



Introduction
Rationale for study
External auditory canal exostoses are broad-based benign bone growths of the bony ear canal that can develop in response to cold-water and wind exposure. They are often bilateral and frequently asymptomatic until they cause significant obstruction.Reference Cooper, Tong, Neil, Owens and Tomkinson1 There is a latency of several years before the development of external auditory canal exostoses and symptoms.Reference Alexander, Lau, Beaumont and Hope2
Recently, the popularity of cold-water sports in Ireland has risen. Between 2013 and 2018, Swim Ireland reported a 71 per cent increase in competitors attending the Leinster Open Sea Race Series, and the number of Triathlon Ireland memberships has increased by 33 per cent to 135 000.3,4 Additionally, Canoeing Ireland noted a membership increase of 15 per cent in 5 years to 3432, and Surfing Ireland estimated there has been a 5-fold increase in regular surfers in the last 20 years to 50 000.5,6 In 2018, there were over 50 clubs registered with Surfing Ireland, compared with just one in 1997. In a previous Irish study, Lennon et al. found that 88 per cent of surfers diagnosed with external auditory canal exostoses were unaware they had the condition.Reference Lennon, Murphy, Fennessy and Hughes7
Awareness of external auditory canal exostoses
Previous research indicated there was 59–86.1 per cent awareness of external auditory canal exostoses among surfers.Reference Morris, Martin, McCahon and Bennett8–Reference Reddy, Abdelrahman, Lau and Flanagan10 However, previous studies have yet to document the awareness of external auditory canal exostoses among other cold-water athletes, such as open water swimmers, kayakers, triathletes and divers.
Prevalence of external auditory canal exostoses
Several studies have examined the ear canals of surfers, reporting a prevalence rate of 38–80 per cent.Reference Lennon, Murphy, Fennessy and Hughes7,Reference Attlmayr and Smith11–Reference Simas, Hing, Furness, Walsh and Climstein18 Unlike awareness levels, several studies have investigated the prevalence of external auditory canal exostoses among non-surfers. Two studies demonstrated a prevalence of 69.5–79 per cent among the kayaking community.Reference Moore, Schuman, Scott, Mann, Davidson and Labadie19,Reference Cooper, Tong, Neil, Owens and Tomkinson1 Divers have a reported prevalence of 26–87 per cent.Reference Sheard and Doherty20–Reference Karegeannes22 Amongst open water swimmers, Hurst et al.Reference Hurst, Bailey and Hurst13 reported a 21 per cent prevalence rate of severe exostosis. However, there is no English language study published that examines external auditory canal exostoses among triathletes.
The primary aim of this study was to determine the awareness, otological symptoms, community known previous diagnosis and actual prevalence of external auditory canal exostoses in Irish cold-water athletes. The secondary aim was to launch a public awareness campaign.
Materials and methods
Participants
Inclusion criteria included cold-water athletes aged 18 years or over. Informed consent was obtained from all eligible participants prior to participation in this study. Information was provided on the study's aims, format and data protection issues (Appendix 1).
The majority of participants were recruited through the national sporting bodies (Canoeing Ireland, Swim Ireland, Surf Ireland, Irish Underwater Council, Sailing Ireland and Triathlon Ireland), who promoted the study via website and social media forums. Additionally, a link to the questionnaire was distributed among water athletes who were known to the authors, local clubs and outdoor retail outlets.
Phase 1: questionnaire
Irish water athletes were invited to complete an online questionnaire. The questionnaire was shared nationwide through national and local sporting bodies over a three-month period and assessed demographic factors such as age and gender as well as geographical location, water-sport discipline, sporting level, self-reported symptoms and previous diagnosis of external auditory canal exostoses.
Participants’ awareness, knowledge and source of information of external auditory canal exostoses were examined using 10 factual questions and a 5-point Likert scale, based on a study from Morris et al. (Appendix 1).Reference Morris, Martin, McCahon and Bennett8 Awareness was defined as having heard of surfer's ear or external auditory canal exostoses. Scores were assigned categorical values (for knowledge: poor, 10–35; good, 36–42; excellent, 43–50). A further category of ‘knowledgeable’ (good and excellent scores) and ‘not knowledgeable’ (poor scores and unaware) was defined. Univariant and multi–variant regression analysis were performed, using a Hosmer and Lemeshow test. The X2 = 8.12 (p = 0.42), suggesting that the model can accurately predict knowledge about external auditory canal exostoses. The concordance index for this model was 0.74 indicating a good predictive model.
Participants were questioned regarding ear symptoms, such as decreased hearing, ear pain, infection, water trapping or ear blockage. Asymptomatic was defined as no symptoms. Scores were assigned categorical values (one symptom was scored as mild and four or more symptoms were scored as severe symptoms). Univariant and multi–variant regression analysis were performed to determine predictors of symptoms. Using a Hosmer and Lemeshow test, the X2 = 3.52 (p = 0.9), suggesting that the model can accurately predict the occurrence of symptoms in external auditory canal exostoses. The concordance index for this model was 0.76 indicating it a good predictive model.
Participants' attitudes towards wearing ear plugs as a preventive measure for external auditory canal exostoses were assessed across nine questions and measured using a five-point Likert scale coded from one (strongly disagree) to five (strongly agree). Scores were assigned categorical values (for attitudes: less than 27, positive; 27, neutral; more than 27, negative). This model was based on the study by Morris et al.Reference Morris, Martin, McCahon and Bennett8 This information was used to determine what factors might contribute to or limit the compliance of ear plug use. Lastly, participants' level of concern with external auditory canal exostoses, desire to know more information and preferred source of information were assessed.
Phase 2: otoscopic examinations
Three ‘surfer's ear clinics’ were held in a regional hospital out-patient department, and a further three were held at sporting or off site events (farmers market, registration stand at Open Swim and Triathlon Race). An ENT consultant was present at each event and categorised the severity of external auditory canal exostoses. Ethical approval was granted by the Ethics Board of Sligo University Hospital. Otoscopic examinations were performed after wax removal, if necessary, using a Firefly Wired Otoscope DE500 (Belmont, USA) and 4 mm specula.
Statistical analyses
Statistical analysis was performed using SPSS® statistical software (version 26) and GraphPad Prism (version 6; San Diego, USA). Patients were not invited to comment on the study design and were not consulted to develop patient-relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
Phase 1: online questionnaire
Participant characteristics
A total of 1143 online questionnaires were completed, and 217 were excluded based on inclusion criteria. Data from the remaining 926 questionnaires were examined. Table 1 presents the characteristic breakdown of participants. The average age of respondents was 41.2 years (standard deviation (SD) = 12.04 years) and they were involved in their sport for a mean (SD) of 11.07 (10.79) years. Participation in sporting disciplines is illustrated in Figure 1.

Fig. 1. Graph showing number of participants in different sporting disciplines.
Table 1. Participant characteristics*
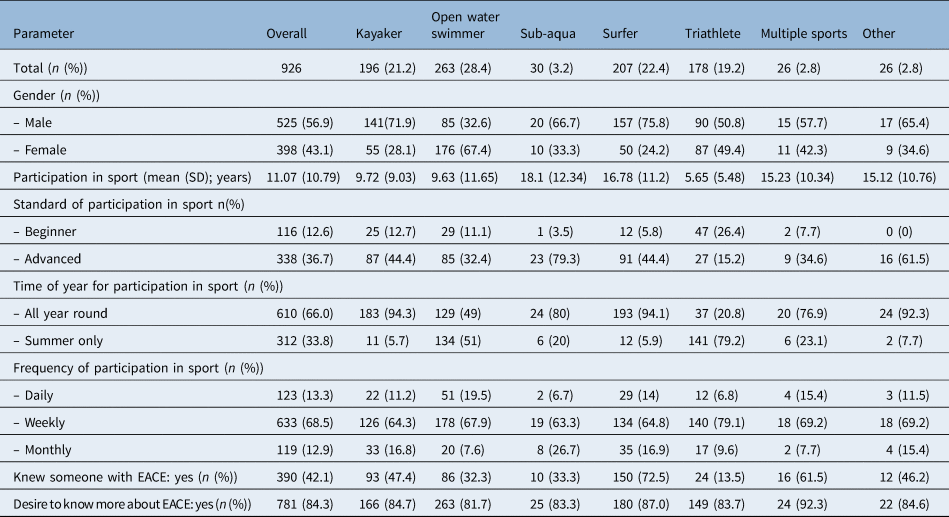
* n = 926. SD = standard deviation; EACE = external auditory canal exostoses
Awareness and knowledge of exostosis
Results from the questionnaire demonstrated that 67.5 per cent (625) of respondents were previously aware of external auditory canal exostoses. Surfers were found to have the most awareness (92.3 per cent) compared with triathletes who had the least awareness (39.9 per cent) of all water athletes. Table 2 outlines the breakdown of awareness of external auditory canal exostoses among different sporting disciplines.
Table 2. Breakdown of participants’ awareness of external auditory canal exostoses

Those individuals with a ‘good’ and ‘excellent’ response were reclassified as being ‘knowledgeable’. Those with ‘no awareness’ and ‘poor knowledge’ were reclassified as ‘not knowledgeable’. The majority of surfers were knowledgeable (85.5 per cent) compared with triathletes (30.3 per cent). Those participating in multiple sports were most interested to learn more (92.3 per cent) and were also most concerned about developing external auditory canal exostoses (73.1 per cent).
Multivariate binary logistic regression analysis was performed to assess the relationship between cold-water athletes and prior knowledge of external auditory canal exostoses. Sport type (p < 0.001) and knowing someone with external auditory canal exostoses (p < 0.001) were significant predictors of having prior knowledge about external auditory canal exostoses. A further breakdown of univariate and multivariate results are outlined in Table 3.
Table 3. Results of the univariate and multivariate analysis for predictors of knowledge

OR = odds ratio; CI = confidence interval
Of the cold-water athletes surveyed, the community known prevalence of external auditory canal exostoses (participants who were previously diagnosed with external auditory canal exostoses) was 9.7 per cent (n = 90). The results also highlighted that 46.7 per cent (n = 42) of reported external auditory canal exostoses cases in our study were among non-surfers. Of those surveyed, the prevalence of external auditory canal exostoses amongst triathletes was 2.8 per cent and for open water swimmers was 4.9 per cent. ‘Other’ cold-water athletes affected included a coast guard volunteer. Surgery had previously been performed on 1.7 per cent (16) of athletes surveyed, including a triathlete and 3 open water swimmers. The breakdown of community known prevalence of external auditory canal exostoses among different sporting disciplines is outlined in Table 4.
Table 4. Community known prevalence, surgical breakdown and symptoms among sporting disciplines

EACE = external auditory canal exostoses
Overall, otological symptoms were experienced by 75.8 per cent (n = 704) of participants, with 76.3 per cent (n = 611) of this cohort experiencing mild symptoms and 23.7 per cent (n = 93) experiencing severe symptoms. The symptoms described include: water trapping (60.5 per cent), ear infection (16.1 per cent), pain (23.1 per cent), reduced hearing (29.5 per cent) and ear blockage (25.5 per cent). Table 4 outlines the breakdown of symptoms by sporting discipline.
Regression analysis shows that age (odds ratio = 0.98; p = 0.003), female gender (odds ratio = 0.7; p = 0.04), years of exposure (odds ratio = 1.04; p = 0.002), ear plug use (odds ratio = 0.79; p = 0.03) and diagnosis of external auditory canal exostoses (odds ratio = 3.35; p = 0.008) were all significant predictors of having symptoms of external auditory canal exostoses, whereas sport type, standard, time of year, frequency of participation, skull cap use, and living near the sea, river or lakes were not significant predictors of having symptoms of external auditory canal exostoses (Table 5).
Table 5. The univariate and multivariate odds ratios for independent variable predictors of ‘symptom’ over ‘no symptom’

OR = odds ratio; CI = confidence interval; EACE = external auditory canal exostoses
Ear protection
Within this study, the use of two forms of ear protection were examined: ear plugs and skull caps or hoods. Of those surveyed, just over half (50.4 per cent) of cold-water athletes used a skull cap or hood whereas 37.1 per cent used ear plugs.
The highest compliance with skull cap or hood use was among sub-aqua (66.7 per cent) and surfing (67.5 per cent) participants, whereas multiple sport participants had the highest use of ear plugs (61.6 per cent). Appendix 2 outlines the breakdown of skull cap and ear plug use in sporting disciplines.
A total of 63.9 per cent (n = 592) of participants reported a ‘positive attitude’ towards ear plug use with triathletes (74.7 per cent; n = 133) having the highest level compared with all other sporting disciplines. However, actual use of ear plugs among triathletes was only 28.7 per cent (n = 51). Hearing loss associated with wearing ear plugs was identified as the main deterrent for athletes across all sporting disciplines.
Phase 2: clinical otoscopic exams
A total of 180 cold-water athletes were examined during the 6 ‘surfer's ear clinics’, with 29.4 per cent (n = 53) of athletes diagnosed with external auditory canal exostoses. There was no significant difference between the percentage of right and left ear occlusion (39.6 ± 26.9 per cent vs 41.4 ± 27.5 per cent; p = 0.76).
Otoscopic features correlated to questionnaire
The completed questionnaires and findings from the otoscopic examination were complete for 139 participants (see Appendix 3 for external auditory canal exostoses prevalence by sport). The overall prevalence of external auditory canal exostoses was 23.7 per cent (n = 33). Only 3.6 per cent knew of this diagnosis prior to examination. Those that developed external auditory canal exostoses participated in cold-water sport for a greater number of years (mean = 15.3, SD = 12.2) compared to those without external auditory canal exostoses (mean = 7.44, SD = 7.5). Multivariant analysis failed to determine any predictors of external auditory canal exostoses including years in sport, standard, frequency, time of year involved in sport, ear protection and sport discipline.
Discussion
Why we did it?
The study was based in County Sligo on the West Coast of Ireland, an area renowned for surfing and open water sports. Several of the authors have an interest in open water sports, and awareness and knowledge of external auditory canal exostoses was anecdotally variable across different sports. This formal study emanated from local and national sporting body discussions.
The rise of open water sports
Open water sports such as open water swimming, triathlon and surfing in Ireland have seen a rise in popularity from 15 to 71 per cent.3–6 Awareness of external auditory canal exostoses varies between different water sports. Surfers in particular have a greater knowledge of external auditory canal exostoses. We report 92.3 per cent of Irish surfers were aware of external auditory canal exostoses, but 11 per cent had ‘poor knowledge’. Among Australian surfers awareness ranged from 88.2 to 100 per cent.Reference Simas, Hing, Pope and Climstein9 This compares to a UK based paper by Morris et al. with 86.1 per cent awareness and ‘poor knowledge’ in 23.4 per cent.Reference Morris, Martin, McCahon and Bennett8 Our study is the first the authors could find to document awareness and knowledge among non-surfers, specifically triathletes and swimmers. These cohorts have an awareness of 39.9 and 58.5 per cent, respectively. We have yet to determine whether increased media awareness campaigns will increase awareness, diagnosis and possible prevention with ear plugs.
Strengths and limitations
This is one of the largest national studies of external auditory canal exostoses in open water athletes. The study's initial online questionnaire phase had responses from across the entire country of Ireland. Building on this information, open clinics were established where athletes could view their own external auditory canal exostoses and the team could correlate the otoscopic findings to their questionnaire. As a result of our findings, a significant local, regional and national media awareness campaign was conceived.
• Awareness of external auditory canal exostoses among emerging sports such as triathlon is low (39.9 per cent)
• Sub-aqua divers were the least knowledgeable of external auditory canal exostoses at 36.7 per cent
• Overall otological symptoms were experienced by 75.8 per cent, but ear plug use reduced ear symptoms
• Eighty-four per cent wished for further external auditory canal exostoses health advice, predominantly through social media
• Increasing cold-water activities have the potential to increase the workload of general practitioners and ENT surgeons
• Awareness of ear protective equipment such as ear plugs may reduce the morbidity of external auditory canal exostoses
Authors of this study promoted awareness at two competitive kayaking events. Articles detailing the hazards of cold-water exposure were reported in many local and national newspapers. Furthermore, two specific magazine articles were created for kayakers (Flowstate) and general practitioners (Forum). A scientific poster (information slide) detailing the study's findings was created and displayed alongside a digital illustration to raise awareness in hospital out-patient departments (Appendix 1).
A television interview with authors and open water swimmers was broadcast as a news article on national television (Raidió Teilifís Éireann (RTÉ) followed by a regional radio interview (Ocean FM). A webpage detailing information on external auditory canal exostoses and study findings was published on the national health website (Saolta). Additionally, a series of videos were produced for social media platforms (YouTube, San Bruno, USA, and Facebook, Menlo Park, USA).
One of the limitations of the questionnaire was regarding the question of date of birth. Many found scrolling through the year selection onerous and led to many inputting their date of birth as 2019. This resulted in the athlete's exclusion in phase 1 (217 respondents) and phase 2 (41 respondents) of the study. The design of the clinics was contrasting: three clinics were in a hospital setting and three were at competition registrations. There was potential selection bias in those who attended the clinics, with perhaps only the most symptomatic attending.
Further study
Areas of further research in the non-surfing cohort are required. For example, there are high risk groups such as ‘ice water swimmers’ (who swim in water of temperatures of 5°C and lower) who are yet to be studied. Two of the clinics in this study were held at race events registration open water and swimming events. Further studies of kayakers and divers at similar race or meeting events would be useful to document. A follow-up national awareness study should be performed to determine if increased awareness and fewer symptoms have been achieved.
Surfer's ear: a misnomer?
The online questionnaire aspect of this project demonstrates two points: 9.7 per cent of participants (n = 90) were previously diagnosed with external auditory canal exostoses, of whom 46.7 per cent were non-surfers, and surfers are no more symptomatic than other cold-water athletes. Therefore, the term surfer's ear is not an appropriate term, and it may thwart the efforts to bring awareness to other cold-water athletes. The authors suggest a more accurate patient friendly title such as cold-water athletes’ ear because one of the aims of this project is to highlight non-surfing cohort awareness, prevalence and attitudes to ear protection. Several papers have documented the prevalence of external auditory canal exostoses among kayakers and divers.Reference Cooper, Tong, Neil, Owens and Tomkinson1,Reference Moore, Schuman, Scott, Mann, Davidson and Labadie19,Reference Sheard and Doherty20 The implications of not raising awareness is that a greater number of cold-water athletes will gradually develop external auditory canal exostoses and become symptomatic. Inevitably, this leads to increased presentations of otitis externa, ear toileting and ultimately invasive surgery. In Cornwall, an increase of 1.3 per cent of cold-water athletes requiring surgery was observed over a 9-year period.Reference Attlmayr and Smith11 Surgery for external auditory canal exostoses is not without complications, such as hearing loss, facial nerve injury, temporomandibular injury and restenosis.Reference Fisher and McManus23–Reference Whitaker, Cordier, Kosjakov and Charbonneau27
Acknowledgements
We wish to acknowledge the assistance of Aoife Morrissey (communications officer, Saolta Group), Eileen Magnier (RTE), John McMorrow (RTE cameraman), Aileen Concannon (Sligo Research and Ethics Foundation), hospital security, clerical staff and management of Sligo and Letterkenny University Hospital, local, provincial and national sporting organisations, and the Irish Institute of Otorhinolaryngology. We would like to thank the ENT department of Sligo University Hospital as well as the local and national sporting bodies who contributed to the promotion of the study. We wish to thank Mr Simon Morris, Mr Niall Considine, Ms Mary Bresnihan, Mr Hafeez Khan, Mr Javed Munir, Dr Sam Jaber, Dr Mamdoh Stefen, Dr Mohammed Hijazi, Dr Constantine Melu, Dr Marcel Jinih, Dr Fiona Boland, Mr Martin Young, Mr Douglas Hetzler, Fionn Rodgers, Francis O'Grady, Connie Brady, Sally Boland, Dr Maeve Leonard, Niall McDonald, Paddy Doherty, Dr Aoife Moriarty, Dr Aisling Moriarty, Dr Eoin Kelleher, Dr Eoin McCarthy Deering and Dr Eamonn Murphy for their expertise. Funding was granted for this project for purchase of an otoscopic camera from the Sligo Research board.
Data available on request.
Competing interests
None declared
Appendix 1. Knowledge questions
– Surgery is the only cure for surfer's ear
– Ear wind chill contributes to surfer's ear
– All surfers are at risk of surfer's ear
– Surfer's ear/exostosis can completely close up the ear canal
– Surfer's ear is due to cold-water exposure
– You cannot see surfer's ear/exostosis by looking in a mirror
– Surfer's ear/exostosis can be prevented
– Surfer's ear/exostosis is due to bone growth in ear canal
– Surfer's ear/exostosis features ear infections & hearing loss
– Only long-term water athletes get surfer's ear/exostosis

Fig. 1. Likert scale example
Attitude questions
– Ear plugs limit my hearing in the water
– Ear plugs interfere with feeling immersed in the sea
– Ear plugs are uncomfortable
– Ear plugs are anti-social
– Ear plugs cost too much
– Ear plugs will reduce my balance
– Ear plugs affect my performance
– I accept that surfer's ear/exostosis is inevitable if I don't wear ear plugs
– I feel self-conscious wearing ear plugs
Information slide
Title: To determine water athletes’ awareness of surfer's ear or exostosis and attitudes to wearing ear plugs
Introduction and study information section
You are invited to take part in a research study undertaken by the Ear, Nose and Throat Department at Sligo University Hospital. It is important for you to understand why this research is being done and what it will involve. Please take time to read the following information carefully and discuss it with others if you wish. If you would like more information, please email surfersearproject@gmail.com. Take time to decide whether or not you wish to take part. Thank you for reading this.
What is the purpose of this study
Surfer's ear or exostosis are benign bone growths in the ear. It is associated with cold-water exposure particularly seen in surfers. An Irish study determined 66 per cent of surfers in Ireland can have these bone growths, 88 per cent of whom were unaware of their diagnosis (Auditory canal exostoses in Irish surfers, P. Lennon et al.). Surfers are not the only water participants potentially at risk – any person exposed to prolonged cold-water exposure may develop surfer's ear.
A previous study in the UK determined 86 per cent of surfers reported awareness of surfer's ear (awareness and attitudes towards external auditory canal exostosis and its preventability in surfers in the UK by S Morris et al.). There is paucity in the literature to determine the awareness of surfer's ear in Irish kayakers, triathletes, open water swimmers, sailors and sub-aqua participants and attitudes towards ear plugs. The aim is to answer these questions, as well as raising awareness of surfer's ear and potential preventative measures. This study involves a questionnaire.
You have been chosen as you are either a water or non-water athlete. Those picked as a non-water athlete will be used as a control to determine general baseline information.
The questionnaire takes around 3 minutes to complete. No treatment or intervention will be performed in this study. The aim is to gather information on awareness of surfer's ear and attitudes to ear plug use. All information which is collected about you during the course of the research will be kept strictly confidential.
What are the possible disadvantages and risks of taking part
No intervention will be performed.
What are the possible benefits of taking part
The benefits of this study are to raise awareness of surfer's ear and potential prevention of surfer's ear in water athletes. The information we obtain from this study may help us to provide better outcomes for future patients with surfer's ear.
What happens when the research study stops and what will happen to the results of the study
The results of this study will be analysed. The data may be accepted for publication to a medical journal and may be presented at national medical meetings. This is an observational study. If you are concerned you may have surfer's ear, please contact your GP.
The Research Ethics Committee of Sligo University Hospital have reviewed this study.
For Further Information please contact Seamus Boyle, ENT Spr, Dept. of ENT Sligo University Hospital by email: surfersearproject@gmail.com
Thank you for your time.
Appendix 2. Breakdown of use and attitudes towards ear protection by sporting disciplines

Appendix 3. Breakdown of otoscopic examination and diagnosis of EACE by sporting disciplines








