


Introduction
Involvement of the temporal bone as a result of direct extension from an intracranial meningioma is rare. Recognised sites of origin include the tegmen tympani, jugular foramen and internal acoustic meatus. There is a tendency for these lesions to spread to either the middle ear or labyrinthine apparatus.
We discuss the clinical and radiological findings in three cases of intracranial meningioma that presented as a result of external auditory canal involvement. We aimed to highlight the important role of the radiologist in making this potentially challenging diagnosis.
Case reports
Case one
A 35-year-old female was referred with a 2-year history of unilateral hearing impairment. She reported feeling like her ear was constantly underwater and complained of a pressure sensation in the right side of her head. The referring ENT surgeon initially noted a middle-ear effusion and flat tympanometry, for which a grommet was inserted. In light of persistent discharge, the grommet was removed, at which time dehiscence of the external auditory canal roof was noted. This prompted referral for temporal bone computed tomography (CT).
The unenhanced CT comprised images reconstructed with bony algorithm; there were no images reconstructed with a soft tissue algorithm available. Computed tomography was reported to show fluid within the mastoid air cells and non-specific soft tissue swelling in the external auditory canal roof, with no associated bone destruction (Figure 1).
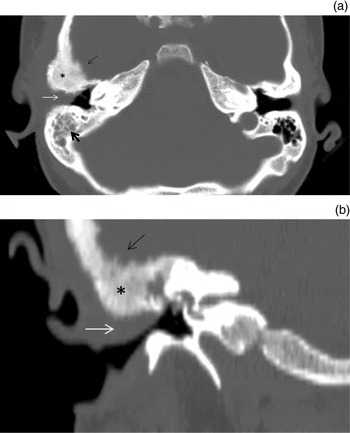
Fig. 1 (a) Axial and (b) coronal unenhanced computed tomography images at the level of the external auditory canal, demonstrating abnormal soft tissue thickening in the superior aspect of the external auditory canal (white arrow), with hyperostosis of the adjacent temporal bone (*) and a ‘hairy’ cortical bone margin (thin black arrow). The mastoid air cells are opacified (thick black arrow).
The patient was managed conservatively. She was reviewed a year later following further deterioration in her hearing and a new complaint of pulsatile tinnitus. At this time, there was a middle-ear effusion and conductive hearing loss; hence, tertiary referral was instigated.
Following local review of the previous CT scans, the temporal bone texture was noted to be abnormal, which was thought to be due to fibrous dysplasia, and magnetic resonance imaging (MRI) was recommended. In the meantime, conservative measures failed to manage the patient's symptoms.
The patient later underwent meatoplasty for symptomatic relief, after which her hearing improved but pulsatile tinnitus persisted. Histology at this time unexpectedly indicated grade 1 meningothelial meningioma. Magnetic resonance imaging demonstrated a large middle cranial fossa meningioma, with extensive temporal bone, middle-ear and external auditory canal involvement (Figure 2). The patient has since undergone surgical excision at another institution.
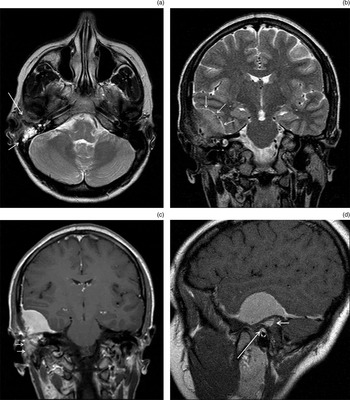
Fig. 2 (a) Axial T2-weighted magnetic resonance imaging (MRI) scan, demonstrating a right mastoid effusion (short arrow) and abnormal intermediate T2-weighted signal material within the external auditory canal and temporal bone (long arrow). (b) Coronal T2-weighted MRI scan demonstrates a large right middle cranial fossa mass (arrows) consistent with a meningioma. (c) Coronal and (d) sagittal T1-weighted MRI scans following gadolinium administration clearly demonstrate infiltration of the temporal bone (short arrows) and extension into the roof of the external auditory canal (long arrow).
Case two
A 58-year-old female was referred to our local ENT surgeons with a 4-month history of otalgia, a blocked ear sensation and pulsatile tinnitus. The patient was known to have a middle cranial fossa meningioma, diagnosed five years previously following MRI for a possible cerebrovascular event.
Examination under anaesthesia revealed a chronically inflamed and oedematous external auditory canal, with swelling in the roof of the canal and an area of exposed bone involving the anterior wall of the external auditory canal. Histology indicated squamous epithelium, possibly cholesteatoma, with no evidence of neoplasia. A temporal bone CT indicated abnormal temporal bone texture, and raised the possibility of continuity of the known middle cranial fossa meningioma with superior external auditory canal swelling (Figure 3).
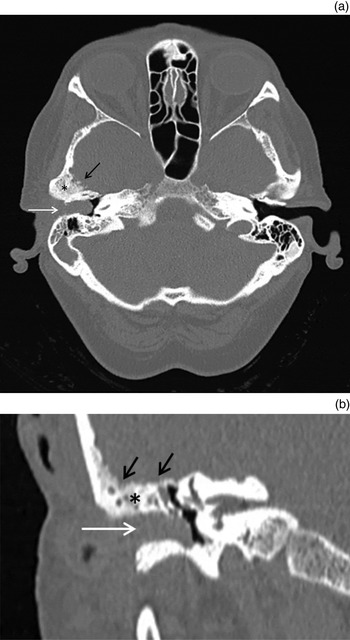
Fig. 3 (a) Axial and (b) coronal computed tomography at the level of the external auditory canal, showing complete stenosis of the right external auditory canal due to a large soft tissue mass (white arrows). There is subtle hyperostosis (*) of the adjacent temporal bone and an irregular ‘hairy’ cortical bone margin (black arrows).
A repeat biopsy showed only hyperkeratosis. Magnetic resonance imaging confirmed the presence of a middle cranial fossa meningioma, and demonstrated direct extension through the substance of the temporal bone to the roof of the external auditory canal (Figure 4).

Fig. 4 (a) Axial T2-weighted magnetic resonance imaging (MRI) scan at the level of the external auditory canal, showing abnormal intermediate signal soft tissue obliterating the canal (arrow). Fat-suppressed (b) axial, (c) coronal and (d) sagittal post-gadolinium T1-weighted MRI scans, demonstrating a middle cranial fossa meningioma (*), with enhancing tumour spreading through the substance of the temporal bone into the roof of the external auditory canal (white arrow) and posterior aspect of the temporomandibular fossa (black arrow).
The patient is currently awaiting stereotactic radiotherapy.
Case three
A 40-year-old female was referred to an ENT team at a neighbouring hospital with a 5-week history of a painful swelling in the right external auditory canal.
Clinical examination revealed abnormal soft tissue in the roof of the ear canal, with intact overlying mucosa and a normal tympanic membrane. An audiogram showed a unilateral 40 dB sensorineural hearing loss. Temporal bone CT indicated abnormal soft tissue within the superior aspect of the external auditory canal and epitympanum of the middle ear, with temporal bone ‘ground glass’ change and irregular bony margins (Figure 5). Histology from incisional biopsy at this time revealed a fibrous lesion. A second pathology opinion raised the possibility of a ceruminous adenoma or low-grade ceruminous adenocarcinoma, and repeat biopsy was advised.

Fig. 5 (a) Sagittal and (b) coronal computed tomography images demonstrate a mass within the superior aspect of the external auditory canal (white arrows). The adjacent temporal bone is hyperostotic (*), with a ‘hairy’ margin (black arrows). (c) Axial image at the level of the superior semi-circular canal nicely demonstrates an expanded, branching Haversian canal (arrow), confirming retained bony architecture.
When reviewed by our local ENT surgeon, the lesion appeared clinically benign, but erosion of the superior and posterior external auditory canal walls was noted. Radiological review suggested the strong possibility of a meningioma in light of the previous two cases, and MRI was requested. Magnetic resonance imaging demonstrated a middle cranial fossa meningioma, extending through the temporal bone to the external auditory canal (Figure 6). A repeat biopsy confirmed grade 1 meningothelial meningioma.

Fig. 6 (a) Sagittal volumetric interpolated breath-hold examination (‘VIBE’) and (b) axial T1-weighted magnetic resonance post-contrast images demonstrate the enhancing middle cranial fossa meningioma (white arrows), with enhancing tissue extending into the substance of the temporal bone through the expanded Haversian canals (black arrows), as was seen on computed tomography (see Figures 5a and 5c).
The patient is currently awaiting stereotactic radiotherapy.
Discussion
Meningiomas are common, accounting for up to 30 per cent of all central nervous system tumours.Reference Fathi and Roelcke 1 They are thought to arise from arachnoid cap cells found within the outer layer of the arachnoid mater, and hence the vast majority of lesions are located intracranially. Direct extracranial extension is seen in up to 20 per cent of patients,Reference Thompson, Bouffard, Sandberg and Mena 2 most commonly involving the orbits, with temporal bone involvement seen very rarely. The temporal bone is also a recognised site of primary extracranial meningiomas, which are thought to arise from ectopic arachnoid cells found within the middle ear and temporal bone, though reports of these are exceedingly rare.
A 2006 review of the imaging features of secondary temporal bone meningiomas described three principal intracranial sites of origin, namely the tegmen tympani, jugular foramen and internal auditory canal, with each having a recognised route of spread to involve the temporal bone.Reference Hamilton, Salzman, Patel, Wiggins, Macdonald and Shelton 3 Tegmen tympani and jugular foramen lesions extend directly into the middle ear, presenting either as treatment-refractory otitis media or conductive hearing loss due to ossicular encasement.Reference Nicolay, De Foer, Bernaerts, Van Dinther and Parizel 4 – Reference Shihada, Lurie and Luntz 6 Internal auditory canal lesions spread to the labyrinthine apparatus, resulting in sensorineural hearing loss, tinnitus and vertigo. We have described three cases where middle cranial fossa meningiomas preferentially spread through the substance of the temporal bone to the external auditory canal, presenting clinically as an external auditory canal mass. This suggests a further potential route of spread in temporal meningiomas.
The majority of external auditory canal meningioma case reports detail extensive lesions that first obliterated the middle-ear cleft and subsequently extruded into the external auditory canal. There are only a few isolated cases where patients have initially presented with external auditory canal pathology,Reference Hemanth, Sreenivas and Chaturvedi 7 – Reference Tsunoda and Fukaya 10 and very little information regarding the imaging of such lesions. A recent radiological review of external auditory canal pathology does not mention meningioma within the imaging differential diagnosis, thus reflecting its rarity.Reference White, Ananthakrishnan, McKean, Brunton, Hussain and Sudarshan 11
Radiological evaluation plays an important role in the investigation of external auditory canal lesions in general, as there are wide-ranging differential diagnoses and clinical findings are often non-specific. As illustrated by two of our cases, temporal meningioma may also prove challenging for the pathologist. These difficulties can lead to delays in reaching a final diagnosis, and significantly longer symptom duration has been shown in cases of external auditory canal meningioma when compared to involvement at other temporal bone sites.Reference Thompson, Bouffard, Sandberg and Mena 2 These factors highlight the importance of the radiologist's awareness of this potential diagnosis and its imaging features, not least because early diagnosis would make subsequent treatment options more straightforward.
Whilst contrast-enhanced MRI is the most sensitive imaging modality for demonstration of both the intracranial and extracranial extent of temporal meningiomas, the initial investigation of undiagnosed external auditory canal pathology in most centres is unenhanced, thin-slice temporal bone CT or cone beam CT. Computed tomography better depicts the intricate anatomy of the temporal bone and allows detection of subtle bone erosion, but provides very little soft tissue detail, a particular limitation of cone beam CT. In addition, as illustrated in our first case, images reconstructed using a soft tissue algorithm are not routinely given to the reporting radiologist in many institutions. These limitations make the detection of small intracranial meningiomas extremely challenging. However, with modern thin-slice temporal CT, there are secondary features, recently described by Nicolay et al.,Reference Nicolay, De Foer, Bernaerts, Van Dinther and Parizel 4 which can direct the radiologist towards the correct diagnosis.
In all three cases described, thin-slice temporal bone CT demonstrated some degree of generalised bony hyperostosis. Preservation of internal trabecular architecture is said to allow discrimination of hyperostosis from the alternate diagnosis of fibrous dysplasia, where normal trabeculae are replaced by a ‘ground glass’ pattern. However, as demonstrated in two of our cases, this can be a challenging distinction to make. If present, expansion of the Haversian canals within the involved bone can be a useful sign to suggest retained architecture. Interestingly, in our third case, there was clear demonstration of Haversian canal expansion on CT, with corresponding enhancement within the expanded canals shown on MRI. This is consistent with the known tendency of meningiomas to spread along the path of least resistance, which in the case of bone is along the Haversian system, via sutures or foramina rather than via direct invasion.
The second, and arguably most useful CT finding is an irregular ‘hairy’ margin to the involved bone, which should direct the radiologist to the potential diagnosis of temporal meningioma.
Thirdly, varying degrees of soft tissue opacification within the external ear canal, with relatively minor middle-ear involvement and an absence of bony erosion, was seen in all cases. This suggests an additional vector of spread for middle cranial fossa meningiomas through the substance of the temporal bone directly to the external auditory canal, with such lesions not necessarily following the more traditionally recognised path through the tegmen tympani to the middle ear.
Gadolinium-enhanced MRI will demonstrate the extent of any intracranial component, which may be immediately apparent as an avidly enhancing dural-based mass, as in all three of our cases. In the case of en plaque meningiomas, this may be indicated by more subtle localised thickening and enhancement of the dura. Magnetic resonance imaging can show enhancing material extending through the substance of the temporal bone, in some cases demonstrably infiltrating the expanded Haversian system. Magnetic resonance imaging is invaluable in mapping the extent of any external, middle-ear and extracranial components, all of which will have implications when considering subsequent management options.
-
• Temporal bone meningiomas most commonly involve the middle ear and labyrinthine apparatus
-
• In rare cases, they may present as a mass within the external auditory canal
-
• Important radiological observations can be made on temporal bone computed tomography
-
• These include generalised bony hyperostosis with internal trabecular architecture preservation, irregular ‘hairy’ cortical bone margins and soft tissue opacification in the external auditory canal
-
• Contrast-enhanced magnetic resonance imaging can demonstrate direct spread from an intracranial meningioma to the temporal bone
In conclusion, direct extension of an intracranial meningioma to involve the temporal bone, and more specifically the external auditory canal, is an extremely rare but important diagnosis to make. Given that the clinical findings may be non-specific and histological diagnosis may prove challenging, it is important for both the surgeon and head and neck radiologist to be aware of this potential diagnosis and its associated imaging features.






