



There is mounting evidence that many forms of psychopathology begin early in life, with problems often appearing within a few years of birth, and can be expressed as a variety of clinical problems over the course of the lifespan (Copeland, Wolke, Shanahan, & Costello, Reference Copeland, Wolke, Shanahan and Costello2015b; Egger & Angold, Reference Egger and Angold2006; Garvey, Avenevoli, & Anderson, Reference Garvey, Avenevoli and Anderson2016). One of the strongest early childhood predictors of later psychopathology is irritability (Wakschlag et al., Reference Wakschlag, Perlman, Blair, Leibenluft, Briggs-Gowan and Pine2018).
Irritability is a transdiagnostic phenotype and facet of negative affectivity characterized by a tendency toward anger and temper outbursts (Stringaris & Taylor, Reference Stringaris and Taylor2015). Factor-analytic studies suggest that irritability is best conceptualized dimensionally spanning the normal–abnormal continuum (Wakschlag et al., Reference Wakschlag, Choi, Carter, Hullsiek, Burns, McCarthy and Briggs-Gowan2012, Reference Wakschlag, Estabrook, Petitclerc, Henry, Burns, Perlman and Briggs-Gowan2015), in that it is both a heritable trait that is relatively common in community samples of youth, and in more severe and dysregulated forms, a symptom of at least 10 DSM disorders. Even at relatively low levels, irritable children have a substantially higher risk for developing many common forms of psychopathology that span both the internalizing and externalizing spectrums (Copeland, Brotman, & Costello, Reference Copeland, Brotman and Costello2015a). The lack of specific associations between irritability and particular forms of psychopathology is especially apparent in studies of young children. For example, preschool irritability has been shown to predict depressive, anxiety, and behavioral disorders [ODD, conduct disorder (CD), and attention-deficit hyperactivity disorder (ADHD)] across childhood (Dougherty et al., Reference Dougherty, Smith, Bufferd, Stringaris, Leibenluft, Carlson and Klein2013, Reference Dougherty, Smith, Bufferd, Kessel, Carlson and Klein2015; Wakschlag et al., Reference Wakschlag, Estabrook, Petitclerc, Henry, Burns, Perlman and Briggs-Gowan2015).
The fact that early irritability observed in preschool-aged children predicts such a broad spectrum of psychopathology spanning both internalizing and externalizing disorders rather than any particular disorder or group of disorders (i.e. multifinality), raises questions about the mechanisms by which it leads to such phenotypically diverse outcomes and how to determine whether irritability will lead to clinical presentations that are relatively more internalizing v. those in which externalizing symptoms dominate.
Theorists have argued that there may be a number of biological and environmental moderators that shape the phenotypic expression of transdiagnostic vulnerabilities, like irritability, over the course of development (Beauchaine & Constantino, Reference Beauchaine and Constantino2017; Nolen-Hoeksema & Watkins, Reference Nolen-Hoeksema and Watkins2011). Specifically, Beauchaine and Constantino (Reference Beauchaine and Constantino2017) have hypothesized that variations in biological systems that have been shown to differentiate between pure disorders, such as amygdala reactivity, may steer the likelihood of whether irritability is expressed in a more internalizing v. externalizing fashion. Additionally, the effects of these factors may vary across developmental periods (Costello, Copeland, & Angold, Reference Costello, Copeland and Angold2011). However, very few studies have empirically tested this proposition and identified moderators that determine what specific symptoms irritable children will later develop and when.
Previous work from our laboratory has shown that the error-related negativity (ΔERN), an event-related potential that represents a neural index of error monitoring and differentiates internalizing from externalizing manifestations of psychopathology, interacts with very early irritability to predict internalizing and externalizing outcomes. We found that among children with higher levels of irritability at age 3, an enhanced ΔERN at age 6 predicted the development of more internalizing symptoms at age 9, whereas a blunted ΔERN at age 6 predicted the development of more externalizing symptoms at age 9, and these findings were relatively specific to anxiety and rule breaking behavior, respectively (Kessel et al., Reference Kessel, Meyer, Hajcak, Dougherty, Torpey-Newman, Carlson and Klein2016). However, at age 9, the prevalence of many forms of internalizing and externalizing psychopathology commonly associated with early childhood irritability (i.e. depression and CD) is low, as they often emerge or intensify during adolescence. To extend our previous findings, we examine early adolescent outcomes of irritability in preschool-aged children and speculate that stress system functioning may be another candidate psychobiological process that differentiates pure internalizing from pure externalizing psychopathology and steers the phenotypic expression of the more general liability reflected by early irritability along a continuum of internalizing to externalizing problems.
Sustained exposure to unhealthy levels of stress has been related to the development of various forms of psychopathology (Shirtcliff & Essex, Reference Shirtcliff and Essex2008). One easily accessible index of the limbic–hypothalamic–pituitary–adrenal axis, the primary biological stress system, is salivary cortisol. Cortisol secretion follows a diurnal cycle with elevated levels beginning shortly before awakening, followed by a rapid decrease throughout the day. A surge in morning cortisol followed by a steady decline primes the body for the demands of the pending day (Smyth et al., Reference Smyth, Ockenfels, Gorin, Catley, Porter, Kirschbaum and Stone1997). Low morning or high evening cortisol (i.e. a blunted diurnal cortisol slope) or unusually high morning and low evening cortisol (i.e. an abnormally steep diurnal cortisol slope) may signify stress system dysregulation (Shirtcliff & Essex, Reference Shirtcliff and Essex2008). Stress system dysregulation may place an individual at higher risk for psychological symptoms in the presence of some forms of adversity (Halligan, Herbert, Goodyer, & Murray, Reference Halligan, Herbert, Goodyer and Murray2007). At the same time, however, physiological responses to stress are also, to some degree, shaped by an individual's prior exposure to stress. Both acute and chronic stressors have been shown to dysregulate HPA axis activity, though the resulting pattern has been shown to depend on the type and duration of the stressor (Koss & Gunnar, Reference Koss and Gunnar2018). Thus, the diurnal slope may serve as a marker of a psychobiological mechanism through which the environment influences the development or presentation of later psychopathology. Indeed, both internalizing and externalizing behaviors have been linked to dysregulated cortisol rhythms in youth but in opposing directions (Koss & Gunnar, Reference Koss and Gunnar2018).
The majority of studies suggests that externalizing problems in middle childhood and adolescence are associated with a blunted diurnal cortisol slope, characterized by lower than typical morning levels and higher than typical evening levels in both cross-sectional (Kariyawasam, Zaw, & Handley, Reference Kariyawasam, Zaw and Handley2002; Moss, Vanyukov, & Martin, Reference Moss, Vanyukov and Martin1995; Pajer, Gardner, Rubin, Perel, & Neal, Reference Pajer, Gardner, Rubin, Perel and Neal2001; Shirtcliff, Granger, Booth, & Johnson, Reference Shirtcliff, Granger, Booth and Johnson2005) and longitudinal (McBurnett et al., Reference McBurnett, Raine, Stouthamer-Loeber, Loeber, Kumar, Kumar and Lahey2005; Platje et al., Reference Platje, Jansen, Raine, Branje, Doreleijers, de Vries-Bouw and Vermeiren2013; Salis, Bernard, Black, Dougherty, & Klein, Reference Salis, Bernard, Black, Dougherty and Klein2016) studies. However, there are exceptions to this pattern, as some studies fail to find any association (Azar et al., Reference Azar, Zoccolillo, Paquette, Quiros, Baltzer and Tremblay2004; Klimes-Dougan, Hastings, Granger, Usher, & Zahn-Waxler, Reference Klimes-Dougan, Hastings, Granger, Usher and Zahn-Waxler2001; van Bokhoven et al., Reference van Bokhoven, Van Goozen, van Engeland, Schaal, Arseneault, Seguin and Tremblay2005) and a few have reported a positive association (Gerra et al., Reference Gerra, Zaimovic, Avanzini, Chittolini, Giucastro and Caccavari1997; McBurnett et al., Reference McBurnett, Raine, Stouthamer-Loeber, Loeber, Kumar, Kumar and Lahey2005; van Bokhoven et al., Reference van Bokhoven, Van Goozen, van Engeland, Schaal, Arseneault, Seguin and Tremblay2005). The pattern of associations between cortisol and internalizing behaviors tends to be the opposite of externalizing behaviors, though findings have been less consistent and these studies have focused on morning cortisol rather than the diurnal slope. In the cross-sectional literature, a number of studies have reported that higher morning cortisol levels are associated with internalizing problems (LeMoult, Ordaz, Kircanski, Singh, & Gotlib, Reference LeMoult, Ordaz, Kircanski, Singh and Gotlib2015; Lok et al., Reference Lok, Mocking, Ruhe, Visser, Koeter and Assies2012; Lopez-Duran, Kovacs, & George, Reference Lopez-Duran, Kovacs and George2009; Ruttle et al., Reference Ruttle, Shirtcliff, Serbin, Fisher, Stack and Schwartzman2011), although some have found that lower cortisol levels are associated with internalizing behaviors (De Bellis et al., Reference De Bellis, Dahl, Perel, Birmaher, Al-Shabbout and Williamson1996). The prospective literature is more consistent, as most longitudinal studies report that elevated morning cortisol levels predict later internalizing symptoms in both children and adolescents (Goodyer, Herbert, Tamplin, & Altham, Reference Goodyer, Herbert, Tamplin and Altham2000; Halligan et al., Reference Halligan, Herbert, Goodyer and Murray2007). Importantly, inconsistencies in the literature regarding the pattern of associations between cortisol and internalizing and externalizing behaviors may be due to the fact that few studies account for the substantial comorbidity between these two dimensions of psychopathology.
The current study capitalized on existing data from a well-designed cohort study of adolescents who were first assessed at age 3 and reassessed at 3-year intervals to determine whether variation in the diurnal cortisol pattern moderates developmental pathways between preschool irritability and internalizing and externalizing symptoms 9 years later. We hypothesized that among 3-year olds with higher levels of irritability, an enhanced diurnal cortisol slope at age 9 would predict an increase in internalizing symptoms at age 9. We also hypothesized that among those same children, a blunted diurnal cortisol slope at age 9 would predict an increase in externalizing symptoms at age 12. As irritability has been shown to be moderately stable across development (Vidal-Ribas et al., Reference Vidal-Ribas, Brotman, Valdivieso, Leibenluft and Stringaris2016), though tends to decline with age from childhood to adolescence (Stringaris et al., Reference Stringaris, Goodman, Ferdinando, Razdan, Muhrer, Leibenluft and Brotman2012), a second, more exploratory aim, was to evaluate whether diurnal cortisol slope at age 9 also predicted the continuity of irritability at age 12.
Method
Participants
Families (N = 559) with 3-year-old children (M = 3.55 years, s.d. = 0.43) were recruited through commercial mailing lists. Children with no significant medical condition or developmental disabilities who were living with at least one English-speaking biological parent were eligible to participate. In total, 541 parents (primarily mothers) completed a diagnostic clinical interview and questionnaires regarding their 3-year-old child. Of these 541, 383 families went on to participate in the saliva data collection when children were approximately 9 years old (M = 9.19, s.d. = 0.40). Three years later, when children were 12 years old (M = 12.75, s.d. = 0.50), 354 of these 383 mothers again reported on their child's psychological functioningFootnote †Footnote 1. Full information on maximum likelihood estimation was used in analyses to account for missing data. Thus, the analytic sample included 541 participants.
Measures
Preschool irritability
Irritability at age 3 was assessed with the Preschool Age Psychiatric Assessment (PAPA) (Egger et al., Reference Egger, Erkanli, Keeler, Potts, Walter and Angold2006). A 3-month primary period was used to enhance recall, but symptom-onset dates were obtained for all criteria. PAPA items were rated for intensity, frequency, and duration. Six items from the PAPA were used to assess irritability. Items corresponded to items from the Affective Reactivity Index, a parent- and child-reported chronic irritability scale for older youth (Stringaris et al., Reference Stringaris, Goodman, Ferdinando, Razdan, Muhrer, Leibenluft and Brotman2012). In addition, to assess whether the child experienced irritable mood states for a long time, this criterion was coded present if the child was rated as having at least a 30 min duration on irritable mood, being prone to frustration, annoyance or anger, or having difficulty recovering from temper tantrums. The total irritability scale consisted of the sum of symptoms coded as present according to the intensity, frequency, and duration criteria described by Dougherty et al. (Reference Dougherty, Smith, Bufferd, Stringaris, Leibenluft, Carlson and Klein2013, Reference Dougherty, Smith, Bufferd, Kessel, Carlson and Klein2015). The Cronbach α coefficient of internal consistency for the irritability scale was 0.74.
Child internalizing and externalizing symptoms
Mothers reported on children's symptoms using the CBCL (Achenbach & Rescorla, Reference Achenbach and Rescorla2000, Reference Achenbach and Rescorla2001). We used the CBCL 1½–5 when children were 3 years old and the CBCL 6–18 when children were 12 years old. On each questionnaire, parents evaluate the severity of internalizing and externalizing symptoms using a scale from 0 (never true) to 3 (very true or often true). At age 12, we also examined the CBCL internalizing (anxious/depression: 13 items; withdrawn/depression: eight items; somatic complaints: 11 items) and externalizing (rule breaking: 15 items; aggression: 18 items; attention problems: 10 items) subscales. To ensure that overlapping irritability symptoms (CBCL 1½–5: ‘easily frustrated’, ‘angry moods’, ‘stubborn, sullen, or irritable’, ‘sudden changes in mood or feelings’, ‘temper tantrums or hot temper’; CBCL 6–18: ‘sulks a lot’; ‘stubborn, sullen, or irritable’; ‘sudden changes in mood or feelings’; and ‘temper tantrums or hot temper’) captured in the age 3 internalizing and externalizing scales, and age 12 externalizing scale and aggression subscale did not account for the predictive association between preschool irritability and later psychopathology, we removed these items and recalculated non-overlapping scales. Coefficient α was 0.84 (35 items) for the recalculated internalizing scale at age 3 and 0.87 (32 items) for the internalizing scale at 12. Coefficient α for the recalculated externalizing scales was 0.88 (20 items) and 0.85 (31 items) at ages 3 and 12, respectively.
Age 12 irritability
Mothers reported on children's irritability using the ARI (Stringaris et al., Reference Stringaris, Goodman, Ferdinando, Razdan, Muhrer, Leibenluft and Brotman2012), a six-item parent-report questionnaire that assesses irritability in children over the past 6 months (α = 0.85). The scale has good reliability, both internally and across informants, and convergent and discriminant validity (Stringaris et al., Reference Stringaris, Goodman, Ferdinando, Razdan, Muhrer, Leibenluft and Brotman2012).
Cortisol
When children were 9 years old, they collected saliva samples three times per day over three consecutive days. Parents were asked to assist their children in taking saliva samples right after they woke up in the morning, 30 min after waking up, and 30 min before going to bed. Only the waking and bedtime samples were used in this analysis to capture diurnal slope (i.e. the wake-up level to the evening nadir in cortisol), as the rise in cortisol from wake to 30 min, or the cortisol awakening response, is imposed on the diurnal rhythm and its underlying regulatory mechanisms are independent from the rest of the diurnal cycle (Edwards, Clow, Evans, & Hucklebridge, Reference Edwards, Clow, Evans and Hucklebridge2001). Children were asked to passively drool into a polypropylene tube using a straw, then label each tube with the date and time. Parents instructed children not to eat or drink for 30 min before each sample. After 3 days, samples were either mailed back to the laboratory or retrieved by research assistants. Samples were stored at −20 °C before being sent to Trier, Germany for assay. Samples were assayed in duplicate using a time-resolved immunoassay with fluorometric detection (DELFIA)Footnote 2.
Any cortisol value that was three standard deviations above the mean was excluded, resulting in 19 excluded samples. Samples were also excluded if the child was taking an oral or inhaled corticosteroid, antipsychotic, or methylphenidate – extended release (Concerta) during sample collection, as these medications have been shown to affect hormone levels in children and adolescents (Granger et al., Reference Granger, Fortunato, Beltzer, Virag, Bright and Out2012). Seventy samples were excluded due to medication use. In addition, any waking sample that was taken more than 15 min after waking time, as determined by self-report, was excluded. This resulted in a total of 87 waking samples being excluded across the three study days. Intra-assay coefficients of variation (CVs) were between 4.0% and 6.7%, and inter-assay CVs ranged from 7.1% to 9.0%.
Data analysis
We utilized a latent change model to estimate cortisol slope, following procedures used in previous studies (Bernard, Peloso, Laurenceau, Zhang, & Dozier, Reference Bernard, Peloso, Laurenceau, Zhang and Dozier2015; Kertes, Gunnar, Madsen, & Long, Reference Kertes, Gunnar, Madsen and Long2008). To parse out observed scores from error variance, we created latent factors for wake-up and evening cortisol using the daily values as indicators. Cortisol slope was modeled as a latent difference score between evening and morning samples (i.e. Bedtime–Wake-up). In this model, more negative values indicate a steeper slope across the day, whereas more positive values indicate a blunted slope. By accounting for measurement error, latent change models allow for more reliable and less biased estimates of change (Burt & Obradovic, Reference Burt and Obradovic2013) compared to simple difference scores (King et al., Reference King, King, McArdle, Grimm, Jones and Ollendick2006; McArdle, Reference McArdle2009).
Models were estimated using full information maximum likelihood estimation with standard errors approximated by first-order derivatives (see Fig. 1). FIML utilizes all available information to estimate parameters in models with missing data (Enders & Bandalos, Reference Enders and Bandalos2001). This method has been shown to be a reliable way to account for missing data in latent variable interaction models (Cham, Reshetnyak, Rosenfeld, & Breitbart, Reference Cham, Reshetnyak, Rosenfeld and Breitbart2017).

Fig. 1. Conceptual diagram illustrating the latent difference model of the cortisol slope. Cortisol slope was modeled as a latent difference score between evening and morning samples (i.e. Bedtime–Wake-up). More negative values indicate a steeper slope across the day, whereas more positive values indicate a blunted slope.
The main question of the current study concerns whether variation in the diurnal pattern of cortisol moderates developmental pathways between preschool irritability and subsequent internalizing and externalizing symptoms in early adolescence. Thus, we ran moderated multiple regression models testing the interactive effects of diurnal cortisol slope and early childhood irritability on adolescent internalizing and externalizing symptoms. We initially ran two separate multiple regression models with age 3 irritability and diurnal cortisol slope predicting age 12 internalizing and externalizing symptoms to examine main effects. Next, we re-ran the multiple regressions including the cross-product term for the interaction between age 3 irritability and age 9 diurnal cortisol slope (using latent change scores). In these models, we included age 3 internalizing and externalizing symptoms to adjust for preexisting internalizing and externalizing symptoms. We also included gender, co-occurring age 12 symptoms, and irritability in order to identify unique predictors of internalizing and externalizing symptoms, respectively.
To examine our second, and more exploratory, aim of whether diurnal cortisol slope at age 9 also predicted the continuity of irritability at age 12, we tested a third moderation model. However, in this model, we did not adjust for co-occurring age 12 internalizing and externalizing symptoms, as the unique part of irritability that is unrelated to these symptoms may not have substantive meaning.
To probe significant interactions, simple slope terms were tested (Aiken, West, & Reno, Reference Aiken, West and Reno1991) and to determine the values of irritability at which varying levels of age 9 diurnal slope differed significantly on age 12 symptoms, we conducted a regions of significance test (RoS; Hayes & Matthes, Reference Hayes and Matthes2009).
Finally, given that variation in diurnal cortisol pattern may moderate developmental pathways between preschool irritability and only specific symptom dimensions comprising the internalizing and externalizing spectrums, respectively, we also conducted follow-up analyses in which we replaced age 12 internalizing and externalizing symptoms as the dependent variable with each of their respective subscales (internalizing: anxious/depressed, withdrawn/depressed, and somatic complaints; externalizing: attention problems, aggressive behavior, and rule breaking). We continued to adjust for age 3 internalizing and externalizing, rather than the corresponding subscale, in these models as some of the subscales in the CBCL 1½–5 do not correspond to the subscales in the CBCL 6–18 (see Appendix for results).
Results
Table 1 presents the descriptive statistics and bivariate correlations of the major study variables. As expected, irritability and internalizing and externalizing symptoms at both ages 3 and age 12 showed moderate concurrent associations. From age 3 to age 12, irritability and internalizing and externalizing symptoms showed moderate within and between construct associations. Age 9 diurnal slope was not correlated with any symptom variables at age 3 or 12.
Table 1. Descriptive statistics and bivariate associations between variables

*p ⩽ 0.05, **p < 0.01, ***p < 0.001.
Effects of age 3 irritability, age 9 diurnal slope, and their interaction on the development of age 12 internalizing symptoms
Greater age 3 internalizing symptoms, age 12 externalizing symptoms, and age 12 irritability predicted greater age 12 internalizing symptoms. The main effects of gender, age 3 irritability and externalizing symptoms, and age 9 diurnal slope on age 12 internalizing symptoms were not significant. However, there was a significant interaction between age 3 irritability and age 9 diurnal slope (see Table 2 and Fig. 2). For children with a steeper or more negative diurnal slope, greater early persistent irritability predicted increased internalizing symptoms at age 12 [b = 1.19 (0.51) p < 0.05]. In contrast, among children with a less steep slope, early persistent irritability did not significantly predict age 12 internalizing symptoms [b = −0.89 (0.54), p = 0.10]. The RoS revealed that when irritability was >−0.19 s.d. below the mean, a more negative or steeper diurnal slope was associated with an increase in age 12 internalizing symptoms.
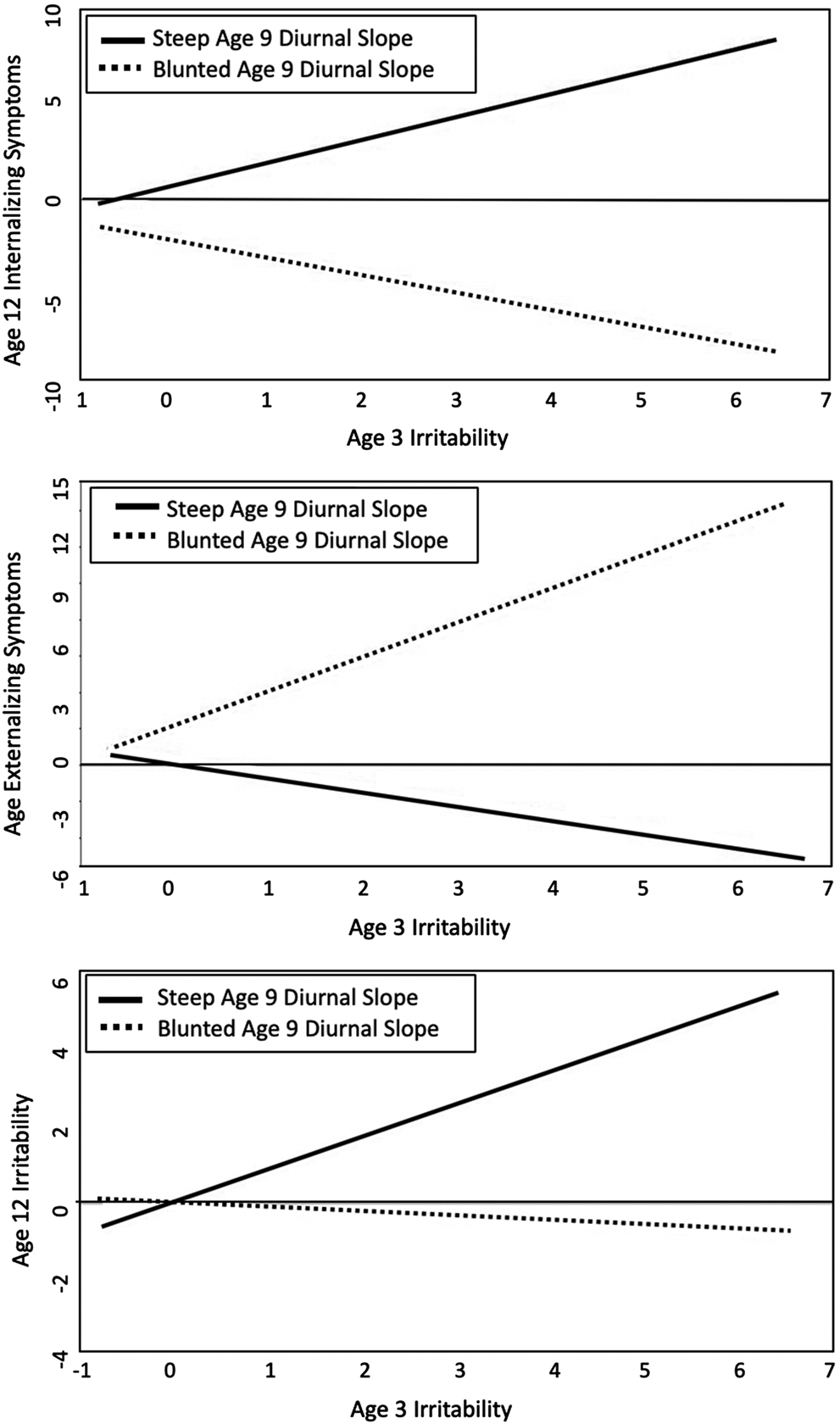
Fig. 2. Significant interactions between early persistent irritability and the age 9 diurnal slope at 1 s.d. above and below the mean in predicting age 12 internalizing (top) and externalizing (middle) symptoms and age 12 irritability (bottom).
Table 2. Multiple regressions with age 3 irritability and age 9 diurnal slope (Model 1) and their interaction (Model 2) predicting children's internalizing (top) and externalizing (middle) symptoms and irritability (bottom) at age 12

*p ⩽ 0.05, **p < 0.01, ***p < 0.001.
Effects of age 3 irritability, age 9 diurnal slope, and their interaction on the development of age 12 externalizing symptoms
Greater age 3 externalizing symptoms and age 12 irritability and internalizing symptoms predicted greater age 12 externalizing symptoms. The main effects of gender and age 3 irritability and internalizing symptoms and age 9 diurnal cortisol slope on age 12 externalizing symptoms were not significant. However, there was a significant interaction between age 3 irritability and age 9 diurnal slope (see Table 2 and Fig. 2). For children with a steeper or more negative diurnal slope, greater early persistent irritability did not predict externalizing symptoms at age 12 [b = −0.52 (0.35), p = 0.14]. In contrast, among children with a less steep or more blunted slope, early persistent irritability significantly predicted increased age 12 externalizing symptoms [b = 1.15 (0.41) p < 0.01]. An RoS test revealed that when irritability was > –0.15 s.d. below the mean, a more blunted or less steep diurnal slope was associated with increases in age 12 externalizing symptoms.
Effects of age 3 irritability, age 9 diurnal slope, and their interaction on the development of age 12 irritability
Male gender and greater age 3 irritability and externalizing symptoms were associated with greater age 12 irritability. However, the significant main effect of age 3 irritability was qualified by a significant interaction with age 9 diurnal slope (see Table 2 and Fig. 2). There were no significant main effects for age 3 internalizing symptoms or age 9 diurnal slope. For children with a steeper or more negative diurnal slope, greater early persistent irritability significantly predicted increases in irritability at age 12 [b = 0.84 (0.28), p < 0.01]. In contrast, among children with a less steep or more blunted slope, there was no significant association between age 3 irritability and 12 irritability [b = −0.13 (0.28) p = 0.66]. An RoS test revealed that when irritability was greater than the mean, a more negative or steeper diurnal slope was associated with increases in age 12 irritability.
Discussion
This study explored how early irritability leads to phenotypically diverse outcomes over the course of development. We examined whether individual differences in the diurnal cortisol slope, a measure of HPA axis functioning, predicts whether preschool irritability is associated with later internalizing v. externalizing outcomes in early adolescence. We found that among children with higher levels of irritability at age 3, a steeper diurnal cortisol slope at age 9 predicted the development of more internalizing symptoms at age 12, whereas a blunted diurnal cortisol slope at age 9 predicted the development of more externalizing symptoms at age 12. Importantly, these longitudinal associations were apparent after adjusting for preexisting internalizing and externalizing symptoms at age 3 and irritability at age 12, indicating that these effects are not an artifact of preexisting symptoms or co-occurring irritability. Furthermore, we found that among children with higher levels of irritability at age 3, a steeper diurnal cortisol slope at age 9 also predicted increases in irritability at age 12.
Previous research indicates that stress system functioning can have opposing associations with externalizing and internalizing psychopathology (Koss & Gunnar, Reference Koss and Gunnar2018), although the results have been somewhat inconsistent. In the present study, cortisol slope was not correlated with internalizing or externalizing symptoms at age 3 or 12. However, we found that diurnal cortisol slope predicted age 12 internalizing symptoms after adjusting for prior and concurrent externalizing symptoms, and vice versa. This suggests the importance of accounting for comorbidity between these two dimensions of psychopathology when examining associations between diurnal cortisol and internalizing and externalizing outcomes. Additionally, at low levels of early irritability, diurnal cortisol slope did not predict the development of either internalizing or externalizing symptoms in early adolescence. This suggests that variation in diurnal cortisol slope in and of itself may not be associated with psychopathology, but instead interacts with, and possibly shapes, the specific expression of a more general liability for psychopathology, like irritability.
Thus, our results suggest that stress system regulation plays a role in moderating the influence of early childhood irritability on later internalizing and externalizing outcomes in early adolescence. Preschoolers with higher levels of irritability who later exhibit a blunted diurnal rhythm may be more inclined to externalize as a result of the aversive physiological states associated with low arousal (Brennan & Raine, Reference Brennan and Raine1997). In contrast, children with higher levels of irritability and with a steeper than normal cortisol slope may be hyperreactive to stressful experiences and consequently internalize (Koss & Gunnar, Reference Koss and Gunnar2018; Lopez-Duran et al., Reference Lopez-Duran, Kovacs and George2009).
Recent research suggests that early but not later irritability shares a strong genetic risk for ADHD, which has led some to argue that early irritability is better conceptualized as an early neurodevelopmental manifestation of ADHD, and that irritability later in life may be relatively distinct (Riglin et al., Reference Riglin, Eyre, Cooper, Collishaw, Martin, Langley and Thapar2017). Our findings partially support this notion in that an enhanced diurnal cortisol slope moderated the association between early and later irritability, such that a steeper diurnal cortisol slope was associated with homotypic continuity of irritability from preschool to early adolescence. This suggests that irritability in adolescence may be heterogeneous, and that HPA functioning may be a marker for a homotypic pathway.
Follow-up analyses examining the specificity of early irritability and the diurnal cortisol slope with respect to internalizing and externalizing outcomes (see Appendix) suggested that our findings are most applicable to the anxious/depressed, somatic complaints, rule breaking, and aggression subscales. We also found that children with higher levels of irritability who had a blunted diurnal cortisol slope at age 9 went on to develop fewer withdrawn/depression symptoms at age 12. Thus, a blunted diurnal cortisol slope in the context of high levels of irritability may play a protective role against some forms of internalizing psychopathology. Finally, diurnal cortisol moderated the relationship between early irritability and attention problems. Although the relationship took opposing directions as a function of diurnal slope, neither of the simple slopes was significant on their own.
Some investigators suggest that early irritability reflects a non-specific liability to develop psychopathology (Lahey, Krueger, Rathouz, Waldman, & Zald, Reference Lahey, Krueger, Rathouz, Waldman and Zald2017; Mulraney, Melvin, & Tonge, Reference Mulraney, Melvin and Tonge2014) and may be a salient early developmental feature of a general psychopathology factor, or P, that accounts for the shared association between internalizing and externalizing in structural models of psychopathology (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Lahey et al., Reference Lahey, Krueger, Rathouz, Waldman and Zald2017; Olino, Dougherty, Bufferd, Carlson, & Klein, Reference Olino, Dougherty, Bufferd, Carlson and Klein2014). In these models, P is represented as a general bifactor that is orthogonally related to higher order internalizing (I) and externalizing (E) factors. P has been proposed to represent non-specific etiological factors that include pleiotropic genetic effects, dispositional traits, and/or broad-acting environmental exposures to enhance the risk for any and all disorders. I and E are thought to represent more specific casual factors that influence the specific phenotypic expression of psychopathology (Caspi et al., Reference Caspi, Houts, Belsky, Goldman-Mellor, Harrington, Israel and Moffitt2014; Lahey et al., Reference Lahey, Krueger, Rathouz, Waldman and Zald2017). Our findings are consistent with this view, as we have found both in the current study and in our previous work (Kessel et al., Reference Kessel, Meyer, Hajcak, Dougherty, Torpey-Newman, Carlson and Klein2016) that psychobiological processes that differentiate internalizing from externalizing psychopathology, like the ΔERN and diurnal cortisol slope, appear to steer the phenotypic expression of early irritability along a continuum from relatively greater internalizing to relatively greater externalizing problems in early adolescence. It remains to be seen whether the ΔERN and diurnal cortisol slope continue to predict the phenotypic expression of early forms of irritability at older ages and whether it does so in a uniform or time-varying fashion across development. We are continuing to follow this sample in order to examine these questions.
This study had several strengths. First, we identified a biological variable that influenced the clinical expression of a transdiagnostic construct that may reflect a general liability to phenotypically distinct psychopathological outcomes. This approach can guide further exploration of the mechanisms by which other transdiagnostic factors lead to phenotypically diverse outcomes. Second, we used an unselected community sample, which is important as irritability is common in the course of development, and allowed us to explore the full range of variation in all our variables. Finally, our prospective longitudinal design allowed us to examine development over a 9-year period.
Despite these strengths, this study also has limitations. First, as there is no validated measure for persistent irritability in preschoolers, we derived our own measure using items from a well-validated diagnostic interview (Egger et al., Reference Egger, Erkanli, Keeler, Potts, Walter and Angold2006) and guided by the content of a well-validated scale for irritability in older children (Stringaris et al., Reference Stringaris, Goodman, Ferdinando, Razdan, Muhrer, Leibenluft and Brotman2012). Although it was derived ad hoc, our measure has shown good concurrent and predictive validity in previous reports (Dougherty et al., Reference Dougherty, Smith, Bufferd, Stringaris, Leibenluft, Carlson and Klein2013, Reference Dougherty, Smith, Bufferd, Kessel, Carlson and Klein2015). Second, while a community sample allows for greater generalization, it may not be as readily applicable to children with clinical levels of internalizing or externalizing problems. Indeed, only about 10% of the current sample showed clinical or borderline clinical levels of internalizing or externalizing problems according to the CBCL. Thus, future work should attempt to replicate these findings in a clinical sample. Third, we were unable to assess diurnal cortisol slope at age 3; hence, we cannot determine how early in development stress system functioning begins to influence the link between irritability and internalizing and externalizing symptoms. Finally, the current study only included parent-reported symptoms which may have diminished our ability to detect the full range of internalizing symptoms at age 12. As self-reported, compared to parent-reported, internalizing problems tend to be higher early adolescence (Achenbach, McConaughy, & Howell, Reference Achenbach, McConaughy and Howell1987), parent-reported levels at age 12 may be an underestimation.
The present study is the first to examine the role of stress system functioning as a potential developmental mechanism through which the transdiagnostic construct of irritability leads to subsequent internalizing and externalizing psychopathology across development. Our results suggest that variation in diurnal cortisol slope influences developmental trajectories from preschool irritability to later internalizing and externalizing outcomes in preadolescence. These findings underscore the importance of considering the dynamic interplay of different units of analysis across development when examining transdiagnostic constructs, like irritability, in understanding the development of multifinality in youth psychopathology. They also point to the possible utility of using measures of stress system functioning, like diurnal cortisol slope, to anticipate which direction an irritable child's subsequent psychopathology is likely to take in order to inform prevention and intervention efforts.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0033291719003684.
Acknowledgements
This work was supported by NIMH Grants: RO1MH069942 to DNK; and F31MH111172 to EMK.
Conflict of interest
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.






