


Owing to the fact that three-dimensional echocardiography allows enhancement of morphological description of the cardiac structures, this technique is increasingly considered to be complementary to cross-sectional echocardiography in case of congenital heart disease.Reference Simpson and Miller 1 Thus, three-dimensional echocardiography was proved to improve the detection rate of congenital malformations of the atrioventricular valves in comparison with cross-sectional echocardiography.Reference Takahashi, Mackie and Rebeyka 2 Real-time three-dimensional echocardiography was also recently reported as providing precise anatomical analysis of the mitral valve apparatus in children with mitral ring.Reference Pawelec-Wojtalik, Iorio, Anwar and El Midany 3 An accurate pre-operative description of the mitral valve is required to guide the surgeon in this context because surgical procedure of mitral ring may differ according to its relation with mitral annulus.
Case report
A 2-month-old girl was hospitalised in our institution for recent digestive disorders. Antiacids therapy was started because an oesophagitis was suspected. Owing to the inefficiency of the treatment, an oesophageal endoscopy was performed. No inflammatory lesion was observed during this examination, but, because of a laryngospasm, a vascular filling was necessary. This plasma volume expansion led to syncope with clinical signs of heart failure. Transthoracic echocardiography revealed suprasystemic pulmonary hypertension – systolic pulmonary pressure of 100 millimetres of mercury estimated on the tricuspid regurgitation jet. Cross-sectional echocardiography depicted a supramitral ring (Fig 1) that hampered left ventricular filling. On colour Doppler mode, two antegrade flows were seen through the ring. Three-dimensional echocardiography (iE33 ultrasound system; Philips Medical System, Andover, Massachusetts, United States of America) perfectly showed the mitral ring (Fig 2, Supplementary material (Video 1)) with one main central orifice (2 millimetres in diameter) and a lateral one. The number and location of papillary muscles were normal. After the patient received intravenous diuretics, he was operated on. The surgeon confirmed that the ring that appeared as a fibrous shelf was not adhering to the valve leaflets and was attached between the opening of the left atrial appendage and the mitral annulus. This fibrous shelf was completely removed (Fig 2), allowing the discharge from hospital on post-operative day 16 without any treatment. Since then, the patient did not have any cardiac symptoms.
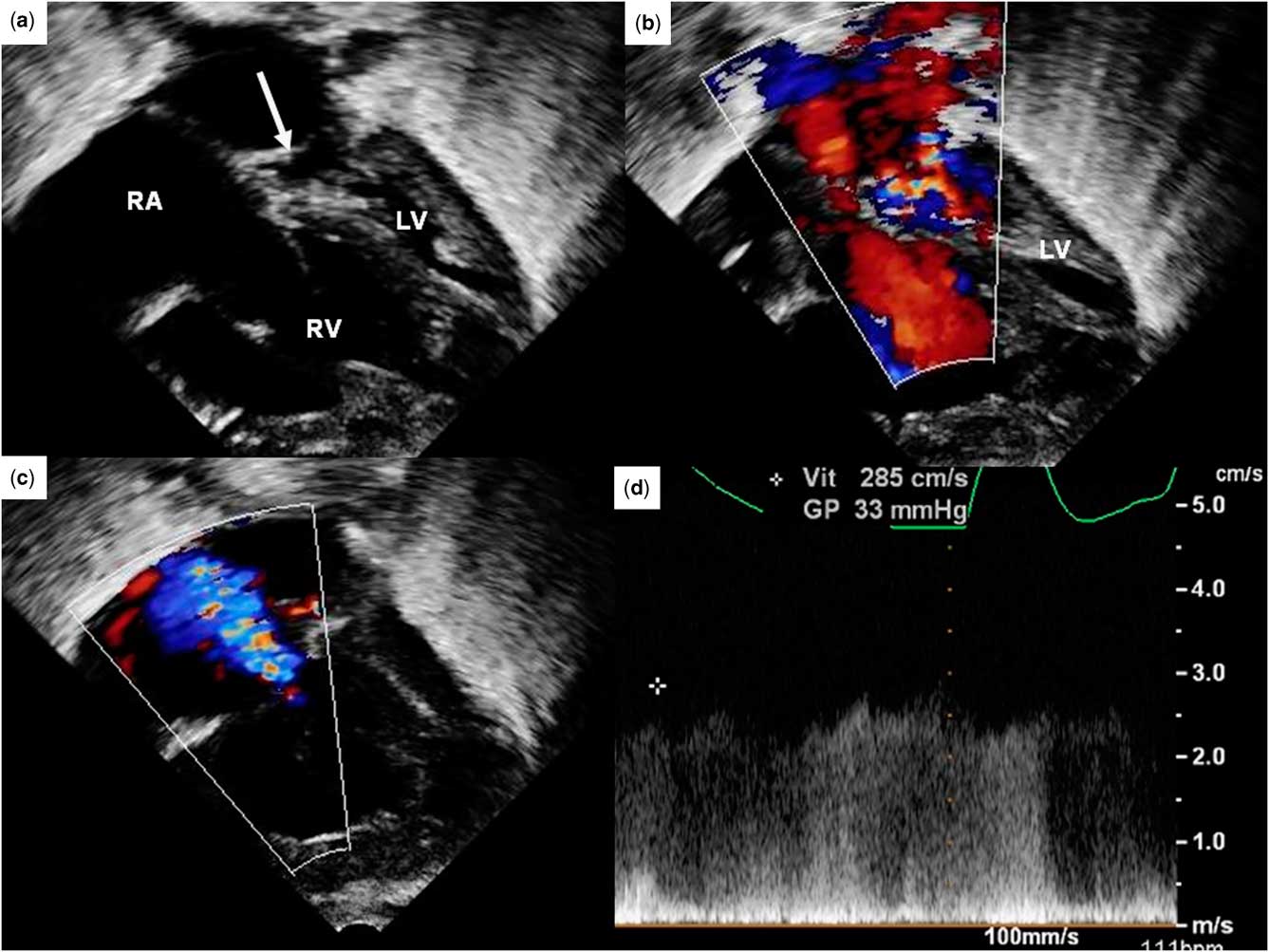
Figure 1 Transthoracic two-dimensional echocardiography showing the supramitral ring in a 2-month-old child. (a) Modified apical four-chamber view showing the mitral ring (arrow), which is located just above the mitral annulus. Owing to the obstruction, the left ventricle is not filled. (b) Colour Doppler mode showing two anterograde flow jets passing through the ring and (c) the tricuspid regurgitation jet that allowed estimation of the systolic pulmonary pressure, which is increased – post-capillary pulmonary hypertension. (d) Doppler mode showing a continuous flow through the ring. LV = left ventricle; RA = right atrium; RV = right ventricle.

Figure 2 Comparison of three-dimensional echocardiographic images with the anatomic specimen. (a) Three-dimensional echocardiography-modified apical four-chamber view showing the fibrous ring (arrow). (b) The supramitral ring is seen as a surgeon from the left atrium (en face view). Two orifices are perfectly depicted (arrows): a central one and a lateral one. (c) The ring is seen after its surgical removal. A catheter was passed through the main hole, illustrating the fact that the blood flow was restricted. (d) Two orifices (arrows) are seen in the specimen. LV = left ventricle; RA = right atrium; RV = right ventricle.
Discussion
Mitral ring is a rare congenital anomaly, which was first described as a component of Shone's syndrome.Reference Anderson 4 In fact, two different entities must be distinguished: intramitral ring, which is a shelf located within the two mitral leaflets, and supramitral ring whose origin is just above the mitral annulus. As for our patient, an intra-operative visualisation of a fibrous shelf that arose beneath the orifice of the left atrial appendage eliminates the diagnosis of the divided left atrium – also named cor triatriatum sinister – and, at the same time, confirms that of the supramitral ring. Indeed, the origin of the divided left atrium is necessarily located above the opening of the left atrial appendage. The two types of mitral rings might still have different embryological origins. Owing to the fact that the intramitral ring is always combined with abnormal subvalvular apparatus, it seems to be a part of an intrinsic mitral valve disease; because the supravalvular ring was found above the tricuspid valve of a congenitally corrected transposition of the great arteries, it was suggested that the supramitral ring would rather be a form of left atrial outlet obstruction – it means a left atrial disease.Reference Marino, Sanders, Parness and Colan 5 This hypothesis is supported by the fact that, in case of the supramitral ring, the subvalvular apparatus is always normal. Both intramitral and supramitral rings are responsible for stenosis that leads to elevated left atrial pressure and post-capillary pulmonary hypertension. Classically, cross-sectional echocardiography reveals dilated right cardiac chambers, whereas the left ventricle is not filled. The definitive treatment of the supramitral ring consists of its surgical removal, which is, most of the time, completely efficient.Reference Toscano, Pasquini and Iacobelli 6
In their series of 15 patients, Collison et alReference Collison, Kaushal and Dagar 7 showed that, using transthoracic cross-sectional echocardiography, the pre-operative diagnosis of mitral ring was possible only for 73% of patients. Moreover, real-time transthoracic three-dimensional echocardiography was proved to be efficient to visualise mitral ring in children.Reference Pawelec-Wojtalik, Iorio, Anwar and El Midany 3 Indeed, this technique allows to see the ring from the left atrium (en face view), as a surgeon. Three-dimensional echocardiography is also helpful to analyse both chordal attachments and papillary muscles. We believe that the combined use of cross-sectional and three-dimensional echocardiography allows both to clarify the diagnosis of congenital mitral stenosis and to provide better morphological analysis of these valves. This is of interest when considering the fact that need for re-operation is 50% in case of intramitral ring, whereas removal of supramitral ring is usually definitive.Reference Toscano, Pasquini and Iacobelli 6 Finally, this observation is unique because, to our knowledge, no other case of multi-perforated mitral ring has ever been reported so far. The two orifices were perfectly depicted by three-dimensional echocardiography, highlighting again its high descriptive value even in small children with congenital heart disease.
Supplementary materials
For Supplementary material referred to in this article, please visit http://dx.doi.org/doi:10.1017/S1047951112000856



