermoid cyst with congenital dorsum discharging sinus was confirmed.
Discussion
Embryologically, the tongue develops mainly from a pair of lateral lingual processes which project from the inner surface of the mandibular arch and fuse in the midline. The fusion site of the processes is the median sulcus of the tongue.
The pathogenesis of lingual dermoid cyst and dorsum sinus is closely related to embryogenic disorders of the tongue. Theories of pathogenesis include: epithelial entrapment and proliferation during fusion;Reference Meyer5 failure of an embryonic cleft to disappear;Reference Raewyn and Paul6 differentiation of the displaced normal epithelial band into a serous gland; and traumatic implantation of epithelium.Reference Miles, Naidoo and Reddy3 The congenital sinus in the midline of the dorsum may be derived from abnormal persistence of the epithelial band,Reference Giunta, Friedman and Karp7 or from a cyst rupture dissecting the tongue muscle along the line of least resistance.Reference Korchin8 Confusingly, some authors have categorised dermoid cyst as a tumour. The presented case adds to our knowledge by suggesting that dermoid cysts may originate from abnormal embryogenesis rather than from an overgrowth of neoplastic cells. Thus, we believe that dermoid cysts should not be classified as tumours.
Thyroglossal duct cyst or sinus should be included in the differential diagnosis of a congenital tongue lesion with a sinus. Thyroglossal duct cysts and sinuses are caused by abnormal persistence or incomplete closure of the primitive thyroglossal duct. A thyroglossal duct cyst may occasionally develop within the tongue or in the floor of the mouth, and sometimes presents with a sinus extending to the foramen caecum. In our case, the sinus was located on the midline of the central third of the tongue, far from the foramen caecum. Thus, thyroglossal duct sinus could be excluded clinically.
The clinical course of a lingual dermoid cyst may be lengthy and the lesion may be symptomatic, depending upon its size. Difficulties in swallowing and sleeping may occur due to enlargement of the tongue.Reference Dimtsas, Theologie-Lygidakis and Iatrou1 Radiologically, dermoid cysts may appear as cystic, well demarcated lesions with fatty, fluid or mixed contents.Reference Becker, Mafee, Valvassori and Becker9 Fatty tissue components, where present, are specifically characterised by their low attenuation on CT images.Reference Mrad Dali-Grissa, Zrig, Mhiri-Souii, Arifa-Achour, Khochtali and Tlili-Graies10 In the present case, a CT attenuation value of –120 Hounsfield units strongly indicated the presence of a fatty component within the mass; this proved to be due to accumulated sebum from the abundant sebaceous glands within the cyst wall.
It is well known that lipomas typically exhibit low CT attenuation values of approximately –100 Hounsfield units. Lipomas can occasionally affect the tongue,Reference Dattilo, Ige and Nwana11, Reference Chung and Ng12 and may be solitary, intermuscular or intramuscular.Reference Nielsen and Mandahl13 Although lipoma should be considered based on radiological findings, there have been no reports of recurrent swelling and abnormal discharge from a congenital sinus, due to a lipoma. Thus, it should be borne in mind that these two separate pathological entities may have great radiological similarity.
• Lingual dermoid cyst is rare
• A congenital fistula may also be present discharging accumulated sebum
• In the presented case, computed tomography showed low-attenuation, homogeneous fatty tissue (resembling lipoma) due to sebum accumulation
Secretions from the sebaceous glands accumulate primarily within the cyst, and are discharged when the cyst becomes too large to withstand compression from the tongue muscles. Rupture of a dermoid cyst may occur when continued expansion is anatomically restricted.Reference Smith, Benson, Blaser, Mizushima, Tarr and Bellon14, Reference Kang, Kim, Seok and Lee15 In the presented case, the lesion developed in the midline of the tongue, within the genioglossus muscle. Muscle constriction during tongue movement made the lesion much more prone to rupture.
Dermoid cysts are sometimes associated with discharging sinuses, and can occur in the lip,Reference Kormanik, Bersu and Bentz16 nose,Reference Cambiaghi, Micheli, Talamonti and Maffeis17–Reference Morimoto, Takemoto, Nishikawa, Umegaki and Nishino19 tongue,Reference Giunta, Friedman and Karp7, Reference Korchin8 orbitReference Tien and Tien20 or other midline sites of the head and neck.Reference Shen, Chiou and Lin21–Reference Layadi, Louhab, Lmejjati, Aniba, Ait Elqadi and Ait Benali24 In the present case, the external opening of the sinus was situated in the midline of the dorsum of the middle third of the tongue, and the sinus itself extended to the superior margin of the cyst wall. A CT sinograph showed that the sinus did not communicate with the cyst directly, indicating that occult rupture of the cyst wall may have been responsible for the observed discharge.
Surgical excision is the preferred management for lingual dermoid cyst.Reference King, Smith and Burk25 Pre-operative evaluation of the location of the cyst in relation to the mylohyoid and geniohyoid muscles is important when deciding whether an intraoral or extraoral approach should be used for excision.Reference Meyer5 The prognosis is usually good, and recurrence is rare after complete surgical excision.
Conclusion
Lingual dermoid cyst may present with a congenital, discharging sinus in the midline of the dorsum of the tongue, and may mimic lipoma on CT.



