


Introduction
The prevalence of unilateral sensorineural hearing loss (SNHL) in newborns is reported to be between 0.1 and 3 per cent.1 More than half of patients with unilateral SNHL are not diagnosed early, with around 60 per cent having normal hearing at birth, based on newborn hearing screening.Reference Ghogomu, Umansky and Lieu2
When the diagnosis of unilateral hearing loss is confirmed to be sensorineural, imaging of the cochlear and retrocochlear pathway is performed. Imaging is conducted to investigate for an aetiology of the hearing loss and to rule out concurrent intracranial and extracranial abnormalities. The imaging scan findings can identify abnormalities that predict progression of the hearing loss, change family counselling regarding high-risk activities that may cause further hearing loss, or indicate likely concurrent health issues such as thyroid disease. Cochlear implant candidacy is also influenced by imaging findings. Specifically, cochlear implantation is usually considered in patients with no structural retrocochlear abnormalities.
Cochlear nerve hypoplasia or aplasia is an increasingly recognised cause of paediatric SNHL. In 2017, Usami et al. reported a 43 per cent prevalence of cochlear nerve deficiency in paediatric patients who underwent computed tomography and/or magnetic resonance imaging (MRI) to investigate severe-to-profound unilateral hearing loss.Reference Usami, Kitoh, Moteki, Nishio, Kitano and Kobayashi3 In that series, the second most common cause of hearing loss was cytomegalovirus infection, diagnosed by polymerase chain reaction of umbilical blood in 13 per cent of cases.Reference Usami, Kitoh, Moteki, Nishio, Kitano and Kobayashi3 Clemmens et al. reported a prevalence of cochlear nerve deficiency of 26 per cent in children with unilateral SNHL, with a prevalence of 48 per cent in cases with severe-to-profound unilateral loss.Reference Clemmens, Guidi, Caroff, Cohn, Brant and Laury4 Nakano et al. reported a prevalence of cochlear nerve deficiency of 50 per cent in a paediatric population with unilateral hearing loss, compared to 5 per cent in cases with bilateral SNHL.Reference Nakano, Arimoto and Matsunaga5
The importance of unilateral hearing loss in the paediatric population has been previously underestimated. It is now thought to result in poorer language performance and an increased likelihood of receiving speech therapy.Reference Lieu, Tye-Murray, Karzon and Piccirillo6 This study aimed to determine the prevalence of cochlear nerve hypoplasia or aplasia in an Australian paediatric population with unilateral or bilateral SNHL, and to discuss its implications with regard to cochlear implantation candidacy.
Materials and methods
Institutional ethics approval was obtained. The study was conducted in accordance with the Strengthening the Reporting of Observational studies in Epidemiology (‘STROBE’) guidelines. A retrospective case series was completed in Western Australia's only tertiary paediatric hospital, between January 2015 and January 2018.
The cases eligible for inclusion were paediatric patients referred for MRI scanning for the investigation of SNHL. At our institution, the criteria for requesting MRI scanning for bilateral hearing loss was a hearing loss of at least moderate severity. Magnetic resonance imaging to investigate single-sided deafness or unilateral hearing loss was performed in patients with moderate-to-profound hearing loss in one ear and with normal hearing (thresholds of less than or equal to 20 dB) in the contralateral ear.
The MRI scans were performed in 102 cases using a 1.5 Tesla Siemens Magnetom Sonata™ scanner and in 53 cases using a 3 Tesla Siemens Skyra™ scanner. The following sequences were obtained: axial T2-weighted, coronal fluid-attenuated inversion recovery (‘FLAIR’); sagittal (or volumetric at 3 Tesla) T1-weighted, axial T2-weighted high-resolution constructive interference in steady state (‘CISS’) (or sampling perfection with application-optimised contrasts using different flip angle evolution (‘SPACE’) at 3 Tesla) (0.7mm slice thickness), T2-weighted thin sagittal oblique through the right and left internal auditory canals (2mm slices); diffusion-weighted imaging, and apparent diffusion coefficient maps.
Imaging reports were reviewed to determine the findings. Specifically, details on the report outlining the anatomy of the primary data point – the cochlear nerve status – within the internal auditory canal and cerebellopontine angle, were documented. The cochlear nerve was deemed to be hypoplastic if its calibre on the affected side was less than that of the contralateral nerve. The nerve was deemed to be aplastic or absent if it was not visible on MRI. In addition, reported abnormalities within the cochlea, vestibular apparatus and brain were identified.
Patients were divided into two groups based upon the type of hearing loss. The first group had bilateral SNHL, and the second group had unilateral hearing loss or single-sided deafness. The MRI scan reports were compared between the two groups, specifically with regard to the primary data point of cochlear nerve status. Differences between the two groups were compared using an independent samples two-tailed t-test, assuming unequal variances between the two groups, with statistical significance defined as a p-value of less than 0.05.
Results
A total of 156 cases were identified as suitable for inclusion. The mean age of this final cohort at the time when MRI scanning was performed was 5.42 years (standard deviation (SD) = 5.1 years). Patients’ age ranged from 2 weeks to 16.5 years. Eighty-four patients had bilateral hearing loss, and 72 had asymmetric hearing loss or profound unilateral hearing loss.
Unilateral hearing loss
The mean age of this cohort was 6.22 years (SD = 5.32 years). Of the 72 patients with unilateral SNHL, 39 per cent (28 cases) had absent or hypoplastic cochlear nerves on the affected side. Fifteen per cent (11 cases) had other abnormal findings on MRI. The most common abnormal finding other than cochlear nerve dysplasia was an enlarged vestibular aqueduct (six cases). Other abnormal findings included an arachnoid cyst, pontomedullary infarction, parietal cortical ischaemic infarct, chiari malformation and posterior semi-circular canal aplasia (Table 1). The remaining 46 per cent of the group had a normal cochlea and cochlear nerve on MRI (Figure 1).

Fig. 1. The prevalence of cochlear nerve anomalies in: (a) unilateral hearing loss or single-sided deafness patients, and (b) bilateral hearing loss patients.
Table 1. Magnetic resonance imaging findings

*n = 72; †n = 84. SNHL = sensorineural hearing loss
Of the 28 patients who had hypoplastic or absent cochlear nerves, 25 per cent underwent a diagnostic MRI when aged under three months. The distribution of patient age at diagnosis is depicted in Table 2. An example of the imaging appearance of unilateral cochlear nerve absence is depicted in Figure 2.
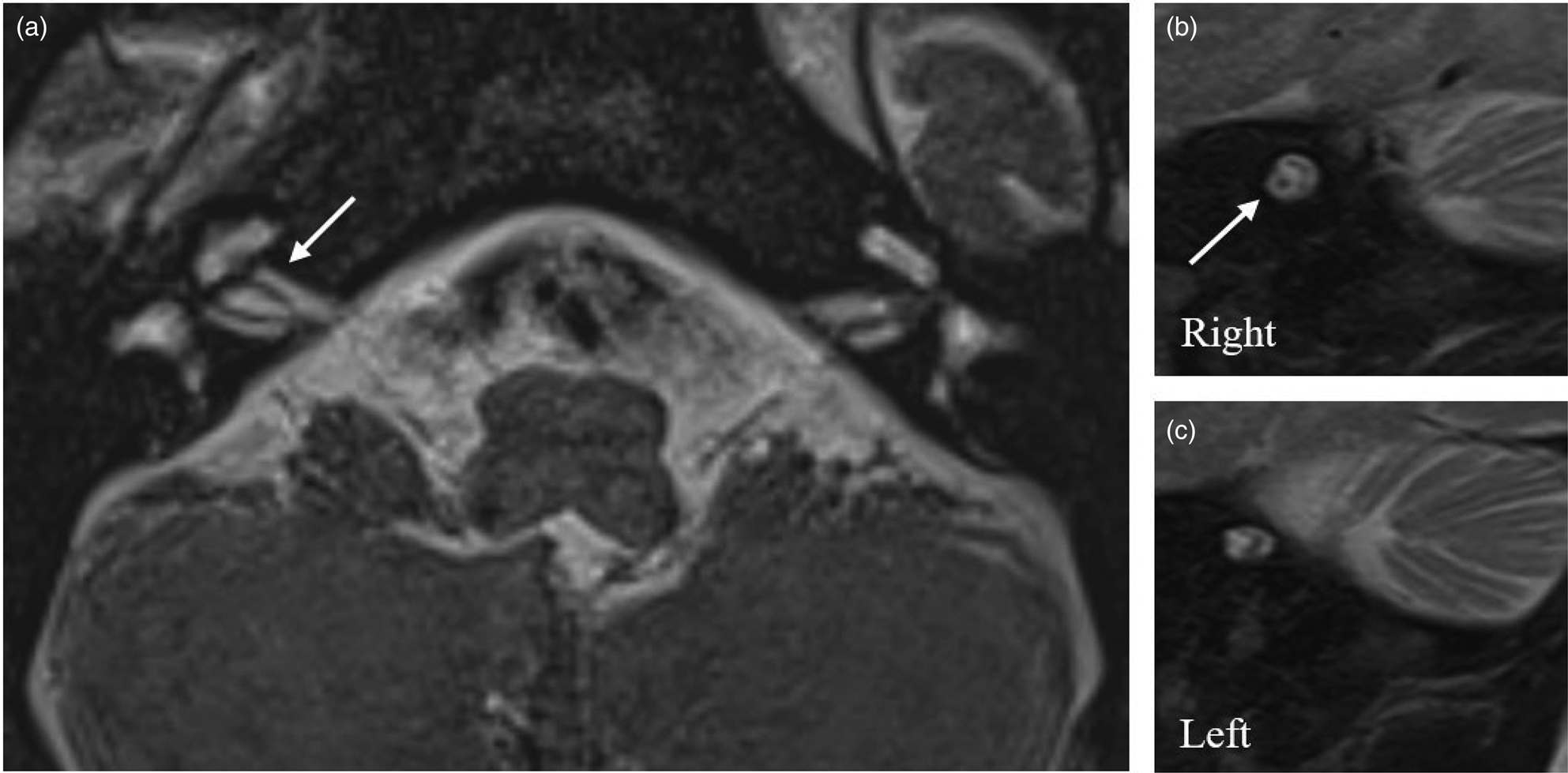
Fig. 2. (a) Axial and (b,c) oblique sagittal magnetic resonance imaging scans demonstrating aplastic left-sided cochlear nerve within a hypoplastic internal auditory canal. Arrows indicate the normal right-sided cochlear nerve.
Table 2. Distribution of age at diagnosis of cochlear nerve hypoplasia or aplasia, in unilateral SNHL patients

SNHL = sensorineural hearing loss
Bilateral sensorineural hearing loss
The mean age of this cohort was 4.74 years (SD = 4.8 years). There was no significant difference between the age of this group and that of the unilateral hearing loss group (p = 0.07).
In this cohort, 84 patients had bilateral SNHL; cochlear nerve hypoplasia or aplasia was identified only in 5 per cent (n = 4) of these cases. Other abnormal findings were identified in 14 per cent (12 cases); again, the most common abnormal finding was an enlarged vestibular aqueduct (5 cases). Other abnormalities included cortical haemorrhagic or ischaemic changes, diffuse parenchymal loss, hypoplastic superior semi-circular canal, and isolated vestibular dysplasia (Table 1).
Chi-square analysis of the primary statistic – cochlear nerve status – revealed a statistically significant difference between the two groups, indicating that cochlear nerve anomalies were more common in patients with unilateral hearing loss or single-sided deafness (χ2 = 29.6592, p < 00001).
Discussion
In our study, cochlear nerve hypoplasia or aplasia was present in 39 per cent of paediatric patients with unilateral hearing loss, which is in keeping with recently published international literature.Reference Usami, Kitoh, Moteki, Nishio, Kitano and Kobayashi3–Reference Nakano, Arimoto and Matsunaga5 This prevalence was statistically significantly greater than in patients with bilateral SNHL, where cochlear nerve abnormalities were identified in only 5 per cent of cases.
In this series, 25 per cent of patients with unilateral SNHL underwent MRI that diagnosed cochlear nerve hypoplasia, before three months of age. Around two-thirds of the patients underwent a diagnostic MRI before the age of two years.
There is a growing understanding of the impact of unilateral SNHL on a child's development. The primary deficit seems to be the lack of a binaural squelch effect and impaired hearing in noise, which affects classroom performance.Reference D'Alessandro, Sennaroğlu, Yücel, Belgin and Mancini7 Children aged between 6 and 18 years with untreated single-sided SNHL have lower intelligence quotients than their peers, with an average difference of 6.3 points.Reference Purcell, Shinn, Davis, Kathleen and Children8 Unilateral hearing loss has been associated with poorer language performance and increased utilisation of speech pathology services.Reference Lieu, Tye-Murray, Karzon and Piccirillo6,Reference Lieu9 Twenty-five per cent of these children will have behavioural and academic problems that extend into adolescence.Reference Fischer and Lieu10,Reference Bess and Tharpe11
Treatment of unilateral SNHL is time-critical to improve a child's development, because there is increasing evidence that time-sensitive irreversible cortical reorganisation is driven by the hearing ear and may result in a delayed implant in the deaf ear not being beneficial.Reference Gordon, Wong and Papsin12,Reference Gilley, Sharma and Dorman13 Currently available treatment strategies for single-sided deafness include conventional hearing aids, contralateral routing of signal (‘CROS’) hearing aids and bone conduction implants. A recent systematic review by Van Zon et al. showed no significant benefit of contralateral routing of signal devices and bone conduction implants on speech perception in noise or localisation in adult patients with single-sided deafness, although there was subjective improvement reported.Reference Van Zon, Peters, Stegeman, Smit and Grolman14 There are obvious limitations to comparing adult patients to paediatric patients with single-sided deafness.
In recent years, the indications for cochlear implantation in adults and children have broadened. In the first systematic review of cochlear implantation for single-sided deafness, by Peters et al., in 2015, no randomised, controlled trials were identified. Examination of the best available evidence suggested that cochlear implantation has a beneficial effect on sound localisation, quality of life and tinnitus.Reference Peters, Smit, Stegeman and Grolman15
Given the limitations of other hearing rehabilitative options, cochlear implantation has become an emerging treatment for children with unilateral SNHL, with positive reports of early outcome measures. Polonenko et al. reported restoration of bilateral auditory input to the cortex following cochlear implantation in five children with single-sided deafness.Reference Polonenko, Gordon, Cushing and Papsin16 In a series of 21 children with congenital single-sided deafness, who were implanted between the ages of 10 months and 11 years, improvements in combined head shadow effect, squelch effect and summation effect, and lateralisation ability, were demonstrated.Reference Thomas, Neumann and Dazert17
However, despite the benefit of unilateral cochlear implantation, its success is predicated upon the assumption that the cochlear nerve and retrocochlear pathways are intact. Up to half of patients with unilateral hearing loss will have an absent or hypoplastic cochlear nerve, necessitating important consideration prior to offering cochlear implantation as a hearing restoration option.
Warren et al. reported a case series of three patients with bilateral SNHL (with at least severe hearing loss in the better hearing ear) and no cochlear nerve evident on MRI, who underwent successful cochlear implantation. These patients demonstrated responses to auditory stimuli and improvement on audiological testing post-operatively. All patients were using their cochlear implant at the time of publication.Reference Gordon, Wong and Papsin12
An Australian study of children with cochlear nerve hypoplasia or aplasia, with bilateral severe-to-profound hearing loss, who underwent implantation, demonstrated Categories of Auditory Performance scores for 59 implanted ears. Forty-seven per cent of ears with cochlear nerve aplasia and 89 per cent of ears with cochlear nerve hypoplasia achieved scores of 5 to 7 (consistent with some verbal understanding).Reference Birman, Powell, Gibson and Elliott18 This suggests that despite the absence of a visible cochlear nerve, auditory fibres may follow an alternate pathway or the cochlear nerve may be too small to visualise. The results of this study are encouraging, but there are limitations to applying cochlear implant results in children with bilateral hearing loss to children with single-sided deafness. The contribution of implantation to speech and language will be very different in children with a normal contralateral ear compared to children with no contralateral aural input.
• More than half of children with unilateral sensorineural hearing loss (SNHL) are not diagnosed on newborn hearing screening
• Cochlear nerve hypoplasia or aplasia, diagnosed with magnetic resonance imaging, is an increasingly recognised cause of paediatric SNHL
• In this series, 39 per cent of patients with unilateral SNHL had absent or hypoplastic cochlear nerves on the affected side
Despite these early and promising studies, further research is needed to determine if cochlear implantation is a viable option for all patients with unilateral hearing loss secondary to cochlear nerve aplasia or hypoplasia.
Conclusion
Paediatric patients with unilateral SNHL are more likely to have cochlear nerve anomalies than those with bilateral SNHL. Further studies are required to determine whether cochlear implantation or other hearing rehabilitative options are best suited to managing this increasingly recognised pathology.
Competing interests
None declared




