



The International Health Regulations (IHR) (2005) require states parties to develop, strengthen, and maintain national capacities necessary for the surveillance of, verification of, and response to potential health threats, and to apply these at their designated points of entry as outlined in Annex 1 (IHR). This legal instrument contains rights and obligations for countries concerning prevention, surveillance, and response health measures applied to international travelers at the point of entry (POE).1 International airports, ports, and ground crossings are required to have health units for undertaking public health measures during routine times and specific measures during the time of public health emergency of international concern (PHEIC). All 194 World Health Organization (WHO) Member States, including India, agreed to implement the IHR (2005). Effective implementation of the framework requires overall national coordination. Preparedness for cross-border implications is vital to facilitate a speedy and effective response to public health emergencies and to deal with cross-border movements resulting from crises.Reference Merrill, Rogers and Ward2 Borders are vulnerable in times of crises because they are increasingly under pressure by a number of cross-border movements.Reference Cohen, Brown and Alvarado-Ramy3,4 Different types of crises – natural disasters, environmental emergencies, man-made crises, cross-border health emergencies, or conflict situations – may all result in a sudden influx of relief goods and personnel, while at the same time people may decide or have to flee across the border, or emergencies may threaten to spill over to neighboring countries. Officials at the border are the first to be confronted with these dynamics, and border security can become affected.4
Several current emerging threats and risks exposing public health vulnerabilities are linked to global processes, such as economics, trade, transportation, environment and climate change, and civil security. Many of these processes are influenced or affected by the migration and mobility of human populations. International migration, which is a supporting component and a consequence of globalization, increasingly affects health in migrant source, transit, and recipient nations. The flow of populations between locations with widely different health determinants and outcomes creates situations in which locally defined public health threats and risks assume international or global relevance.Reference Gushulak, Weekers and MacPherson5 Ground crossings vary in their public health relevance. Whereas some are used mainly for trains or cargo transport and rather link to environmental hazards, others can have a traveler volume of 30 000 to 50 000 per day, often involving queues and waiting times. Some ground crossings are located close to populated areas and big cities, whereas others are in remote or mountainous areas.6 State parties may designate ground crossings to have capacities aimed at protecting the health of travelers and populations, and at containing public health risks at source.
International travel can pose various risks to health, depending on the characteristics of both the traveler and the travel. Failure to respond in a timely manner by local public health authorities undermines the IHR and can be detrimental to the national economy. The exposure to hazards, the conditions of vulnerability that are present, and insufficient capacity or measures to reduce or cope with the potential negative consequences calls upon proactive, all hazards approach, especially, at international points of entry.7 In terms of public health, migration has implications for recognition of threats, as well as for surveillance and response capacity. Migration also influences broader aspects of the “health of the public,” including the background burden of chronic or latent diseases (both infectious and noninfectious) and patterns of preexisting immunity; it also influences the use and uptake of disease prevention and health promotion interventions, and health care service utilization, in general.Reference Gushulak, Weekers and MacPherson5,8
Currently, the WHO-IHR “Assessment Tool for Core Capacity Requirements at Designated Airports, Ports, and Ground Crossings” is designed to score core capacity compliance at designated POE where states often focus resources to building infrastructure and capacity. These are typically the international airports and ports. The same tool was used in this study for assessing the core capacity compliance at the ground crossing of Attari-Wagah border of India and Pakistan.
METHODOLOGY
A qualitative study was conducted at the selected POE. Attari, the busiest ground crossing in India, was selected due to its large inflow of international passengers, as well as trade consignments. The overall objective of the study was to assess the implementation status of IHR (2005) at a ground crossing in prevention and control of public health emergencies. The WHO-IHR assessment tool for core capacity requirements at designated airports, ports, and ground crossings9 was used for assessing the core capacity compliance at the designated international ground crossing of North India. It was used to obtain observational data on the implementation status of IHR at the Integrated Check Post (ICP), Attari border, Amritsar District Punjab. The tool focuses on the capacities required for communication and coordination, prevention, and control of PHEIC at routine times and emergencies, as well as to identify IHR implementation gaps and requirements at the designated POE, which is ICP, Attari. ICP, Attari is an international ground crossing.
This tool consists of checklists that include the requirements for communication, coordination, and adoption of measures at all times (routine) and during emergencies. Components of the IHR core capacity assessment for designated points of entry include details of the POE, such as characteristics of the ground crossing, medical, and public health services available at and/or near the ground crossing, as well as coordination with nearby health facilities or referral health facilities. It consists of a scored assessment that reflects current stage of IHR implementation, which is defined as “Full,” “Partial,” or “None.” This assessment helps in recognizing gaps, strengths, weakness, and work plan on future improvement. An in-depth interview guide was designed to gather information to complement data collected via the IHR assessment tool. A qualitative method enabled to capture informants’ perceptions, experiences, thoughts, and their understanding of the IHR (2005) requirements at POE. It enabled to discuss, clarify, and compare the existing situation with required standards of IHR (2005). The respondents included the officials who were among the key stakeholders at the ground and were willing to be included in the study. The interview guide had a set of themes for both the officials. The meetings were arranged with the officials, visits to isolation sites, and general observations were conducted regarding facilities on routine activities and other infrastructure and equipment that can be used during emergencies, as described in the tool. The questions for the officials included the themes on understanding of the IHR, stakeholder involvement, current implementation, barriers, and suggestions. Respondents were provided with the objectives, and written informed consent was obtained from all those who were willing to participate in the study. The interviews were conducted until the data saturation was achieved. At the end of the interview, the participants were also provided with the additional information to improve their awareness. Progress on the implementation of IHR (2005) and core capacity measurements of compliance were used to generate study findings. This research has been approved from the Institutional Ethical Committee and International Health Division under Directorate General of Health Services. The Clinical Trial Registry – India (CTRI) for the study was done prospectively before the enrollment of the first participant. Confidentiality and anonymity of the participants were maintained.
RESULTS
WHO Tool Assessment Score
The assessment tool for core capacities at designated airports, ports, and ground crossings describes the scored status in the following.
Part (A) Checklist for Core Capacity Requirements for Coordination, Communication of Event Information, and Adoption of Measures (in regard to activities concerning designated airports, ports, and ground crossings, according to Annex 1A of IHR)
Implementation gaps and system requirements identified from the tool are at the level of requirements under Part A (achieved score, 78%) of the tool, which relates to coordination, communication of event information, and adoption measures, which is the international communication link with the competent authorities at other POE regarding strengthening of the bilateral sharing of public health information with the neighboring country for better coordination is required. It is found that there is a gap regarding the legal and administrative provisions to conduct inspections and receive reports of cases of illness in order to empower competent authority to conduct inspection to identify public health risks together with required control measures to be applied is required. The draft regarding these provisions have been prepared and taken up to the respective ministries for approval. Scored assessment results along with identified gaps, strengths, weakness, and work plan on future improvement are outlined in Tables 1 and 2.
TABLE 1 WHO Tool Scored Assessment Along With Identified Gaps and Status
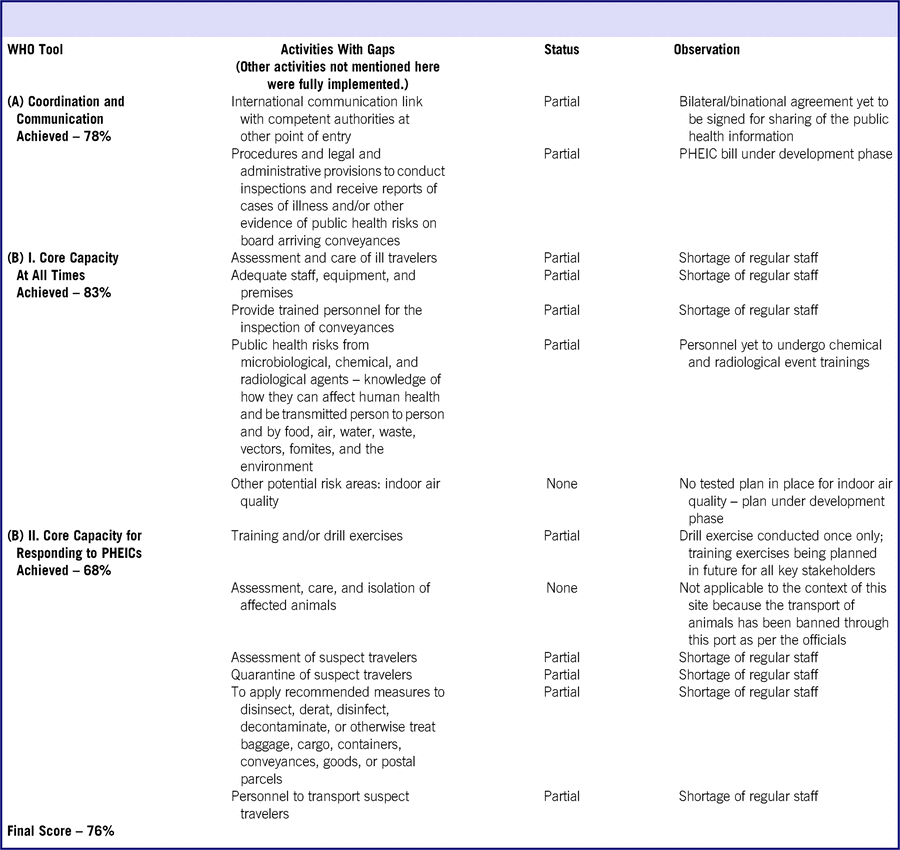
TABLE 2 WHO Tool Scored Assessment Along With Identified Strengths, Weaknesses, and Work Plan on Future Improvement

Part (B) Checklist for Core Capacity Requirements for Designated Airports, Ports, and Ground Crossings
The field visits were planned to observe the activities related to prevention of health risks associated with travel and trade of the aforementioned officials that are conducted at the ICP. The key stakeholders identified at the ICP involved in various activities such as facilitation of travel and trade include customs, immigration, security forces, and quarantine teams, as outlined in Table 3.
TABLE 3 Key Stakeholders at Integrated Check Post – Attari

ABQ- Airport and Border Quarantine, Attari
FRRO- Foreigners Regional Registration Officer
IDSP- Integrated Disease Surveillance Programme
At All Times (Routine)
Under Part B Section 1 of the tool (achieved score, 83%) concerning requirements during all times (routine), it was found there is a need to regularly test the list of facility names for accuracy and accessibility to relevant personnel. There is also need to ensure appropriate number of trained personnel assigned for these duties, in relation to volume and frequency of travelers and complexity of the POE. There is need to ensure control measures for potential risks from air quality to ensure a safe environment.
For Responding to Events That May Constitute PHEIC (Emergencies)
Under Part B Section 2 (achieved score, 68%) concerning responding to events that may constitute PHEIC (emergencies) of the tool, it is found that there is need to conduct periodic drill exercises to familiarize contact points of key sectors with public health contingency plan and respective roles and functions within it. An appropriate number of trained personnel to interview and provide final assessment of suspect travelers is required. The score is inclusive of the requirement for assessment and care of affected animals, but as per the officials, the trade of animals or animal products is banned at this POE. So the requirement for designated veterinary facility was not applicable in this case. Reliable equipment calibrated and maintained in accordance with recommendation is required to ensure application of entry or exit controls for travelers.
Stakeholder Interviews
The interview guide was used, which included a set of questions specified for the officials. The domains covered in the interview guide for the officials included understanding of IHR, stakeholder involvement, current status, barriers, and suggestions.
Understanding of IHR
Knowledge
On interaction with the stakeholders, knowledge among them regarding the implementation of IHR was profound. All of them were aware about the role of health agency in preventing the spread of health risks and controlling them at the land port along with their own respective roles in facilitating travel and trade without any unwarranted restrictions in coordination with all of the key stakeholders. All of them agreed that they are well informed about the unit responsible for implementing these regulations – all of the measures that need to be taken during routine and emergencies.
Trainings/orientation
When asked for any trainings they have received regarding PHEIC, other related activities from the stakeholders, most of them agreed that they have attended the meetings and received training.
The medical unit here is excellent, they already have built MoUs and contacts with various local agencies to handle emergencies well. In case of any foreseeable event, they follow their SOPs, they immediately alert all the stakeholders for their active participation in ensuring safety of everyone. They have already provided us with trainings in case we came in contact with suspected infections like precaution measures, use of PPEs, etc. Key Informant (KI)-008
Stakeholder Involvement and Current Status
Emergency medical services
On interaction with stakeholders regarding their exercises for prevention and control of infectious diseases, they shared that India being free from diseases like yellow fever and polio, surveillance at the ICP and monitoring of vector control are important activities that are conducted. There is also provision of emergency medical aid and other activities, which include inspection of potable water supplies, catering establishments, public wash rooms, and appropriate solid and liquid waste disposal services at the ICP. Besides public health activities, health officials deployed at ICP are also part of the Emergency Medical Task Forcedealing with various medical emergencies (PHEIC, disasters, etc.) at the POE. Standard operative procedures have been incorporated to detail the steps to be undertaken and related documents required for each activity while ensuring uninterrupted International traffic and trade.
Capacity requirements
Land port health units at ICP are equipped for handling PHEIC. During PHEIC, there is the contingency plan involving all stakeholders. The responsibility of the Land Port Health Officer (LPHO) is to implement it practically with coordination of all stakeholders. The field worker and the other staff are part of the team during PHEIC as part of the Standard Operating procedures under the directions of the LPHO.
Field workers will assist in passenger screening procedures, isolation, listing of contacts, transportation of ill/suspect travelers and assisting in arranging the logistics including PPEs. KI-006
Lab diagnosis
The stakeholders mentioned that lab capacity at the national level is National Centre for Disease Control (NCDC), Delhi and National Institute of Virology (NIV), Pune, which have the capacity to provide laboratory diagnosis of Zika virus disease in acute febrile stage. These 2 institutions are the apex laboratories that support the outbreak investigation and for confirmation of laboratory diagnosis.
The samples of the specimen will be collected as per the guidelines of the expert group under DGHS (Directorate General of Health Services). Samples will be transported as per the guidelines for collection and transportation to the designated laboratory as prescribed in the procedure. The cold chain will be maintained for transfer of the samples or samples will be collected and sent to reference lab as per the prescribed procedure. KI-006
Barriers
Financial viability
When asked for any barriers, the stakeholders highlighted the challenge regarding perishable items:
Cold storage could not be made functional due to financial viability as the perishable items imported are very less in quantity. Sometimes there is chance of spoilage of such items and often need to be disposed in case items are not claimed in time. KI-003
Trade restriction
On interaction it was revealed by stakeholders about the challenge of trade restrictions:
About 50 trucks delivering soy were exported from Attari after obtaining required certification from concerned authorities; it was restricted for some reason at their side which was not revealed, and the case had been going on. KI-004
Suggestions
Constructive involvement
Some of the stakeholders added that constructive involvement is required to deal with their current challenges to ensure functioning of the activities at this port even during emergencies. One of the stakeholders revealed that mechanical systems were installed to prevent laborers in handling raw materials that can be harmful in long-term exposures to ensure their health, but it was protested by them:
Constructive involvement with the labor force to allow mechanical systems to be installed which can remain functional during emergencies and prevent restriction of trade. Need to make the labor sector more organized, with the use of biometric system. Recently, a conveyor belt was introduced for the ease of trade but it was protested by the laborers. KI-002
Sufficient supplies
Some of the stakeholders highlighted that sufficient supplies and equipment are important in the handling of any emergencies:
Sufficient medical supplies and equipment need to be maintained, so that the health unit is empowered to provide health care services whenever required and even be able to tackle emergencies well. KI-007
Sufficient staff
All of the stakeholders mentioned the need to ensure that appropriate number of staff is there.
One staff from the health unit is also required at the cargo side to cater to truck drivers from Pakistan; sometimes, for security reasons, it can be difficult for them to access health care, yet the health unit has been very cooperative and the required medical attention is usually provided to them. Drivers report very rarely for any health care yet it must be taken care of. KI-003
Emergency operations center
Most of the stakeholders suggested having emergency operations centers that can help meet the requirement for routine reporting systems and facilitating early response.
Rapidly detect any foreseeable events and transparent sharing of the information and reports about outbreaks when they occur in the neighboring territories/states among all of the stakeholders and adjoining member states. Emergency operations centers can help meet this requirement through establishing routine reporting systems and facilitating response. Such quick detection, assessment, reporting can enhance the response and can help in preventing threats from crossing the borders. KI-008
Improving lab capacity
Many of the stakeholders recommended that the local lab capacity be improved in handling the emergencies and also with the required diagnostic equipment to strengthen these required capacities at this POE. It was mentioned regarding the operational difficulties that may be faced while sending samples to reference labs that are quite far from the POE.
Enabling the testing and procurement of vaccines and diagnostics at the health unit need to be strengthened to facilitate the required measures to contain the risks at the source itself. Improving the lab capacity required for the health unit. Strong commitment is required for strengthening the required capacities from the stakeholders and all of the ministries thereof. KI-006
Cross border meetings
Some of the stakeholders highlighted the importance of sharing information related to such public health events and suggested the need for cross border meetings.
In the cases of the medical tourism, prior information may be obtained online from the counterpart across the border; this point can be taken up with the authorities of the neighboring countries during cross border meetings. KI-007
DISCUSSION
Border health strategies minimize the risk of importation and exportation of disease through POEs, as well as across porous land borders.Reference Merrill, Rogers and Ward2 Airport and Border Quarantine (ABQ), Attari, is a subordinate office which looks after the POEs, including ICP Attari-Wagah-road border (ground crossing), Attari railway station, and Sri Guru Ram Das Jee International Airport, Amritsar. The designated ground crossing, ICP Attari, is the most populous ground crossing for travel and trade in India. Attari is almost mid-way between the 2 historical towns of Amritsar and Lahore in India and Pakistan, respectively.10 Most of the passengers using ICP, Attari for crossing the border are citizens from India and Pakistan. The main purposes for their visit are business, medical, religious, and tourism. Third country nationals also use this facility for entry into India or exit from India. The number of passengers crossing the border in either direction at Attari nearly amounts to 0.1 million.
Bi-regional multi-country expert workshops conducted to strengthen the capacity requirements for the IHR at ground crossings have revealed that some areas of IHR implementation in POE require more research, especially for vector control and coordination of non-health sectors. The workshop also indicated that insufficient human and financial resources have been dedicated to ensuring that states can effectively implement IHR at ground crossings. This workshop, however, also revealed the value of information exchange between experts of neighboring countries.11 Building and maintaining these open lines of communication between neighboring nations are critical for productively responding to disease and environmental issues that threaten to cross borders.Reference Merrill, Rogers and Ward2,Reference Cohen, Brown and Alvarado-Ramy3 It is essential that these meetings are followed up with similar events to allow experts to exchange their insights, build relationships, and identify areas for future improvements that can be incorporated into guidelines for IHR implementation, especially at ground crossings. A regional meeting on IHR (2005) core capacities at POE was held on June 26-28, 2013, at Kochi, India, to discuss progress, identify strengths and weaknesses and follow-up actions at national and regional levels to strengthen core national capacities made under the IHR (2005) at POE in member states.12 As per its report (2015), the designated ground crossing, ABQ, has not been assessed so far. Cross-border meetings for collaboration with neighboring countries were not held at designated Ground Crossing (GC), but have been held with Bangladesh, Bhutan, Nepal, and Sri Lanka on the issue of prevention of communicable diseases.12 Routine activities in terms of surveillance/coordination/communications take place at ABQ, Attari. A Public Health Emergency Contingency Plan (PHECP) has been developed but not pre-tested. As per the report, Myanmar has designated 5 ground crossings, among which 1 is Sagaing Region Tamu-More sharing its border with India, which were still under the process of IHR implementation.12
The stakeholders from various departments showed an understanding of the concepts and functionality of IHR (2005), and this allows the smooth implementation of the IHR (2005) at the ground crossing. Achieving international public health security has been one of the main challenges arising from the new and complex landscape of public health in WHO Member States. Shared vulnerability implies shared responsibility in Member States .13 The international public health security has relied on appropriate and timely management of public health risks that, in turn, depend upon effective national capacities, international, and intersectoral collaboration.14,15 Each area of work has a specific goal that contributes to the overarching goal for international public health security and subject to more detailed implementation plans. There is a paradigm shift from containment at source for public health threats to adapted response.13
Expert exchanges, national tabletop exercises, multi-sectoral workshops, and cooperative agreement collaborations facilitate the use of the IHR on a day-to-day, operational basis. The active participation of senior-level officials in these multi-sectoral and multinational capacity-building activities increases overall understanding of the benefits of IHR compliance and deepens political commitment to IHR implementation. Border health approaches can support strategies in the existing public health systems and infrastructure.Reference Cohen, Brown and Alvarado-Ramy3 The risk of international spread of diseases can be decreased through effective standing public health measures and response capacity at these designated airports, ports, and ground crossings in all countries.Reference Merrill, Rogers and Ward2 Similarly, the main aim of ABQ, Amritsar, is to prevent any infectious disease that is not prevalent in India, for example, yellow fever, severe acute respiratory syndrome (SARS), and Zika. Competent, equipped, and well-trained human resources are therefore essential to maintaining national capacity and preparedness and to ensuring that the IHR are functional. Human resources must be capable of providing public health surveillance and response across all levels and related sectors.
CONCLUSION
Our work has led us to conclude that the overall implementation status at the ground crossing, according to the assessment conducted using the WHO Tool, was achieved to be 76% overall. It has revealed certain areas that were not yet fully implemented, and the need for further strengthening of the implementation in those areas is required as per the IHR requirements for a designated ground crossing. Gaps that were identified included mainly the capacities to detect chemical, radiological and nuclear events, and shortage of regular staff. The WHO Tool also highlighted the current strengths and weaknesses. The study provided insights into various domains and the perceptions of the stakeholders and travelers regarding the current health services and handling the risks provided at ICP, Attari. There is lack of awareness among the travelers, which increases the risks of the import of diseases. This ground crossing being used by travelers from many nationalities for exit or entry to India, with many of the countries reporting travel-related cases of infectious diseases, introduces increased risk of importation or exportation of diseases. The coordination level among the stakeholders was well-established to ensure a quick response to any such risks. Capacity for isolation, quarantine, medical referral, and required vaccination has been developed. However, the lab capacity requirements need to be fulfilled to facilitate early detection at this POE, as well as mechanism for issuing early warnings taken up by the local authorities to mitigate the situation. Information needs to be shared among travelers to bring awareness regarding health risks while traveling. The information desk can provide leaflets regarding health risks related to travel. Current assessment of the only designated ground crossing from this study can support the development of a plan of action that addresses the identified gaps and improve the routine risk management, early warning and response systems to meet IHR requirements. This PoE can serve as an example for identifying and strengthening of other ground crossings in India.
Acknowledgments
We greatly appreciate the support of Dr Himanshu Chauhan DADG (IH) and Dr Sujeet K. Singh DDG (MH and IH), Directorate General of Health Services, Ministry of Health and Family Welfare, for granting the necessary permissions to conduct this study. Our sincere thanks to Dr Nicole J. Cohen, Deputy Associate Director for Science, Division of Global Migration and Quarantine, and Dr Rebecca D. Merrill, Global Border Health Team, US Centers for Disease Control and Prevention, for sharing their expertise and valuable insights in the field of Border Health.
This project would not have been possible without the support of Dr Surinder Pal Singh, Chief Medical Officer, and Dr Vinay Kumar Sukhija, Chief Medical Officer Airport and Border Quarantine, Attari, for informative discussions in the field of Border Health and support in facilitating meetings with all of the stakeholders at the ground crossing.



