


Introduction
This review describes the normal anatomy of the adult chorda tympani, aiming to provide a thorough understanding of its course and functions relevant to head and neck surgery. Whilst anatomical variants are included, most congenital malformation syndromes and pathology are beyond the scope of this review.
Search strategy
A systematic literature review was undertaken using the electronic databases Medline, Embase, PubMed, Web of Science, and Cochrane Library and the search engine Google Scholar. The aim was to identify all papers describing the clinical anatomy of the chorda tympani. English-language and human studies were selected, using the search term ‘chorda tympani’ and its subheadings; a few foreign language articles with English abstracts, and relevant animal studies, were also included. Secondary references were retrieved from primary sources, together with evidence-based observations within selected anatomy, physiology and other reference texts.
Central connections
The chorda tympani contains nerve fibres associated with two brainstem nuclei: (1) the superior salivary nucleus, housing the cell bodies of secretomotor preganglionic parasympathetic neurons; and (2) the solitary nucleus, the upper part of which is the gustatory nucleus. The latter receives the central processes of unipolar taste neurons which have their cell bodies in the ganglia of the three cranial nerves conveying taste.Reference Standring1 After synapsing in the gustatory nucleus, secondary axons ascend in the medial lemniscus to relay in the thalamus. The pathway then passes via the posterior limb of the internal capsule to reach the primary gustatory cortex, located within the face area of the somatosensory cortex between the insula and parietal operculum.Reference Onoda, Kobayakawa, Ikeda, Saito and Kida2 It is uncertain whether this pathway is crossedReference Jeppsson3, Reference Lee, Hwang, Rison and Chang4 or mostly uncrossed,Reference Shikama, Kato, Nagaoka, Hosoya, Katagiri and Yamaguchi5 and whether taste is perceived bilaterally in humans.Reference Onoda, Kobayakawa, Ikeda, Saito and Kida2 Other projections from the thalamus pass to the hypothalamic nuclei and the limbic system.Reference Standring1
Within the facial canal
The smaller ‘sensory’ root of the facial nerve, the nervus intermedius (of Wrisberg), conveys special sensory fibres from taste buds on the anterior tongue and soft palate (cell bodies in the geniculate ganglion), together with secretomotor fibres to salivary glands below the oral fissure.Reference Malone and Maisel6–Reference McMinn8 After exiting the brainstem, the nervus intermedius is typically adherent to the vestibulocochlear nerve for a variable distance, before separating to lie adjacent to and finally merge with the facial nerve within the internal auditory meatus.Reference Rhoton, Kobayashi and Hollinshead9 After fusion of its ‘motor’ and ‘sensory’ roots, the facial nerve enters its own Z-shaped canal, the facial (Fallopian) canal, with its labyrinthine, tympanic and mastoid segments.Reference Kerr10, Reference Weiglein11 Typically, the facial nerve gives off the chorda tympani in the vertical mastoid segment, just before it exits the skull at the stylomastoid foramen. At this point, the facial nerve is composed mostly of large, myelinated fibres, with the smaller (approximately 2–3 µm) fibres of the chorda tympani distributed throughoutReference Malone and Maisel6, Reference Kullman, Dyck and Cody12, Reference Ylikoski, Gamoletti and Galey13 rather than aggregated into a discrete bundle as in animals.Reference Ylikoski, Gamoletti and Galey13 Rarely, facial nerve motor fibres travel with an enlarged chorda tympani,Reference Durcan, Shea and Sleeckx14 although this concept has been disputed.Reference Jahrsdoerfer15
From facial nerve to tympanum
The chorda tympani is the largest intrapetrous branch of the facial nerve,Reference Monkhouse7 arising anterolaterallyReference Martin-Duverneuil, Lafitte and Chiras16 below the nerve to stapedius. It passes anterosuperiorly in the posterior canaliculus, accompanied by a branch of the stylomastoid arteryReference Monkhouse7, Reference Anson, Donaldson and Shilling17 sometimes referred to as the posterior tympanic artery.Reference Kulczynski and Wozniak18 The posterior canaliculus opens into the middle ear via an aperture situated in the angle between the posterior and lateral walls of the tympanic cavity, just medial to the fibrocartilaginous annulus of the tympanic membrane. This opening is variously described as being level with the upper end of the handle of the malleusReference Standring1 and the round window.Reference Anson, Donaldson and Shilling17 The posterior canaliculus is approximately 0.3–0.5 mm in diameterReference Noble, Warren, Labadie and Dawant19 and arises at a mean angle of 22° from the facial canal.Reference Muren, Wadin and Wilbrand20
The chorda tympani is subject to numerous anatomical variations, consistent with the aphorism ‘the hallmark of the temporal bone is variation’.Reference Anson, Donaldson and Shilling17, Reference Donaldson and Anson21 After branching off the facial nerve, the chorda tympani accompanies it for a variable distance before entering the posterior canaliculus,Reference Kulczynski and Wozniak18 which joins the facial canal on average 4–5 mm proximal to the stylomastoid foramen,Reference Weiglein11, Reference Kullman, Dyck and Cody12 near the level of the lower margin of the bony tympanic ring (Figure 1).Reference Yasumura, Takahashi, Sando, Aoki and Hirsch22 This branching point is variable (Table I), in part because some studies have measured the point at which the chorda tympani leaves the facial nerve whilst others have recorded the junction between the posterior canaliculus and the facial canal (Table I). In congenital malformations, the chorda tympani may arise more proximally, even at the geniculate ganglion.Reference Fowler and Edmund25 The posterior canaliculus is between 3 and 14 mm long; in approximately 10 per cent of individuals, it is a sulcus on the posterior wall of the external acoustic meatus rather than a true canaliculus.Reference Kulczynski and Wozniak18
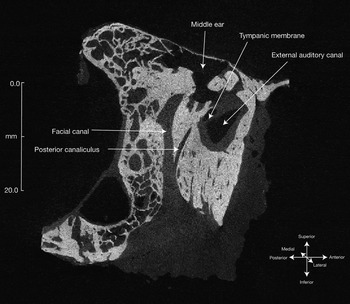
Fig. 1 Sagittal micro-computed tomography scan through a cadaveric temporal bone (from a 64-year-old man), showing the facial canal and the posterior canaliculus.
Table I Studies on origin of chorda tympani from facial nerve
*Extratemporal distances unknown. †Chinese. SF = stylomastoid foramen; 3D = three-dimensional
The true prevalence of an extratemporal origin of the chorda tympani is uncertain. In the two largest studies, this prevalence varied between 212 and 5 per cent.Reference Kulczynski and Wozniak18 There may be ethnic differences. In a study of 30 temporal bones from Chinese cadavers, the chorda tympani had an extratemporal origin in 53 per cent, which the author attributed to a difference in mastoid morphology, with a more ‘proximal’ stylomastoid foramen.Reference Low24 When the chorda tympani originates outside the temporal bone, the posterior canaliculus is entirely separate from the facial canal.Reference Anson, Donaldson and Shilling17, Reference Nager and Proctor26 Rarely, the chorda tympani has a bifid origin from the facial nerve.Reference Donaldson and Anson21 An extratemporal origin of the chorda tympani is readily understood if its development is considered. In the fetus and young infant, the chorda tympani leaves the facial nerve outside the skull,Reference Weiglein11 but with postnatal growth of the mastoid it migrates to a more proximal position (i.e. the facial canal grows more than the mastoid segment of the nerve),Reference Yasumura, Takahashi, Sando, Aoki and Hirsch22, Reference Fujita, Nakashima, Sando and Takahashi23 resulting in the chorda tympani typically diverging from the facial nerve within the facial canal by one year of age.Reference Weiglein11
Across the tympanum
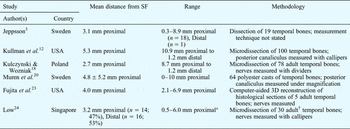
The chorda tympani arches upwards to cross the pars flaccida of the tympanic membrane, medial to the upper part of handle or neck of the malleus and above the insertion of tensor tympani.Reference Anson, Donaldson and Shilling17, Reference Kulczynski and Wozniak18 It lies just medial to the inner mucosal layer of the tympanic membrane, adjacent to the posterior and anterior mucosal folds of the malleus (Figure 2).Reference Anson, Donaldson and Shilling17, Reference Palva, Northrop and Ramsay27 Occasionally, in infants at least, the chorda tympani is suspended from the latter within its own mucosal fold. In contrast to some reports,Reference Durcan, Shea and Sleeckx14, Reference Bosman28 there is no firm evidence to suggest that the chorda tympani innervates the mucosal surface of the tympanic membrane.Reference De Lara Galindo, Segura, Avella, Alaminos and Rosas29
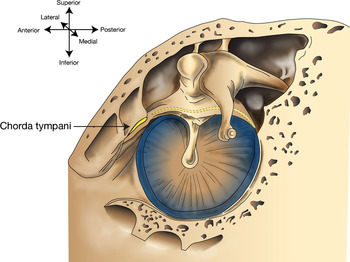
Fig. 2 Illustration of the right middle ear, viewed from the tympanum laterally. The chorda tympani traverses the tympanic membrane from posterior to anterior.
A few anatomical variants of the tympanic segment of the chorda tympani have been described. Two cases have been reported of the chorda tympani lying in a transtympanic bony sheath, associated with conductive hearing loss.Reference Kraus and Ziv30, Reference Ozmen, Sarac, Sennaroglu and Turan31 Lateral displacement of the chorda tympani has been found in association with congenital deformity of the malleus.Reference Gerhardt32 Unilateral or bilateral duplication of the chorda tympani is rare, but in such cases one component may pass lateral to the neck of the malleus within the tympanic membrane.Reference Durcan, Shea and Sleeckx14
Electron microscopy shows that the tympanic segment of the chorda tympani consists of about 5000 nerve fibres, two-thirds of which are myelinated.Reference Ylikoski, Gamoletti and Galey13 In the rat, most of these myelinated fibres are sensory afferents, whilst the unmyelinated fibres are secretomotor efferents.Reference Ylikoski, Gamoletti and Galey13
From tympanum to infratemporal fossa
The chorda tympani exits the tympanum via a separate bony canal, the anterior canaliculus (canal of Huguier), which runs within the medial part of the slit-like petrotympanic fissure.Reference Toth, Moser, Patonay and Olah33 The entrance to this canal is through a foramen immediately above the petrotympanic fissure.Reference Toth, Moser, Patonay and Olah33, Reference Gray34 Accompanying the chorda tympani in the petrotympanic fissure are the anterior tympanic branch of the maxillary artery,Reference Monkhouse7, Reference Anagnostopoulou, Venieratos and Antonopoulou35 lymphatics,Reference Anagnostopoulou, Venieratos and Antonopoulou35 and two wedge-shaped ligaments, namely the anterior malleolar ligament (which connects the anterior aspect of the neck of the malleus to the sphenomandibular ligament) and the discomalleolar ligament (which runs between the malleus and the capsule and intra-articular disc of the temporomandibular joint (TMJ)).Reference Kim, Jung, Kwak, Shim, Hu and Park36 The chorda tympani is the most medial of these structures, and the two ligaments are separated by a bony, septum-like ridge.Reference Kim, Jung, Kwak, Shim, Hu and Park36, Reference Sencimen, Yalcin, Dogan, Varol, Okcu and Ozan37 The anterior canaliculus runs parallel and anterior to the pharyngotympanic tube.Reference Toth, Moser, Patonay and Olah33, Reference Gray34 It crosses the temporo-sphenoidal suture and exits the skull by a minute foramen behind the base of the spine of the sphenoid;Reference Gray34 it does not directly communicate with the mandibular fossaReference Toth, Moser, Patonay and Olah33 but is closely related to the medial surface of the TMJ.Reference Siessere, Vitti, Semprini, Regalo, Iyomasa and Dias38 As it exits the sphenoid bone, it frequently gives off a branch to the cartilaginous part of the pharyngotympanic tube.Reference Kulczynski and Wozniak18, Reference Bosman28 The anterior canaliculus is not fully formed until five years of age; before this, the chorda tympani lies in a groove in the petrous part of the temporal bone.Reference Toth, Moser, Patonay and Olah33 If the canal remains open laterally, TMJ activity may precipitate a variety of symptoms.Reference Toth, Moser, Patonay and Olah33
From the infratemporal fossa distally
The chorda tympani descends medial to the spine of the sphenoid and angles forward to join the lingual nerve approximately 1–2 cm below the base of the skull, just above the lower border of the lateral pterygoid muscle (Figure 3).Reference McMinn8, Reference Erdogmus, Govsa and Celik39 Communications between the chorda tympani and the lesser petrosal nerve or otic ganglion have been reported.Reference Kulczynski and Wozniak18, Reference Bosman28
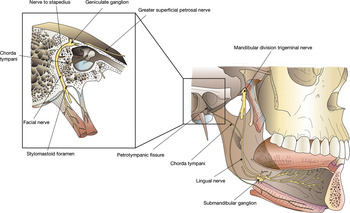
Fig. 3 Schematic illustration of the course of the chorda tympani from the facial nerve to the lingual nerve. Inset shows an oblique vertical slice through the temporal bone. The anterior two-thirds of the tongue are a lighter shade to indicate the area innervated by the chorda tympani.
The lingual nerve descends anteriorly between the lateral surface of the medial pterygoid muscle and the mandible, grooving the medial surface of the mandible between the posterior attachment of the mylohyoid muscle to the mylohyoid line and the mandibular attachment of the superior constrictor to the pterygomandibular raphe.Reference Standring1 It then continues forward medial to the posterior root of the mandibular third molar tooth,Reference Erdogmus, Govsa and Celik39, Reference Du Toit40 where it occupies a variable position covered only by gingival mucosa.Reference Pogrel, Renaut, Schmidt, Ammar and Kiesselbach41 After crossing the superior aspect of the deep part of the submandibular gland, the lingual nerve loops under the submandibular duct in the floor of the mouth, from lateral to medial, to enter the tongue. The diffuse distribution of chorda tympani nerve fibres within the fascicles of the lingual nerve probably accounts for the poor recovery of taste function after lingual nerve repair.Reference Girod, Neukam, Girod, Reumann and Semrau42
The submandibular ganglion lies on the surface of the hyoglossus muscle, above the deep part of the gland, suspended from the lingual nerve by several filamentous branches. Preganglionic parasympathetic nerves from the chorda tympani synapse in the ganglion, and postsynaptic fibres either pass directly to the submandibular gland and its duct or rejoin the lingual nerve to innervate the sublingual salivary gland. A few preganglionic fibres traverse the ganglion and relay in ganglion cells at the hilum of the submandibular gland.Reference Standring1, Reference McMinn8, Reference Blatt and Bunto43
Imaging the chorda tympani
Both the posterior canaliculus and the course of the chorda tympani across the middle ear can be seen in vivo with conventionalReference Martin-Duverneuil, Lafitte and Chiras16 and high-resolution computed tomography,Reference Parlier-Cuau, Champsaur, Perrin, Rabischong and Lassau44 particularly modern 64-slice scans which allow three-dimensional reconstruction.Reference Noble, Dawant, Warren and Labadie45 The anterior canaliculus is not visible. We could find no reports of magnetic resonance imaging of the normal chorda tympani.
Other anatomical variants
Major anatomical variations of the chorda tympani appear to be rare, apart from those described above, except in the presence of severe congenital malformation.Reference Durcan, Shea and Sleeckx14 There is one report of the chorda tympani arising from the facial nerve outside the skull and running forward lateral to the styloid process to join the lingual nerve, without entering the temporal bone, but this was in association with a major congenital ear malformation.Reference Altman46 All or part of the chorda tympani may be duplicate; if one of these nerves arises extratemporally, it may enter the temporal bone by its own separate foramen rather than via the stylomastoid foramen.Reference Donaldson and Anson21 We found only one reference to complete absence of the chorda tympani; this was in children with severe ear anomalies.Reference Saito, Watanabe, Fujita, Fujimoto, Inokuchi and Ogura47
Functions of the chorda tympani
The chorda tympani conveys taste sensation from the anterior two-thirds of the tongue and secretomotor innervation to the salivary glands in the floor of the oral cavity. It has been suggested that the chorda tympani also conveys nerve fibres serving additional functions: general sensation (including pain and temperature) from the anterior two-thirds of the tongue; secretomotor fibres to the parotid gland; and efferent vasodilator fibres to the tongue.
Taste
Each taste bud comprises numerous gustatory receptor cells innervated by multiple nerve fibres.Reference Standring1 Taste buds are found throughout the oral cavity and pharynx, but are particularly plentiful on the papillae of the presulcal dorsal and lateral regions of the tongue. Taste is conveyed centrally via several cranial nerves, as follows:
(i) The lingual nerve carries general sensation and taste from the anterior two-thirds of the tongue,Reference Jeppsson3, Reference Schwartz and Weddell48 excluding the region of the circumvallate papillae. Taste fibres travel with the chorda tympani. Although these generally convey ipsilateral taste sensation, electrogustometric studies indicate that there is bilateral innervation of the tip of the tongue.Reference Tomita, Ikeda and Okuda49, Reference Berteretche, Eloit, Dumas, Talmain, Herman and Tran Ba Huy50 This is supported by detailed dissections of the lingual nerve which show a unilateral distribution, except at the tip of the tongue where there is also contralateral innervation.Reference Rusu, Nimigean, Podoleanu, Ivascu and Niculescu51
(ii) The glossopharyngeal nerve transmits general and taste sensation from the posterior one-third of the tongue, the circumvallate and foliate papillae,Reference Yanagisawa, Bartoshuk, Catalanotto, Karrer and Kveton52 and the oropharynx.Reference Standring1
(iii) Vagal taste fibres are less well characterised, but taste buds are present on the epiglottis.Reference Jowett and Shrestha53, Reference Kano, Shimizu, Okayama and Kikuchi54
(iv) Finally, the lesser palatine (maxillary division of the trigeminal nerve) and greater petrosal nerve (facial nerve) convey taste sensation from the soft palate.Reference Ikeda, Ikui and Tomita55
However, the anatomy is more complex. Some studies have identified anastomoses between the lingual and glossopharyngeal nerves, and found that the glossopharyngeal nerve projects more anteriorly than the posterior third of the tongue.Reference Toure, Bicchieray, Selva and Vacher56, Reference Doty, Cummins, Shibanova, Sanders and Mu57 Electrogustometric studies conducted following injury to the chorda tympani during middle-ear surgery suggest that the circumvallate and foliate papillae may be dually innervated by the chorda tympani and glossopharyngeal nerve,Reference Berteretche, Eloit, Dumas, Talmain, Herman and Tran Ba Huy50 and that the area innervated by the chorda tympani varies widely between individuals.Reference Tomita, Ikeda and Okuda49 Studies in which the chorda tympani was anaesthetised in healthy volunteers noted only a modest impairment in taste, prompting the suggestion that the facial nerve may normally inhibit taste perception transmitted by the glossopharyngeal nerve.Reference Catalanotto, Bartoshuk, Ostrom, Gent and Fast58, Reference Lehman, Bartoshuk, Catalanotto, Kveton and Lowlicht59 This mechanism helps to compensate for the loss of taste sensation: damage to the chorda tympani reduces its central input, thereby releasing inhibition on other taste nerves.Reference Bartoshuk, Snyder, Grushka, Berger, Duffy and Kveton60 Finally, one report suggested that in some cases the greater petrosal nerve may also transmit some taste fibres from the anterior two-thirds of the tongue.Reference Schwartz and Weddell48
Salivation
The chorda tympani carries efferent preganglionic parasympathetic fibres to the submandibular and sublingual salivary glands, which induce salivary secretion.Reference Getchell, Doty, Bartoshuk and Snow61 Stimulation of the chorda tympani causes vasodilation in these glands. It is possible that the salivary glands also receive secretory fibres via other pathways.Reference Chilla, Bruner and Arglebe62 This is supported by the observation that citric acid can still elicit secretion from the submandibular gland, albeit considerably reduced, after the chorda tympani has been severed.Reference Chilla, Bruner and Arglebe62–Reference Diamant, Enfors and Holmstedt64 This reflex secretion is inhibited by local anaesthesia of the hypoglossal and glossopharyngeal nerves.Reference Laage-Hellman and Strom-Blad65 Unlike other glands, salivary secretion can occur in response to parasympathetic or sympathetic stimulation,Reference Standring1, Reference Koeppen and Stanton66 but it is unlikely that sympathetic activity is responsible for this ongoing submandibular gland secretion, since stellate ganglion blockade does not reduce the response.Reference Laage-Hellman and Strom-Blad65
General sensation
Action potential recordings from a transected chorda tympani in one patient (accessed at middle-ear surgery) suggested a response to tactile stimulation of the tongue.Reference Oakley67 Some patients experience numbness, tingling or pain after manipulation, stretching or transection of the chorda tympani. Perez et al. Reference Perez, Fuoco, Dorion, Ho and Chen68 objectively assessed general lingual sensation in a prospective, controlled study of 15 patients undergoing middle-ear surgery. Almost half the patients complained of numbness and tingling in the tongue soon after the operation, and were found to have a small but significant reduction in light touch sensation and two-point discrimination on the operated side; these abnormalities resolved within three months. Interestingly, in this study no sensory deficit was recorded in the single patient with a transected chorda tympani. Thus, the chorda tympani may convey general sensation in at least some individuals, but its contribution is small in comparison to the lingual nerve. Alternatively, the chorda tympani may modulate trigeminal sensitivity.Reference Berteretche, Eloit, Dumas, Talmain, Herman and Tran Ba Huy50, Reference Just, Steiner, Strenger and Pau69
Pain
Based on observations in a single patient who reported touch, pain and taste sensation on electric stimulation of an intact chorda tympani, Costen et al. Reference Costen, Clare and Bishop70 hypothesised that the chorda tympani transmits pain. No other studies have reported similar findings. Other authors have suggested that the chorda tympani inhibits pain perception via the lingual nerve, such that damage to the chorda tympani causes the perception of pain from the corresponding area of the tongue affected by loss of taste.Reference Bartoshuk, Snyder, Grushka, Berger, Duffy and Kveton60, Reference Tie, Fast, Kveton, Cohen, Duffy and Green71
Temperature
Gustatory thresholds are affected by temperature.Reference McBurney, Collings and Glanz72 Weak detection of thermal stimuli by the chorda tympani has been reported in a variety of animalsReference Zotterman73, Reference Ogawa, Sato and Yamashita74 and in humans.Reference Oakley67 In these experiments, water at different temperatures was applied to the tongue, which may have stimulated taste perception. However, Ogawa et al. Reference Ogawa, Sato and Yamashita74 showed that a single chorda tympani fibre can respond to both gustatory and thermal stimuli, and a detailed analysis of these results suggested that temperature is detected independently of taste.Reference Andersen and Hartmann75 More recently, it has been demonstrated that heating or cooling small regions of the tongue can induce taste sensation.Reference Cruz and Green76 The authors suggested that this ‘thermal taste’ is due to temperature-sensitive neurons in the chorda tympani encoding taste rather than temperature.
Parotid gland secretion
It has been postulated that the chorda tympani contains secretomotor fibres to the parotid gland.Reference Diamant and Wiberg77, Reference Jeppsson78 This would not be surprising, considering that the superior and inferior salivatory nuclei, which are the origin of preganglionic parasympathetic fibres within the facial and glossopharyngeal nerves, are contiguous.Reference Standring1, Reference Getchell, Doty, Bartoshuk and Snow61 Therefore, some fibres from the inferior salivary nucleus destined for the parotid may run in the chorda tympani. Furthermore, the chorda tympani has been shown to communicate with the lesser petrosal nerve and otic ganglion in up to one-third of individuals.Reference Kulczynski and Wozniak18
Diamant and WibergReference Diamant and Wiberg77 measured salivary secretion in response to citric acid on the tongue. In seven of 10 cases in which the chorda tympani had been unilaterally severed or damaged, they found that parotid secretion was reduced by up to 50 per cent on the operated side. This may be explained by an impaired salivatory reflex response due to a reduction in afferent signals from the chorda tympani. However, unilateral lingual anaesthesia in two patients with normal taste function did not decrease ipsilateral parotid secretion.
Tongue vasodilation
In cats, electrical stimulation of the chorda tympani or lingual nerve beyond the point at which it is joined by the chorda tympani has been shown to induce vasodilation in the tongue. Erici and UvnasReference Erici and Uvnas79 have suggested that this is due to vasodilator fibres in the chorda tympani. This finding has not yet been demonstrated in humans.
Conclusion
This critical appraisal of the clinical anatomy of the chorda tympani highlights the fact that it is more complex than reference anatomy texts indicate. The chorda tympani appears to possess a range of less commonly known functions, in addition to conveying taste sensation from the anterior two-thirds of the tongue and parasympathetic innervation to the submandibular and sublingual salivary glands. This helps to explain the variable effects of transection or damage to the nerve.




