


INTRODUCTION
Cognitive impairment is common in Multiple Sclerosis (MS), occurs at all disease stages and can be a primary source of social dysfunction, occupational disability and diminished quality of life (Rodgers & Panegyres, Reference Rogers and Panegyres2007). Estimated prevalence of cognitive impairment in people with MS (PwMS) ranges between 43% and 65% (Denney, Sworowski, & Lynch, Reference Denney, Sworowski and Lynch2005) typically involving difficulty with attention, memory, information processing speed, and executive functions (Goretti et al., Reference Goretti, Niccolai, Hakiki, Sturchio, Falautano, Minacapelli and Amato2014; Whelan et al., Reference Whelan, Lonergan, Kiiski, Nolan, Kinsella, Hutchison and Reilly2010).
Balance and gait difficulties and associated risk of falling in PwMS are well documented (Cattaneo et al., Reference Cattaneo, De Nuzzo, Fascia, Macalli, Pisoni and Cardini2002; Leone, Patti, & Feys, Reference Leone, Patti and Feys2015). Postural control has been defined as, “the control of the body’s position in space for the purposes of balance and orientation” (Shumway-Cook & Woolacott, Reference Shumway-Cook and Woolacott2000). Where balance is impaired, greater attention allocation may be required to maintain effective stability. Conventionally, it has been considered a reflex or automatic controlled task, with the implication that minimal attentional resource is used by postural control systems (Woolacott & Shumway-Cook, Reference Woollacott and Shumway-Cook2002). Recent research contradicts this hypothesis, suggesting there are substantial attentional requirements for postural control (Donker, Roerdink, Greven, & Beek, Reference Donker, Roerdink, Greven and Beek2007; Yogev-Seligmann, Hausdorff, & Giladi, Reference Yogev-Seligmann, Hausdorff and Giladi2008).
Poor postural control contributes to increased risk of falling for PwMS (Cameron & Lord, Reference Cameron and Lord2010; Cattaneo et al., Reference Cattaneo, De Nuzzo, Fascia, Macalli, Pisoni and Cardini2002). Dual-task designs, where participants perform cognitive and motor tasks concurrently, have been used to investigate the interaction of cognitive and motor functioning in relation to both gait and postural stability. In relation to gait, Hamilton et al. (Reference Hamilton, Rochester, Paul, Rafferty, O’Leary and Evans2009) found evidence that PwMS show disproportionately larger decrements in gait performance compared to controls under dual task conditions and several other studies have found similar results (see Leone et al., Reference Leone, Patti and Feys2015).
A relatively small number of studies have examined dual tasking in relation to balance in the context of cognitive tasks (e.g., Boes et al., Reference Boes, Sosnoff, Socie, Sandroff, Pula and Motl2012; Kalron, Dvir, & Achiron, Reference Kalron, Dvir and Achiron2010, Reference Kalron, Dvir and Achiron2011; Negahban et al., Reference Negahban, Mofateh, Arastoo, Mazaheri, Yazdi, Salavati and Majdinasab2011; Wajda, Motl, and Sosnoff, Reference Wajda, Motl and Sosnoff2014). Prosperini et al. (Reference Prosperini, Castelli, Sellitto, De Luca, De Giglio, Gurreri and Pozzilli2015) note that among the studies examining postural control under dual-task conditions some have not calculated a dual-task decrement measure (meaning that the specific effect of dual-tasking compared to single-task performance could not be discerned); some have not included a control group (so the question of whether any dual-task decrements are disproportionate in people with MS cannot be addressed); and conflicting results regarding factors such as disability level and fatigue on performance have been found.
In studies conducted by Prosperini and colleagues, they found that people with MS showed a greater dual-task decrement in postural control compared to controls (Prosperini et al., Reference Prosperini, Castelli, Sellitto, De Luca, De Giglio, Gurreri and Pozzilli2015), although this was only apparent when the secondary cognitive task was a test of executive function involving discriminating conflicting stimuli (Stroop) and not a test of word generation (category fluency) or speed of information processing (Symbol Digit Modalities Test) (Prosperini et al., Reference Prosperini, Castelli, De Luca, Fabiano, De Giglio, Gurreri and Pozzilli2016). They also reported that dual-task costs were associated with quality of life in terms of role limitations due to physical problems and social functioning (Castelli et al., Reference Castelli, De Luca, Marchetti, Sellitto, Fanelli and Prosperini2016).
Given the finding of greater dual-task cost for PwMS on the Stroop, it would be useful to examine other tests of executive function to support the claim that tests of executive function may be the most suitable for revealing a disproportionate dual-task decrement in balance for PwMS. The findings of Castelli et al. regarding potential association with quality of life (QoL) related to general aspects of QoL, and it would be good to examine whether measures of dual-task decrement relate to more specific aspects of dual-tasking in everyday life.
Finally, none of the three studies of Prosperini and colleagues examined the potential effect of anxiety on performance. When comparing a patient and control group it is important to examine for potential confounding differences (e.g., age, gender, education) when using measures of cognition. But in addition, to better understand the mechanisms that might cause, or moderate, dual-tasking difficulties, it is important to examine factors that might be expected to differ between groups (e.g., PwMS are more likely to report fatigue than controls) and influence level of dual-task performance. One such factor is mood. Estimated prevalence rates for depression range from 10% to 41.8%; anxiety 23.5% to 41%, which are considerably higher than in the general population (Wood et al., Reference Wood, van der Mei, Ponsonby, Pittas, Quinn, Dwyer and Taylor2012). Given the effects of anxiety/depression on cognition it may be that mood significantly affects the ability to dual-task in PwMS, but this has not been systematically examined to date.
Previous studies have used stable flat surfaces for the balance tasks, but everyday life requires people to stand, and walk on, a range of surfaces. Balancing on uneven/unstable surfaces may be particularly challenging under dual-task conditions; therefore, it would be useful to investigate whether dual-task decrements are greater on unstable compared to stable surfaces.
The present study compared the performance of a group of people with Relapsing Remitting MS and a well-matched group of healthy controls on a balance task and an executive (working memory) task (Backward Digit Span) under both single- and dual-task conditions, on both stable and unstable surfaces. The relationship between level of dual-task decrement and everyday dual-task functioning, measured by scores on a self-report questionnaire the Dual-Task Questionnaire (DTQ; Evans, Greenfield, Wilson, & Bateman, Reference Evans, Greenfield, Wilson and Bateman2009) was examined. We hypothesized that PwMS would show a greater dual-task decrement than healthy controls on both stable and unstable surfaces and that there would be a relationship between level of dual-task decrement and level of difficulty with everyday dual-tasks. Finally, the relationship between disease severity [Expanded Disability Status Scale (EDSS) score], fatigue, and mood (anxiety/depression) and dual-task performance was examined.
METHODS
Participants
In their study of gait under dual-task conditions, Hamilton et al. (Reference Hamilton, Rochester, Paul, Rafferty, O’Leary and Evans2009) found medium–large effect sizes for several dual-task decrement measures (ranging from d=0.7 to d=1.5). In the present study, we took several approaches to try to maximize effect sizes, such as inclusion of a wider range of disability levels of MS participants and use of a Backward Digit Span task, which is more challenging than the previously used forward digit span tasks. However, given that the nature of the motor task was different from that used by Hamilton et al, we took a conservative approach and powered the proposed study on the basis of the lower of their effect sizes (d=0.7; r=−.33). Using G*Power 3.1 (Faul, Erdfelder, Buchner, & Lang, Reference Faul, Erdfelder, Buchner and Lang2009), with power set at 0.8, alpha at 0.05 (two-tailed), d=0.7, a minimum of 34 participants per group was required.
Thirty-five RRMS participants were recruited through NHS Highland Neuropsychology, Neurology, MS Nurses, and MS Therapy Centre services. Inclusion criteria for RRMS participants were: (i) diagnosis of RRMS, (ii) age between 17 and 65 years, (iii) free of relapse 30 days before task administration, (iv) an EDSS score up to 6.5 (Multiple Sclerosis Trust, 2013), (v) capacity to consent. A Consultant Neurologist confirmed diagnosis and EDSS score based on standardized investigation and in alignment with the revised McDonald diagnostic criteria (Polman et al., Reference Polman, Reingold, Banwell, Clanet, Cohen, Filippi and Wolinsky2010). The 34 control participants were a convenience sample of family of MS participants and volunteers recruited through poster advertisement in local hospitals. Volunteers were accepted as control participants if they matched an RRMS participant by age and gender. Exclusion criteria for all participants were: (i) presence of major psychiatric disorders, (ii) history of neurodegenerative disease (other than MS for the patient group) or brain injury, (iii) significant sensory deficits, (iv) severe co-morbid health condition affecting motor abilities, and (v) inability to stand.
Ethical approval was obtained from NRES Committee East Midlands– Nottingham 2. NHS Highland Research and Development Department granted management approval. Participation in the study was voluntary and participants provided written informed consent.
Measures
Demographic information was collected from all participants and in addition for RRMS participants, disease onset, years of illness, and EDSS score.
BACKGROUND ASSESSMENT
Hospital Anxiety and Depression Scale (All Participants)
Anxiety and depression were screened using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, Reference Zigmond and Snaith1983). This self-report measure was designed for use with non-psychiatric hospital patients. The HADS reliability and validity has been described as good to very good with internal consistency coefficients of 0.8, concurrent validity of 0.6–0.8 and both specificity and sensitivity of 0.8 (Bjelland, Dahl, Haug, & Neckelmann, Reference Bjelland, Dahl, Haug and Neckelmann2002). An exclusion criterion of this study was the presence of major psychiatric disorders. The authors of the HADS recommend that, for depression and anxiety scales alike, raw scores of 8–10 identify mild cases, 11–15 moderate, and 16+ severe (Zigmond & Snaith, Reference Zigmond and Snaith1983). Therefore, if participants scored 16+ on anxiety or depression items they would be excluded from the study.
Modified Fatigue Impact Scale (All Participants)
The Modified Fatigue Impact Scale (MFIS) (MSCCP, 1998) is a 21-item self-report measure and was used to assess fatigue. Score range is 0–84. It includes physical, cognitive, and psychosocial subscales. It is a recommended measure of fatigue in MS (MSCCP, 1998) with good reliability and validity. It has an intra-class correlation coefficient of 0.91, internal consistency coefficient of 0.92, and a convergent validity coefficient of 0.67 (Kos et al., Reference Kos, Kerchofs, Carrea, Verza, Ramos and Jansa2005).
Multiple Sclerosis Impact Scale (RRMS Participants Only)
The Multiple Sclerosis Impact Scale (MSIS-29) (Hobart, Lamping, Fitzpatrick, Riazi, & Thompson, Reference Hobart, Lamping, Fitzpatrick, Riazi and Thompson2001) is a 29-item self-report measure and was used to assess quality of life in PwRRMS. Responses options range from 1 “not at all” to 5 “extremely”. Score range is 29–145. It has good variability, small floor and ceiling effects, high intra-class correlation coefficient of 0.87, and high internal consistency coefficients of 0.91 (Hobart et al., Reference Hobart, Lamping, Fitzpatrick, Riazi and Thompson2001).
Dual-Tasking Questionnaire (All Participants)
The 10-item Dual-Tasking Questionnaire (DTQ; Evans et al., Reference Evans, Greenfield, Wilson and Bateman2009) was used to measure self-reported ability to divided attention. This questionnaire asks PwMS to rate how often they experience certain dual-task difficulties in day-to-day life. There are five response options ranging from very often to never, or not applicable. Score range is 0–40. Evans et al. (Reference Evans, Greenfield, Wilson and Bateman2009) reported a test–retest correlation of 0.690 (p<.04) in a group of people with dual-tasking difficulties after brain injury, with indications that the DTQ was sensitive to the effect of a treatment intervention aimed at improving dual-task performance. Evans et al. (Reference Evans, Cullen, Paul, Frei, Norrie and O’Leary2014) found a significant difference between PwRRMS and controls on the DTQ and that the DTQ correlated with measures of dual task decrement on a task that combined walking with digit span.
Test of Premorbid Function (All Participants)
Premorbid intellectual functioning was assessed using the Test of Premorbid Function (TOPF; Wechsler, Reference Wechsler2011). Score range is 0–70. It has a high level of internal reliability (0.95) and high test–retest stability (correlations ranging from 0.89–0.95) (Pearson Education Ltd, 2010).
Addenbrooke’s Cognitive Examination (All Participants)
The Addenbrooke’s Cognitive Examination (ACE-III; Hsieh, Schubert, Hoon, Mioshi, & Hodges, Reference Hsieh, Schubert, Hoon, Mioshi and Hodges2013), a short cognitive test designed to screen for dementia, was used to assess general cognition. It has not been extensively validated in MS, but in the study by Hamilton et al. (Reference Hamilton, Rochester, Paul, Rafferty, O’Leary and Evans2009), it showed a significant difference between PwRRMS and matched controls, suggesting it was sensitive to cognitive impairment in MS. Here, the ACE-III was used primarily as a screen to check participants were not severely cognitively impaired. The test minimum and maximum scores are 0 and 100, respectively. Sensitivity is reported to be 0.94, and specificity is 0.89 for the optimal cutoff (88/100) in relation to distinguishing people with dementia from controls (Hodges, Reference Hodges2007).
Cortical Vision Screening Test (All Participants)
The Cortical Vision Screening Test (CORVIST; James, Plant, & Warrington, Reference James, Plant and Warrington2001) is a 10-subtest measure that was used to assess visuoperceptual ability. Each subtest measures a different aspect of visual processing and identifies cortical based visual problems. Score range is 0–98. The CORVIST was used to ensure participants did not have significant visual impairment.
Backward Digit Span (All Participants)
Individual digit span assessments were completed based on Backward Digit Span, a method developed by Cocchini et al. (Reference Cocchini, Della Sala, Logie, Pagani, Sacco and Spinnler2004). Participants heard digit lists at a rate of one per second and were asked to repeat these back in reverse order. Initial span length was two-digits and participants were presented with six sequences at each span length. If five of six digits were accurately recalled, the digit sequence was lengthened by one digit. Individual digit span was determined as the last sequence length at which five of six responses were correct. Individual digit span was identified during the baseline assessment. Established individual span length was then used during single- and dual-task conditions.
BALANCE TASKS
BioSway (All Participants)
Postural stability was measured using the BioSway (Biodex, 2015), a flexible balance assessment device. It measures neuromuscular control and capability to balance on firm and unstable surfaces. Sensors embedded in a platform (21.25” wide×19.00” long×2.56” high) produce an Anterior/Posterior Stability Score (APSS), a Medial/Lateral Stability Score (MLSS) and a person’s Overall Stability Index (OSI). These indexes are standard deviations assessing movement of the person’s center of pressure around the central point. The OSI is a composite of the MLSS and APSI and was the primary stability score used in this study. It has good reliability with an intra-class correlation coefficient of 0.81 (Biodex, 2015).
Measuring center of pressure and its displacement has been found to be a reliable method of balance assessment during dual task static standing balance assessments (Yang, Liao, Lam, He, & Pang, Reference Yang, Liao, Lam, He and Pang2015). The Biosway has been used in several clinical studies in both MS (e.g., Ozkan, Guclu-Gunduz & Irek, Reference Ozkan, Guclu-Gunduz and Irek2015) and other neruological conditions (e.g., Suh et al., Reference Suh, Han, Jeon, Kim, Lee, Yoon and Chong2014) and has been used as the gold standard measurement of balance in MS from which the validity of other clinical measures can be calculated, for example, MiniBEST (Aydin et al., Reference Aydin, Irek, Guclu-Gunduz, Ozkan, Yazici, Ozkul and Batur-Caglayan2015).
During the four balance tasks participants stood barefoot on the BioSway with eyes open and hands by their sides. To ensure measurement of normal balance, if a participant used a walking aid to balance day-to-day they were asked to use this aid while undertaking all study-related balance tasks. Participants stood with their feet in a comfortable positon. This foot position was recorded before task commencement and the same foot position was used for each task. Participants stood on a stable surface during tasks 2 and 4 and an unstable (foam) surface for tasks 3 and 5. The unstable condition included to assess dual-task ability under more challenging conditions. They were instructed to focus on maintaining their balance throughout single-task conditions and to simultaneously focus on holding balance and saying aloud, in reverse order, numbers heard during dual-task conditions. OSI scores were calculated under single- and dual-task conditions and dual-task decrement score calculated in terms of percentage change from single- to dual-task conditions.
COGNITIVE TASK
During one single- and two dual-task conditions, participants listened to sequences of digits at their individualized digit span length. Pre-recorded digit sequences were played aloud and participants were to repeat each sequence in reverse order. Responses were recorded manually. Scores were calculated by allocating one point for each digit in the correct place in a sequence. The total correct was then calculated. To obtain percentage correct scores, the total score was divided by the total possible correct score and multiplied by 100.
Procedure
Recruiters were given study information before recruiting so they knew inclusion/exclusion criteria. At routine appointments, PwRRMS who met study criteria were informed about the study by their clinician or MS Therapy Centre Manager. Those who expressed an interest were given the participant information sheet. If consent and contact information was provided, after 24 hr, the researcher contacted potential participants by telephone to provide further information regarding the study and answer any questions. Control participants contacted the researcher using contact details on the poster. If verbal consent was given, arrangements were made to meet. Written consent was obtained at the face-to-face appointment.
All participants completed baseline assessment measures as previously described. Subsequently, all participants undertook three single- and two dual-tasks. Task 1 required participants to complete a titrated Backward Digit Span task. Task 2 involved participants standing on the BioSway platform, stable surface, for a total of 80 s with a 15-s break half way. Task 3 involved participants standing on the BioSway platform, unstable surface, for 80 s with a 15-s rest half way. For Task 4, participants stood on the BioSway platform, stable surface, while simultaneously completing the Backward Digit Span task. Task 5 required participants to stand on the BioSway platform, unstable surface, while completing the Backward Digit Span task.
To ensure consistency of delivery, instructions for balance tasks were pre-produced by the researcher and instructions for digit span were based on the Backward Digit Span subtest in the WAIS-IV (Pearson Education Ltd, 2008). To control for order effect, task order was randomly assigned. A simple function in Excel was used to produce different combinations of 1–5 to ensure that the 68 participants completed the three single- and two dual-tasks in a different order from one another.
Data Analysis
Distributions of all variables were examined for normality. All scores apart from age and DTQ were not normally distributed. Where appropriate, a parametric approach was used and a non-parametric approach was adopted for all other scores. Descriptive statistics were produced to describe the data. Independent samples t tests and Mann-Whitney U tests were used as appropriate to compare groups on demographic information, baseline clinical features, and on single-task and dual-task performance. Using Mann-Whitney U Test, measures of dual-task decrement (for balance and digit span tasks) were compared for both groups.
Spearman correlations were used to examine whether there was a relationship between DTQ scores and individual dual-task decrement scores. Spearman correlation coefficients (rho) were used, first, to explore relationships between self-reported anxiety and depression and dual-task decrement scores and, second, to examine disease severity (EDSS score) and dual-task decrement scores in the MS group only.
To balance risk of type I and II errors, a Bonferroni correction was applied; the level of significance was reduced by the number of correlations calculated for each factor. More specifically, four different correlations were derived for each factor; therefore, the p-value was divided by four to reduce the likelihood of type I errors, whilst maintaining reasonable power. Therefore, the significance level became 0.0125 for these correlations. Field and Hole (Reference Field and Hole2003) recommend use of r as an effect size for non-parametric statistics and so all effect sizes were reported in terms of r for consistency.
RESULTS
Descriptive Characteristics
Data were collected for 35 RRMS and 34 control participants. One control participant was a genetic family member, two were spouses, and the remaining 31 were non-related. No participants were deemed unfit to participate in the study based on baseline assessment results. Data for one RRMS participant could not be used due to a leg tremor during balance testing. Data included in statistical analysis were, therefore, taken from 34 PwRRMS and 34 healthy control participants. Demographic and clinical characteristics of each group are outlined in Table 1.
Table 1 Participant demographic and clinical characteristics

Note. Values are mean±SD, median [lower–upper interquartile range] or n.
*Statistically significant difference for RRMS versus healthy control participants.
† p-Value for difference between RRMS versus healthy control participants.
There were no significant differences in age (t(df 66)=0.207), gender (χ2(df 1)=0.000), years of education (U=488.5; z=−1.101), estimated pre-morbid IQ (U=440; z=−1.695), or baseline digit span (U=493; z=−1.108) between the groups. A significant difference was found between groups for self-reported DTQ scores (t(df 66)=9.476; p<0.001; r=0.75); PwRRMS reported greater difficulty dual-tasking day-to-day compared to controls. The performance of PwRRMS was significantly poorer on the ACE-III compared to healthy controls (U=67; p<.001; z=−6.306; r=0.76). All 34 control subjects scored above the two clinical cutoffs compared to 25 RRMS participants. Five PwRRMS scored below the first cutoff (score of 88) and four scored below the second cutoff (score of 82). PwRRMS self-reported greater levels of fatigue (U=115; p<.001; z=−5.683; r=0.69), depression (U=211; p<.001; z=−4.543; r=0.55;), and anxiety (U=290.5; p<.001; z=−3.548; r= 0.43) compared to controls.
Performance Under Single- and Dual-Task Conditions
Data were analyzed to establish performance on digit span and balance tasks under single- and dual-task conditions. Significant differences were found between groups on all digit span tasks (single-task: U=330; z=−3.236; p<.001; r=0.39; dual-task stable: U=210; z=−4.596; p<.001; r=0.56; dual-task unstable: U=50; z=−6.536; p<.001; r=0.79). Significant differences were also found between groups on all balance tasks (single stable: U=204; z=−4.683; p<.001; r=0.57; single unstable: U=159; z=−5.189; p<.001; r=0.63; dual-task stable: U=269; z=−3.828; p<.001;, r=−0.46; dual-task unstable: U=101; z=−5.888; p<.001; r=0.71). Table 2 and Figure 1 summarize RRMS and control participant performance on all single- and dual-tasks.

Fig. 1 RRMS and control participant median performance on all single- and dual-tasks.
Table 2 RRMS and control participant performance on all single- and dual-tasks

Note. Values are median [lower–upper interquartile range].
** p-Value for difference between RRMS versus healthy control participants.
*Statistically significant difference for RRMS versus healthy control participants.
a Effect size (r) of difference between RRMS and controls.
OSI, Overall Stability Index; %C, percentage correct.
DUAL-TASK DECREMENT
 $${\rm Percentage}\,{\rm of}\,{\rm change}\,{\rm task}\,{\rm A{\equals}}{{{\rm Single{\hbox -}Task}\,{\minus}\,{\rm Dual}\,{\rm task}\,{\rm A}} \over {{\rm Single{\hbox -}Task}\,{\rm A}}}{\rm {\times}100}$$
$${\rm Percentage}\,{\rm of}\,{\rm change}\,{\rm task}\,{\rm A{\equals}}{{{\rm Single{\hbox -}Task}\,{\minus}\,{\rm Dual}\,{\rm task}\,{\rm A}} \over {{\rm Single{\hbox -}Task}\,{\rm A}}}{\rm {\times}100}$$
The formula of Baddeley et al. (Reference Baddeley, Della Sala, Gray, Papagno and Spinnler1997) was used to calculate percentage change (decrement) in performance from single- to dual-task conditions. Percentage changes (decrements) in performance from single- to dual-task conditions are outlined in Table 3 and Figure 2.
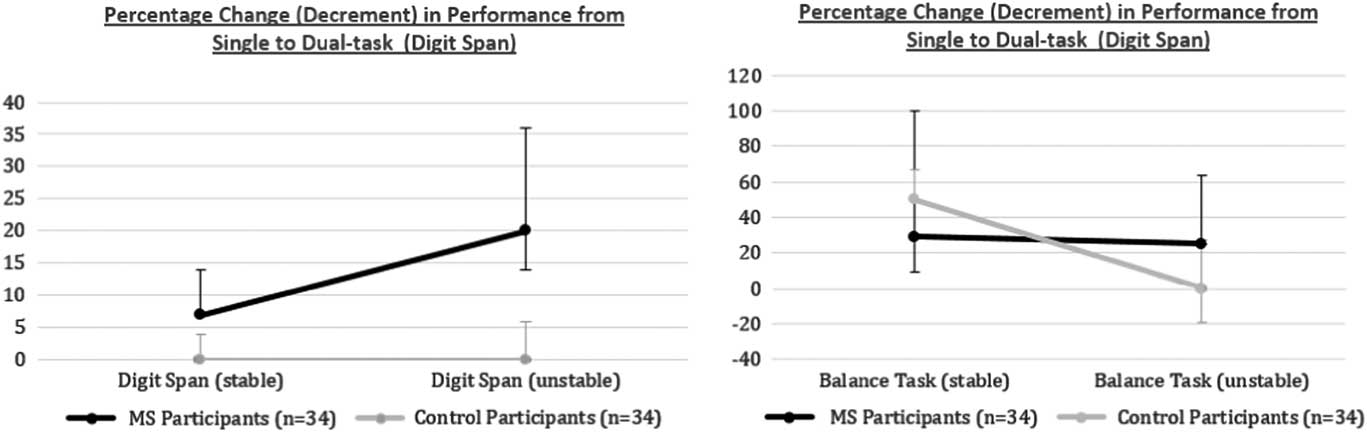
Fig. 2 Percentage change (decrement) in performance from single- to dual-task.
Table 3 Percentage change (decrement) in performance from single to dual-task

Note. Values are median [lower–upper interquartile range].
** p-Value for difference between RRMS versus healthy control participants.
*Statistically significant difference for RRMS versus healthy control participants.
a Effect size (r) of difference between RRMS and controls.
Digit Span Performance
Statistically significant differences were found between RRMS and control participants in digit span performance decrement in stable (z=−3.417; p<.001 two-tailed; r=0.41) and unstable (z=−6.556; p<.001 two-tailed; r=0.80) dual-task conditions. In the stable dual-task condition, RRMS participants’ performance decreased by 7% compared to 0% for controls. In the unstable dual-task condition, performance decreased by 20% in the RRMS group compared to 0% in the control group.
Balance Task Performance
Statistically significant differences were found between RRMS and control groups in balance task performance decrement in unstable (z=−2.715; p=.007 two-tailed; r=0.33), but not stable (z=−0.413; p=.679 two-tailed; r=0.05) dual-task conditions. A medium–large effect size was found for the unstable condition with overall stability decreasing by 25% in the RRMS group compared to 0% in the control group. No effect was found for the stable condition with RRMS overall stability decreased by 29% compared to 50% for controls.
Correlational Analysis
The relation between a measure of everyday dual-tasking (DTQ), fatigue (MFIS), a cognitive screening measure (ACE-III), and decrement scores for digit span and balance tasks were explored. The results are outlined in Table 4. No significant correlations were found between self-reported DTQ scores, self-reported MFIS scores, ACE-III scores, and decrement scores under any of the dual-task conditions.
Table 4 Correlation between measure of divided attention (DTQ), fatigue (MFIS), a cognitive screen (ACE-III), and decrement scores

Note. Values are Spearman’s rho and p-value.
*Statistically significant correlation.
The relation between disability status (EDSS), levels of anxiety and depression (HADS), and decrement scores were also explored. The results are outlined in Table 5. No significant correlations were found between EDSS and decrement scores under any of the dual-task conditions. Stable surface balance decrement scores were significantly correlated with levels of anxiety (rho=0.527; p=.001), depression (rho=0.451; p=.007), and HADS total (rho=0.539; p=.001) for the RRMS group, but not the controls.
Table 5 Correlation between measure of disability status (EDSS), levels of anxiety and depression (HADS), and decrement scores

Note. Values are Spearman’s rho and p-value.
*Correlation is significant at the .01 level (two-tailed).
To investigate the interaction between group and HADS scores in relation to decrement in balance on the stable surface, a regression model was examined. In the model, the dependent variable was the decrement in balance on the stable surface. As the balance decrement scores were not normally distributed, scores were transformed using a Box-Cox power transformation. Independent variables were: Group (RRMS vs. Control), HADS Total, and an interaction term (Group×HADS Total). As HADS Anxiety and Depression scores were significantly correlated (r=0.806), a combined HADS Total score was used. As HADS Total and the interaction term were highly correlated, to reduce multicollinearity problems, the HADS total score was mean-centered. A significant regression equation was found: F(3,64)=4.083; p=.01, with an adjusted R2 of 0.121. In this model only the Group×HADS interaction was significant (Beta−.558; p=.007). Figure 3 illustrates the interaction with a plot of decrement scores against HADS Total for each group, with associated regression lines. Models using HADS Anxiety and Depression scores separately were also developed and both produced similar, significant results for the interaction term in each model.

Fig. 3 Graph illustrating the relationship between HADS Total score and dual-task decrement for the RRMS and Control groups with associated regression lines.
DISCUSSION
A main finding of the study was that PwRRMS show a greater decrement under dual-task conditions compared to single conditions on measures of balance, digit span, and combined decrement scores when compared with controls. However, with regard to balance, a significantly greater decrement was not found in the stable dual-task condition. Where statistically significant differences were found, effect sizes were medium–large. The finding of greater decrement on the balance task for PwRRMS compared to controls is consistent with the recent studies of Prosperini and colleagues (Reference Prosperini, Castelli, Sellitto, De Luca, De Giglio, Gurreri and Pozzilli2015, 2016). However, the effect sizes relating to the differences between groups in terms of dual-task decrement on the balance measure were considerably larger in our study (medium–large) compared to the effect sizes in the Prosperini studies (small–medium).
Furthermore, we found significant differences in dual-task decrement on the cognitive task as well as the balance task, which was not apparent in the studies by Prosperini et al. It may be, therefore, that the Backward Digit Span task makes even more demand on the executive processes that are also required for maintaining balance. Another potential explanation is that on the studies by Prosperini et al., participants were instructed to prioritize the cognitive task under dual-task conditions, whereas in our study no specific instructions regarding prioritizing any particular task were given.
On the stable balance condition, the percentage change in performance from single- to dual-task conditions was higher in the control group (50%) compared to the RRMS group (29%), although this was not significant. One reason for the higher percentage change in the controls is that they had very good balance, that is, a low baseline OSI level, so relatively modest changes (i.e., similar absolute level to those of the MS group), represent a higher percentage change.
We examined the difference between groups using just the raw change scores (Dual OSI – Single OSI), but once again, there was no difference between the groups in the Stable condition. Somewhat anomalously, the median OSI scores were the same for controls and PwRRMS in both single stable and dual stable conditions, despite the median change scores being 50% and 29%, respectively. This results from the skewed distributions, and the difference in distributions of absolute scores and percentage change scores.
Two theoretical explanations have been proposed to account for the observed dual-task decrements in performance: the capacity model and the bottleneck model (Leone et al., Reference Leone, Patti and Feys2015). The capacity model proposes that the amount of cognitive resources available has a limit. Tasks are, therefore, completed within the capacity limits of those resources and dual-task decrements are apparent when the demands are greater than the resources. When a cognitive task is added to a demanding motor task, the system is overloaded and decrements occur. The question for this study though is why PwRRMS show greater decrements than controls. The cognitive task was titrated to individualized levels and so should have been requiring equal resources (unless we hypothesize that, due to working memory capacity being reduced in MS, the MS group require greater cognitive resources to produce a similar level of performance to that of the controls). For the motor task, however, it may be argued that this was more difficult for the MS group, given their performance under single- task conditions was poorer than controls. Therefore, if this task is demanding a much higher level of cognitive resource, when a secondary cognitive task is added, the attentional capacity may be compromised to a greater extent than for controls.
The bottleneck model suggests that decrements in dual-tasking occur due to both tasks attempting to use the same neuronal resources. There is some evidence from fMRI studies that working memory, spatial attention, and locomotive tasks use similar neuronal resources (LaBar, Gitelman, Parrish, & Mesulam, Reference LaBar, Gitelman, Parrish and Mesulam1999; Malouin, Richards, Jackson, Dumas, & Doyon, Reference Malouin, Richards, Jackson, Dumas and Doyon2003). In the present study, although the digit span task is a verbal task, so potentially not drawing on visual/motor system resources, some participants self-reported mentally visualizing digit sequences as they heard them and reading them backward, using the visual representation as a memory aid. This spatial aspect of digit span, combined with the visual feedback component of the balance task, suggests that shared neuronal resources were being used and if the capacity of these shared resources is reduced in MS, then this may have resulted in a disproportionate decrement under dual-task conditions.
Another potential explanation is that, in MS, there may be a central difficulty with dividing attention (even on tasks that are not making greater demands than usual) and that this makes it more difficult to efficiently allocate attention to two tasks simultaneously.
In the present study, although the most likely explanation for the disproportionate decrements for PwRRMS is the capacity model, some combination of all three potential explanations cannot be ruled out, something that could be explored in future research.
Factors Affecting Dual-Tasking
Stable surface balance decrement scores were significantly associated with levels of anxiety and depression in PwRRMS, but this relationship was not evident on the unstable surface. Effect sizes were medium–large. Regression analysis demonstrated that mood (anxiety/depression) moderated the balance decrement scores on the stable surface, but only in the RRMS group. The findings suggest that adding a cognitive task does not have any greater effect on the balance of PwRRMS than it does on controls when on a stable surface, unless MS participants are experiencing higher levels of anxiety/depression, in which case balance begins to deteriorate.
On the unstable surface, there was a significant difference between PwRRMS and controls at a group level, but no association with anxiety/depression. Perhaps it is the case that difficulties with dual-tasking on the unstable surface are so great as a result of limited cognitive resources, that variations in anxiety/depression do not have any additional impact on a system that is already compromised. It is noteworthy that the HADS asks for ratings of anxiety/depression over the past week. It was possible that the tasks themselves induced anxiety, and this situational anxiety may not have been related to the HADS score, but nevertheless impacted on dual-task performance. Future studies could measure situational anxiety and examine its impact on decrement.
A previous relationship between postural stability and anxiety has been shown in different clinical groups. For example, Matsuura and colleagues (Reference Matsuura, Fujino, Hashimoto, Yasuda, Yamamori, Ohi and Imura2015) assessed postural instability in patients with schizophrenia and control subjects, finding that postural instability was exacerbated by anxiety in the patient group only. However, the precise nature of the relationship between anxiety and dual-task decrement remains unclear.
Given that some of the conducted correlations were not statistically significant, it is important to consider the possibility of chance findings. Although a relatively conservative approach to significance level was adopted, nevertheless, it is possible these were random errors.
Another factor that may contribute to dual-task decrement is significant cognitive impairment. The finding that 25/34 participants did not fall below ACE-III cutoff scores suggests that most of the sample was not grossly cognitively impaired, and there were no group-level differences in baseline Backward Digit Span. However, the ACE-III was unlikely to be sensitive to more subtle impairment in speed of information processing, and Prosperini et al. (Reference Prosperini, Castelli, Sellitto, De Luca, De Giglio, Gurreri and Pozzilli2015) found that performance on the Symbol Digit Modalities Test was associated with dual task decrement in PwMS. It would be interesting for future studies to examine this in more detail.
Dual-Tasking and Disease Severity
One may anticipate that dual-tasking performance may decrease as disability status increases. This effect has been found in previous studies (Boes et al., Reference Boes, Sosnoff, Socie, Sandroff, Pula and Motl2012). However, the present study found no association between disease severity and dual-task decrement scores. This lack of association was also found in other studies, such as Hamilton et al (Reference Hamilton, Rochester, Paul, Rafferty, O’Leary and Evans2009). A recent systematic review by Wajda and Sosnoff (Reference Wajda and Sosnoff2015) further highlighted the discrepancy in results regarding the association between decrement and disability status. They postulated that divergent methodologies might explain the differences.
Everyday Dual-Tasking
PwRRMS reported significantly higher levels of everyday dual-tasking difficulties compared to control subjects. However, no correlation was found between measures of dual-task decrement and scores on the DTQ Questionnaire. Seemingly a range of factors other than the impact of cognitively demanding tasks on balance are affecting functioning on the dual-tasks covered in this questionnaire. Alternatively, measures of dual-task decrement in this balance study and the gait related DTQ perhaps tap into different motor abilities. Future research should explore the relationship between balance and gait parameters in RRMS.
Day-to-Day and Clinical Implications
Results suggest that PwRRMS will have difficulties maintaining balance and performing cognitive tasks, when attempted simultaneously. Furthermore, results suggest that dual-tasking performance may decrease when PwRRMS have heightened levels of anxiety/depression in certain circumstances. These findings have consequences for everyday life where we commonly maintain our balance while concurrently attending to cognitive tasks, for example, standing having a conversation. A review by Cameron and Lord (Reference Cameron and Lord2010) highlighted that PwMS commonly fall, display a fear of falling, are at greater risk of sustaining fall-associated injuries, and have increased risk of fatal falls. They also found that impairments of balance are probable causes of falls in PwMS. Postural instability under day-to-day dual-tasking conditions may, therefore, increase the risk of falls in PwMS.
Explaining potential balance and cognitive dual-task difficulties and the associated impact of increased levels of anxiety/depression, may help to inform future clinical assessment and treatment planning. Present study findings propose that solely assessing balance may not translate to everyday balance ability, where additional tasks may need to be concurrently attended to. Assessing balance with and without a concurrent task maybe a more reliable way of measuring balance function abilities in clinical settings. The need to assess dual-task ability is further supported by the present study finding that dual-task decrement is not predicted by factors such as fatigue, disease severity, or general cognitive ability. Developing a clinical assessment that measures balance and cognitive performance under both single- and dual-task conditions would be ideal but may not be practical for some clinical settings. Moreover, including measures of anxiety/depression will be important in comprehensively assessing everyday dual-task difficulties in MS. Levels of anxiety/depression should also be considered when planning treatment of everyday dual-task difficulties; anxiety and mood management techniques could be applied and may improve dual-tasking, although this needs to be evaluated.
Limitations
The present study had several limitations. First, multiple Spearman correlations were conducted to test the second study aim and to assess the impact mood has on dual-task performance. Although the accepted level of significance was reduced to try to balance the risk of type I and II errors, multiple correlations still raise the possibility of chance findings. Second, RRMS was the only form of MS scrutinized in this study; therefore, it is unknown if the same dual-tasking effects would be found in other types of MS, or to those with greater levels of disability. Third, the methods do not allow for differentiation between potential explanations for the disproportionate dual-task decrement.
The cognitive screening test used (ACE-III) has not been formally validated in an MS population, but did show group level differences between the groups suggesting it is sensitive to cognitive impairment in MS, as it was in Hamilton et al. (Reference Hamilton, Rochester, Paul, Rafferty, O’Leary and Evans2009). If specifically examining hypotheses relating to cognitive impairment and dual-task performance, measures sensitive to more subtle impairment (such as the SDMT) are recommended.
It was noted that several RRMS participants were taking medications, but the study was not sufficiently powered to analyze the specific impact of MS-related medication on dual-task performance. The number of participants using walking aids was not recorded, and this should be done in future studies.
The DTQ has not been extensively validated in MS. There was a highly significant difference between scores on the test in people with MS and controls in the present study. Evans et al. (Reference Evans, Cullen, Paul, Frei, Norrie and O’Leary2014) found some evidence of a relationship between DTQ score and level of dual-task decrement on a walking/digit span dual task, but given the absence of a relationship with level of dual-task decrement in the present study more extensive validation of it as a specific measure of everyday dual-tasking is required.
Future Research
This was the first dual-tasking study in an RRMS population to manipulate task demand by using Backward Digit Span, and so should be replicated. This methodology could also be applied to different types of MS. Future studies could also explore the impact of this more cognitively demanding task on gait. Despite reporting significantly higher levels of everyday dual-tasking difficulties the level of difficulty was not explained by the severity of dual-task difficulties on the balance/digit span tasks measured by degree of dual-task decrement. It will be important to determine whether the DTQ questionnaire is a valid measure of everyday dual-tasking difficulties and if so, what accounts for these difficulties. Furthermore, future work should also focus on developing a clinical tool to measure day-to-day balance and dual-tasking difficulties in MS.
CONCLUSIONS
RRMS causes difficulties with dual-tasking, impacting balance, particularly under challenging conditions, which may contribute to an increased risk of gait difficulties and falls. The relationship between anxiety/depression and dual-task decrement suggests that emotion could be contributing to dual-task difficulties, and raises the possibility that therapeutic interventions aimed at managing anxiety/mood may improve cognitive–motor dual-tasking.
ACKNOWLEDGMENTS
We thank all of the participants in this study and all NHS Highland staff who assisted with recruitment. The authors have neither conflicts of interest nor financial support related to this work.








