


Introduction
Cardiopulmonary resuscitation (CPR) maneuvers are essential in the management of cardiac arrest. To increase the odds of early return of spontaneous circulation and, consequently, reduce downtime and mortality rate, CPR technique should be as effective as possible.
According to US resuscitation guidelines, one important aspect of CPR is that excessive ventilation should be avoided,Reference Dabrowska and Telec 1 as hyperventilation is detrimental to patient survival rates.Reference O’Neill and Deakin 2
Hyperventilation during CPR is believed to reduce the efficiency of compressions and hinder venous return, as well as prevent the generation of negative intrathoracic pressure.Reference O’Neill and Deakin 2
In preclinical studies with a porcine model, the ratio of surviving animals declined to one out of seven from six out of seven when respiratory rate was increased to 30 versus 12 breaths/minute.Reference Aufderheide, Sigurdsson and Pirrallo 3 This increase in ventilatory rate leads to a reduction in coronary perfusion pressure (regarded as the best hemodynamic marker of CPR efficacy), consequently reducing the odds of survival.Reference Aufderheide, Sigurdsson and Pirrallo 3
To ensure that effective ventilation is achieved during CPR requires understanding which factors limit the proper performance of CPR technique by responders.
The present study was developed to compare the regularity and intensity of non-invasive ventilation during simulated, conventional CPR and ventilatory support performed by trained Basic Life Support responders using three distinct ventilation devices: a standard manual resuscitator (bag-valve-mask, BVM); a BVM equipped with a digital airway pressure manometer; or an automatic transport ventilator.
Methods and Materials
This study was carried out at Escola Superior de Bombeiros (ESB, the fire academy for the state of São Paulo, Brazil), located in the municipality of Franco da Rocha. The sample consisted of firefighters trained in prehospital emergency care.
Due to the risk of cardiothoracic injury when testing resuscitation techniques in human subjects, this study was performed on manikins; no victims or patients were involved.
The study protocol was evaluated and approved by the Ethics Committee of the ESB Department of Emergency Medical Services.
Methods and Measurements
Three groups were established for comparison purposes: the control group (CG), in which responders used BVMs alone, both for ventilatory support and for CPR; the manometer support (MS) group, in which responders used BVMs equipped with digital manometers, both for ventilatory support and for CPR; and the automatic ventilator (AV) group, in which responders used automatic transport ventilators, both for ventilatory support and for CPR. After sample size calculation, 11 responders (nine men, two women) were randomly selected from a cohort of firefighters squad (trained Basic Life Support responders) to perform ventilations in the three different study groups.
The CPR protocol used in the study consisted of 30 compressions followed by two breaths (compression-to-ventilation ratio 30:2), whereas the ventilatory assistance protocol consisted of 12 ventilations/minute.
Three CPR training manikins (QCPR, Laerdal; Wappinger, New York USA) equipped with data-logging airway monitors were used to measure the following variables: pressure, flow, volume, ventilation rate, inspiratory time, expiratory time, and inspiratory/expiratory (I:E) ratio (Figure 1). Pressure and flow measurements for each of the three monitor modules were calibrated and adjusted against an airway monitor previously calibrated at a Brazilian Calibration Network laboratory accredited by the National Institute of Metrology, Quality, and Technology (Inmetro; Rio de Janeiro, Brazil).
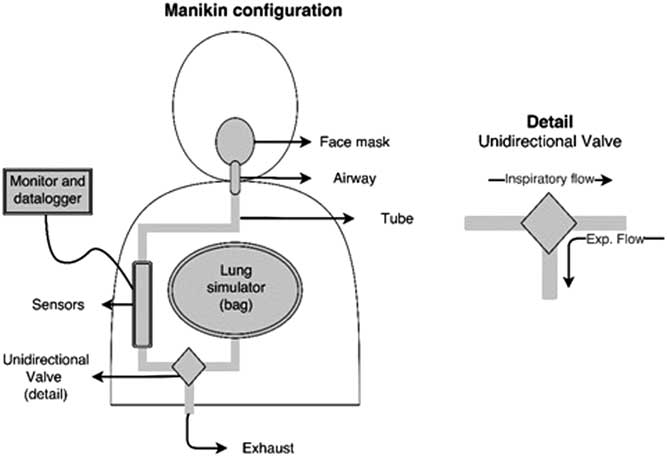
Figure 1 Manikin Configuration.
The devices used in the CG and MS groups were Oxigel (São Paulo, Brazil) brand, adult-size manual resuscitators, consisting of a reusable, autoclavable, silicone reservoir (capacity 1800 ml) and a one-way pop-off valve (pressure limit 60 cmH2O). The devices used for the AV group were time-cycled, pressure-limited, automatic transport ventilators (VentPlus; Vitória, Brazil) with a fixed I:E ratio.
Both the manual resuscitators and automatic ventilators were connected to Ventcare (Buri, Brazil) face masks (with silicone-cushioned rim, inflation valve, and hook ring) secured with Vent 11 model silicone straps. The head strap was used to improve mask seal.
The manometer developed for mechanical ventilation monitoring in this study is a low-pressure, low-power, digital gauge that measures peak inspiratory pressure and minimum airway pressure.
Outcomes
To evaluate the regularity and intensity of non-invasive ventilation during conventional CPR and ventilatory support, it was assessed the peak inspiratory pressure and ventilatory rate.
Statistics
After collection of quantitative data from all respiratory cycles, means and standard deviations were calculated for each group. The generated data were analyzed in PASW Statistics Version 18 (SPSS Inc.; Chicago, Illinois USA). Student’s t-test was used to evaluate statistical differences between groups. P values<.05 were regarded as significant.
Results
The average age of responders was 24 years old (ranging from 19 to 27).
Peak Inspiratory Pressure during Ventilatory Support
Comparison between the CG and MS group revealed a statistically significant reduction (P=.006) in peak inspiratory pressure in the MS group during ventilatory support alone (Figure 2; Table 1).

Figure 2 Mean Peak Inspiratory Pressure with Ventilatory Support. Abbreviations: AV, automatic ventilator; CG, control group; MS, manometer support.
Table 1 Analysis of Peak Inspiratory Pressure Data from Different Ventilatory Support Scenarios

Abbreviations: AV, automatic ventilator; CG, control group; MS, manometer support.
Comparison between the MS and AV groups revealed a significantly lower mean inspiratory pressure (P=.043) in the latter. As expected, comparison between the CG and AV group revealed a significantly higher (P=.0005) peak inspiratory pressure in the CG, in which airway pressure during ventilation was neither monitored nor limited.
Ventilatory Rate during Ventilatory Support
Ventilatory rate was significantly higher in the CG than in the MS (P=.002) or AV (P<.001) groups (Figure 3; Table 2). Comparison between the MS and AV groups revealed a lower ventilatory rate in the latter (P=.041).

Figure 3 Mean Ventilation Rate with Ventilatory Support. Abbreviations: AV, automatic ventilator; CG, control group; MS, manometer support.
Table 2 Analysis of Ventilation Rate Data from Different Ventilatory Support Scenarios

Abbreviations: AV, automatic ventilator; CG, control group; MS, manometer support.
Peak Inspiratory Pressure during CPR
Peak inspiratory pressure during CPR was significantly higher in the CG than in the MS or AV groups (P<.001 for both comparisons; Figure 4; Table 3). Comparison of peak inspiratory pressure during CPR between the MS and AV groups revealed higher values in the former (P=.041).

Figure 4 Mean Peak Inspiratory Pressure with CPR.Abbreviations: AV, automatic ventilator; CG, control group; CPR, cardiopulmonary resuscitation; MS, manometer support.
Table 3 Analysis of Peak Inspiratory Pressure Data from Different CPR Scenarios

Abbreviations: AV, automatic ventilator; CG, control group; CPR, cardiopulmonary resuscitation; MS, manometer support.
Discussion
During ventilatory support, both hyperventilation and excessive inspiratory pressure can increase the risk of organ injury and reduce the patient’s odds of recovery.Reference O’Neill and Deakin 2 , Reference Aufderheide, Sigurdsson and Pirrallo 3
In mammals, a tidal volume of 6.3 mL.kg-1 is considered appropriate.Reference Schultz, Haitsma, Slutsky and Gajic 4 The main causes of inadequate artificial ventilation are excessively high inspiratory pressure and excessively high respiratory rate.
High inspiratory pressures can lead to pulmonary hyperinflation, hemodynamic instability, gastric insufflation, and increased risk of barotrauma and, consequently, pneumothorax.Reference O’Neill and Deakin 2 , Reference Ho-Tai, Devitt, Noel and O’Donnell 5 Gastric insufflation is reported in up to 50% of patients receiving non-invasive pressure support ventilation. The lower esophageal sphincter pressure, or gastroesophageal junction pressure, which prevents reflux of gastric contents into the pharynx and insufflation of air into the gastrointestinal tract during ventilation, is approximately 20-25 cmH2O. The odds of gastric insufflation during BVM ventilation increase five-fold when peak airway pressure increases from 20 to 30 cmH2O.Reference Ho-Tai, Devitt, Noel and O’Donnell 5 High ventilatory rates, in turn, reduce coronary perfusion pressure.Reference Aufderheide, Sigurdsson and Pirrallo 3 , Reference Ho-Tai, Devitt, Noel and O’Donnell 5
In the present study, wide variation and higher ventilatory rates were observed when non-invasive ventilation was provided using a standard manual resuscitator alone, both during CPR and during ventilatory support, than when an AV was used or when the manual resuscitator was equipped with an airway pressure manometer. In this group, inspiratory pressure was also higher than in the MS and AV scenarios, which suggests that ventilation with a BVM alone is associated with increased risk of complications compared to ventilation with a manometer-equipped manual resuscitator or, especially, with an AV.
Limitations
The limitations of this study were the use of manikins instead of humans and a small number of responders assessed; more accurate studies will be necessary to confirm the manuscript’s results.
Conclusion
The study suggests that, in prehospital emergency care settings, ventilatory support should preferably be provided using manual resuscitators equipped with airway pressure manometers or better, using portable AVs, due to the risk of reduction in coronary perfusion pressure and iatrogenic thoracic injury during hyperventilation found using manual resuscitators without manometers.







