


Introduction
The external auditory canal consists of two sections, which are separated at the narrowest (isthmus) portion. The inner two-thirds – the bony canal – is formed by the tympanic bone antero-inferiorly and postero-inferiorly, the squamous temporal bone superiorly, and the mastoid bone posteriorly. The outer third of the external auditory canal is cartilaginous. The external auditory canal is lined with keratinising stratified squamous epithelium. The skin over the lateral aspect is thicker, comprising a subcutaneous layer, hair follicles, sebaceous glands and wax-secreting ceruminous glands. These structures are absent in the skin over the more medial bony canal, which is closely adherent to the underlying periosteum.
Lesions arising in the external auditory canal that require surgical excision are uncommon. From 2009–2010, in England (which, according to the 2008 census, had a population of around 50.76 million), only 574 in-patient completed consultant episodes were coded as D08.1: ‘extirpation of lesion of external auditory canal’.1
We describe a 10-year personal case series of external auditory canal lesions requiring surgical excision, and provide discussion of the relevant literature.
Materials and methods
A 10-year review of external auditory canal lesions was performed. Data were collected prospectively as patients attended; these were crosschecked with operating theatre databases to ensure completeness. Information regarding histopathology and imaging features were obtained from a subsequent case note review. Imaging characteristics were reviewed by one of the authors of this paper (RDW).
Results
Data were collected from 48 patients (mean age of 59 years) over the time period. Of these, 38 (79 per cent) had pre-operative imaging with computed tomography (CT), of which 4 also had a magnetic resonance imaging (MRI) scan. All underwent surgical management for a diverse range of conditions, grouped broadly into five categories: bony lesions, infective, neoplastic, epithelial disorders and other benign lesions. The range of lesions is presented in Table I.
Table I Case series lesions

Pt = patient; y = years; M = male; F = female; MOE = Malignant otitis externa; EAC = external auditory canal; BCC = Basal cell carcinoma; SCC = Squamous cell carcinoma; LCH = Langerhans cell histiocytosis; chol = cholesteatoma; KO = keratosis obturans
The surgical management of bony lesions was dependant on the degree of external auditory canal obstruction. All exostoses in this series were removed via a postauricular approach, with the exception of one osteoma case (pictured in Figure 1) which was removed via a transcanal approach. The postauricular approach provided optimum visualisation, especially of the anterior exostosis, as well as access for drilling. The skin was elevated from a lateral to medial direction and the most posterior exostosis was removed first. The bony canal wall was followed to the new bone and the new bone was removed. The exostosis was ‘egg shelled’ (cavitated) and collapsed in order to preserve the canal skin. Care was taken to preserve the tympanic membrane and identify the annulus. The facial nerve was monitored during the procedure. The preserved skin tube was then replaced, but some secondary intention healing was required to line the newly enlarged bony canal.

Fig. 1 Clinical photograph of an external auditory canal osteoma.
The infective lesions were managed via a transcanal approach in order to avoid opening tissue planes and facilitating the spread of infection. All patients in this series underwent biopsy of external auditory canal granulations to exclude malignancy, which is the main differential diagnosis of such lesions, and had local debridement of sequestrum. Polypectomy was performed in the operating theatre as opposed to the out-patient setting in these cases in order to attain an adequate view of the tympanic membrane. The authors prefer not to remove polyps blindly as they may be adherent to the stapes superstructure or facial nerve. Careful removal also facilitates examination of the tympanic membrane and middle ear.
Small benign tumours were removed using both permeatal and endaural approaches, although the improved access and visualisation associated with the endaural approach was preferred as it facilitated complete excision. The resulting defects were left to granulate and heal by secondary intention. No complications were seen with this approach and the lesions were excised completely.
For suspected malignant lesions, a biopsy alone was performed using a permeatal approach, followed by an appropriate resection or radiotherapy. The basal cell carcinoma (BCC) included in this series were managed by sleeve excision of the ear canal skin. The details of each group are discussed below.
Discussion
Bony lesions
Exostoses are the most common bony abnormality of the external auditory canal and are typically multiple and bilateral. There is now strong evidence that exostoses are related to cold water exposure.Reference Chaplin and Stewart2, Reference Robinson and Gleeson3 The underlying pathology may be a periosteitis following exposure, leading to new bone formation. Exostoses are often asymptomatic, but if large and/or multiple, they may occlude the external auditory canal, resulting in otitis externa and conductive hearing loss.
High resolution CT aids diagnosis (a typical example of a CT image of external auditory canal exostoses is shown in Figure 2). Umeda et al. Reference Umeda, Nakajima and Yoshiola4 described a scoring system to grade the percentage obstruction of the external auditory canal, but this has not been translated into treatment recommendations. Active intervention is not required if the condition is asymptomatic, but earplugs could be recommended for continued cold water exposure. Conservative treatment would include regular aural toilet to prevent complications. Surgery for obstructive canal exostoses is challenging: there may be very little space between the bony swellings; the overlying skin is thin; access can be poor; and the tympanic membrane, facial nerve and temporomandibular joint are all at risk during bone removal. High resolution CT is recommended to identify disease when the tympanic membrane is not visible. Exostoses are likely to recur after removal if exposure to cold water continues.
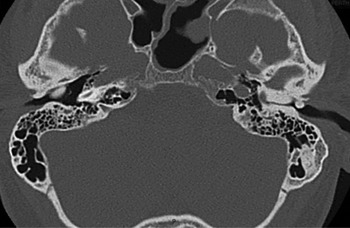
Fig. 2 Axial computed tomography image of external auditory canal exostoses, showing bony narrowing of the left external auditory canal typical of exostoses.
Osteomas are benign tumours of the bony external auditory canal. They are typically unilateral and solitary, and arise from the tympanosquamous or tympanomastoid suture lines.Reference Michaels, Cardesa and Slootwig5 Osteomas are slow-growing, frequently asymptomatic and may be an incidental finding, but may cause obstructive symptoms and conductive hearing loss. Per operative photograph of external ear canal osteoma is shown in Figure 1. Non-obstructive lesions can be managed conservatively, with aural toilet and observation. An expanding or obstructive mass may need to be removed to prevent or alleviate symptoms. The transcanal or endaural approach is favoured because osteomas typically arise from a narrow pedicle, which can be fractured and drilled flush to the bony canal without having to elevate much skin.
Infective lesions
Malignant otitis externa was the most common infective lesion identified in this case series. It is more accurately described by the term ‘skull base osteomyelitis’, which reflects the underlying pathological condition. Malignant otitis externa commonly presents in an immunocompromised host, typically an elderly diabetic person, with severe otalgia and unilateral otorrhoea. There may be invasion of local structures and necrosis of skin, cartilage and bone. Cranial nerve palsies may ensue with involvement of the petrous apex. Pseudomonas aeruginosa is the commonest pathogenic micro-organism,Reference Babiatzki and Sade6 although other pathogens including fungi have been identified.Reference Gordon and Giddings7
Imaging of the skull base is required, both for diagnosis and for assessing progress. High resolution CT scanning is useful for delineating bony erosion, whereas MRI is preferable when skull base inflammation and cranial nerve involvement is suspected. However, changes are not specific for malignant otitis externa and further diagnostic imaging may be of benefit. Technetium-99m bone scintigraphy is sensitive in detecting bony involvement and is therefore used for diagnostic purposes, whereas gallium-67 scintigraphy is useful to monitor the response to antimicrobial treatment. Prolonged and targeted systemic antimicrobial therapy is required. Fluoroquinolones (particularly ciprofloxacin) have a high cure rate and are the treatment of choice.Reference Gehanno8 However, antimicrobial resistance to ciprofloxacin is emerging and must be suspected in patients with deteriorating clinical features (such as new cranial nerve palsies) or rising inflammatory markers.Reference Bernstein, Holland, Porter and Maw9 Hyperbaric oxygen has been used with some benefit as an adjuvant to antimicrobials,Reference Shupak, Greenburg, Hardoff, Gordon, Melamed and Meyer10 but a Cochrane review found no evidence from randomised controlled trials to support this treatment.Reference Phillips and Jones11
Polyps in the external ear typically arise from the middle ear and indicate underlying inflammatory disease.Reference Tay and Hussain12 However, this is not necessarily the case in Asian populations, in whom aural polyps have been shown to be associated with pathology of the external auditory canal.Reference Loh13 Dawes and Soames reported cholesteatoma in 60 per cent of children with aural polyps.Reference Dawes and Soames14 Aural polyps will often regress with intensive conservative treatment (cautery and topical antimicrobials),Reference Hussain15 but polypectomy should be considered for histology and to facilitate examination of the middle ear if the polyp persists. The differential diagnosis includes both neoplastic and granulomatous conditions, such as tuberculosis, syphilis, and xanthomatosis and eosinophilic granuloma.Reference Tay and Hussain12
Neoplastic lesions
In the current case series, 14 lesions were neoplastic, with 11 different histological diagnoses. Seven lesions were classed as benign (ceruminous adenoma, paraganglioma, angiomyxoma, haemangioma, neuroma and lipoma), while the other seven were of varying malignant potential.
Ceruminous adenomas are rare tumours of the external auditory canal, which are composed of well-differentiated tubular, ductal or papillary structures. Thompson et al. (2004) reviewed the 32 cases in the English literature and described the pathological features of these tumours.Reference Thompson, Nelson and Barnes16 Care must be taken to differentiate ceruminous adenoma from pleomorphic adenomas of the parotid gland and paragangliomas that can arise in this area.
Cavernous haemangioma presenting exclusively in the external auditory canal is extremely rare. Covelli et al. reviewed the world literature in 2008 and identified 10 case reports prior to their own.Reference Covelli, De Seta, Zardo, De Seta and Filipo17 The patient in this present series had a sensation of fullness and tinnitus, which resolved after local excision. The haemangioma arose from the antero-superior external auditory canal and was removed via a small endaural incision.
One patient initially presented with papillomata of the ear canal, which were managed by cold steel excision followed by CO2 laser ablation. After several months of indolent disease she re-presented with multiple papillomata and a small focus of conversion to squamous cell carcinoma (SCC).Reference Miah, Crawford, White and Hussain18
Complete removal of benign and malignant lesions is advised, although it can be difficult to achieve adequate excision margins given the close relationship with the bony canal. Many lesions in this series were removed via a small endaural incision. This technique provides adequate access for tumour removal, it is quick and carries minimal morbidity.
Both BCC and SCC in the external auditory canal can be aggressive because they are not dependant on ultraviolet light. Such tumours often require more extensive surgery to achieve adequate margins, which typically involves a sleeve excision of the canal possibly including the tympanic membrane. Basal cell carcinoma may be nodular, cystic, morphoeic or pigmented. The histology of a nodular BCC is shown in Figure 3.
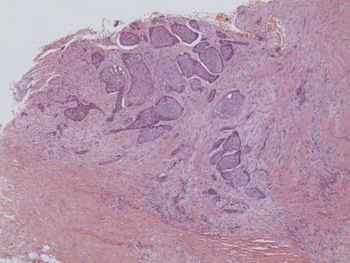
Fig. 3 Photomicrograph of basal cell carcinoma. (H&E; × 10)
A tumour that is invading bone would require an en bloc resection of the ear canal and temporal bone, or treatment with external beam radiotherapy.
This series demonstrates the rare nature of any specific tumour type in the external auditory canal, and emphasises the need for excision biopsy to confirm the diagnosis and guide subsequent treatment.
Epithelial abnormalities
External auditory canal cholesteatoma is characterised by bony erosion and invasion of squamous epithelium, with localised periosteitis and bone sequestration.Reference Shire and Donegan19 This condition is rare, occurring in 1 in 1000 new patients within an adult otologic practice;Reference Anthony and Anthony20 the incidence has been calculated as being 60 times less than that of middle-ear cholesteatoma.Reference Dubach, Mantokoudis and Caversaccio21 The cholesteatoma is typically in the floor of the external auditory canal but can involve the middle ear and mastoid, and facial nerve involvement is not uncommon. The differential diagnosis includes malignant otitis externa and SCC.
Keratosis obturans is characterised by a plug of organised keratin, which causes obstruction of the external auditory canal lumen and expansion of the bony walls without erosion. Keratosis obturans typically causes severe pain and conductive hearing loss, while a dull ache and otorrhoea are more typical of external auditory canal cholesteatoma.
The clinical differences between external auditory canal cholesteatoma and keratosis obturans have been well described by previous authors,Reference Miah, Crawford, White and Hussain18, Reference Persaud, Hajioff, Thevasagayam, Wareing and Wright22 and are summarised in Table II. Piepergerdes et al. Reference Piepergerdes, Kramer and Behnke23 first differentiated between these two entities, postulating that primary external auditory canal cholesteatoma was caused by periosteitis of the bony canal. The cholesteatoma can also arise secondary to congenital or acquired stenosis of the external canal and first branchial arch anomalies.Reference Hickey, Scott and Traub24 In contrast, keratosis obturans arises due to an abnormality of epithelial migration, which has been demonstrated in vivo,Reference Corbridge, Michaels and Wright25 although the aetiology of this condition is not yet known. High resolution CT can help to differentiate the two conditions if this cannot be achieved clinically, and provide information about the middle-ear structures and mastoid air cells in external auditory canal cholesteatoma. Typical examples of CT images of keratosis obturans and external auditory canal cholesteatoma are shown in Figures 4 and 5 respectively. Histologically, keratosis obturans is characterised by subepithelial inflammation without bone erosion, and keratin squames in a lamellar pattern (like onion skin). In tissue samples of external auditory canal cholesteatoma, the keratin is loosely packed and randomly distributed, and there is sequestration of adjacent bone.Reference Naiberg, Berger and Hawke26
• This paper reports a 10-year case series of rare external ear canal masses requiring surgical management, including bony lesions, infective conditions and neoplasms
• Surgical treatment of canal exostoses is challenging and specialist training is recommended
• The range of neoplasms arising in external auditory canal is broad
• Excision biopsy should be performed to identify tumour type and guide subsequent treatment
• We report a cavernous haemangioma arising in the external auditory canal, which is only the 12th case reported to date

Fig. 4 Axial computed tomography image of right-sided keratosis obturans occluding the external auditory canal but not eroding bone.

Fig. 5 Coronal computed tomography image of right-sided external auditory canal cholesteatoma, which has eroded the external auditory canal wall and filled the middle ear.
Table II External auditory canal cholesteatoma and keratosis obturans comparison

EACC = external auditory canal cholesteatoma; KO = keratosis obturans
In cases of external auditory canal cholesteatoma where lesions are limited, local curettage with application of topical antimicrobials may be suitable, but formal tympanomastoid surgery and canalplasty will be required for more extensive disease.Reference Dubach and Hausler27 Keratosis obturans can be managed effectively by removing the keratin plug from the external auditory canal, which may require general anaesthesia. This procedure will typically be repeated at regular intervals, as the epithelial migratory defect is often chronic. Surgical intervention to remodel the external canal has been proposed for intractable cases.Reference Paparella and Goycoolea28
Benign lesions
In the current series, four non-neoplastic lesions were excised for diagnostic histology: epidermoid cysts of the anterior canal wall and tympanic membrane, and an intradermal melanonevus. Excision biopsy is frequently required for such lesions to confirm their benign nature and to relieve local symptoms.
Conclusion
This paper presents a 10-year series of 48 external auditory canal lesions, which demonstrated a range of pathologies. We have emphasised the diagnostic differences between exostoses and osteomas, and between external auditory canal cholesteatoma and keratosis obturans. We have also discussed the management of aural polyps, and highlighted the need to excise external auditory canal masses for histology in order to guide subsequent treatment.
Acknowledgment
We would like to acknowledge the support provided by Dr G Stenhouse (Department of Pathology (formerly Ninewells Hospital), Raigmore Hospital, Inverness, Scotland, UK).







