


Introduction
Several types of sinonasal disease have been attributed to fungal pathogens. Fungal diseases of the paranasal sinuses are categorised as either invasive or non-invasive based on the presence or absence of tissue invasion. Fungus balls are extramucosal overgrowths of mycotic elements, which in the paranasal region are commonest in the maxillary sinus followed by the sphenoid sinus. Aspergillus species are the most commonly documented pathogens associated with the disease.Reference Grosjean and Weber 1 – Reference Costa, Polini, Zerman, Robiony, Toro and Politi 3 Most patients are either asymptomatic or present with non-specific complaints similar to those of chronic sinusitis.Reference Grosjean and Weber 1 , Reference Songu, Unlu, Gunhan, Ilker and Nese 2
We report an unusual case of a fungus ball in the concha bullosa without paranasal sinus involvement.
Case report
A 29-year-old woman was admitted to our clinic complaining of nasal obstruction and postnasal discharge for 10 years. She had a history of seasonal allergy symptoms. Several courses of antibiotics and anti-allergic drugs had been prescribed, but her symptoms had never resolved completely. She was otherwise healthy, and there was no clinical suspicion of immunodeficiency.
An endoscopic examination revealed a prominent right middle turbinate. It was covered with smooth mucosa and was hard on palpation. The nasal mucosa was normal and no pus was detected.
Computed tomography (CT) showed that the sinuses were clear, but identified a concha bullosa of the right middle turbinate filled with a high-density material (Figure 1).
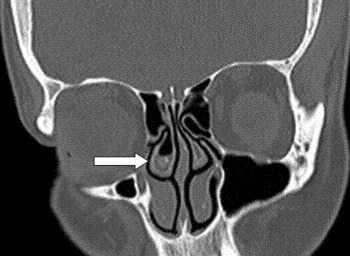
Fig. 1 Coronal computed tomography image showing the concha bullosa of the right middle turbinate filled with a high-density material (arrow).
The fungal material was removed via endoscopic resection. A vertical midline incision was made in the anterior part of the middle turbinate, and the lateral portion of the concha was then removed via an endoscopic transnasal approach. After removing the lateral portion, a dark brown, cheese-like material was aspirated from within the concha bullosa.
Histopathological examination of the excised specimen revealed aspergillosis (Figure 2).

Fig. 2 Photomicrograph of the excised specimen showing septated aspergillus hyphae (arrow).
The patient did not receive additional antifungal therapy, and there was no recurrence of disease post-operatively (Figure 3).

Fig. 3 Post-operative coronal computed tomography image showing absence of the fungus ball (arrow).
Discussion
Fungal infections are rare in otorhinolaryngology. However, an increasing number of fungal infections of the paranasal sinuses have been reported. This is attributed to improved diagnostic approaches to investigating the paranasal sinuses, and also to an increase in conditions that favour fungal infections, such as diabetes, long-term antibiotic and corticosteroid treatment, radiochemotherapy, immunosuppressive treatment, and diseases causing immunodeficiency. Fungus balls typically affect healthy individuals and exhibit a female predominance.Reference Costa, Polini, Zerman, Robiony, Toro and Politi 3
Fungus balls are usually found as an isolated collection in one sinus.Reference Lee, Yang and Kim 4 Although paranasal sinus involvement with mycotic infection is well known, a fungus ball in the concha bullosa is unusual, with only a few reported cases. Cukurova et al. reported one such case in a series of 31 cases of concha bullosa pathology, and suggested that this case was only the second to be reported.Reference Cukurova, Demirhan, Karaman and Yigitbasi 5 Of course, there may have been unreported cases.
The pathogenesis of fungal infections of the paranasal region is unclear. Hypoventilation could be important in trapping fungal spores and providing anaerobic conditions for fungus ball development.Reference Lee, Yang and Kim 4 The concha bullosa has a mucociliary transport system which connects the aerated cell to the frontal recess, lateral sinus or hiatus semilunaris, via the ostium.Reference Okuyucu, Akoğlu, Dağli and Concha bullosa 6 , Reference Unlü, Akyar, Caylan, Nalça and Concha 7
Initially, we thought that obstruction of the ostium and inflammatory changes within it might have led to our patient's mycotic infection; however, the ostium of the concha bullosa did not appear obstructed in the CT images. Our patient had previously been prescribed several courses of antibiotics and anti-allergic drugs, and these may have acted as predisposing factors contributing to the aetiology of her condition.
Computed tomography is the most common method of diagnosing fungal infections, as it is for other types of sinonasal pathology. The most common CT appearance of fungus balls is partial or complete, heterogeneous opacification of the involved sinus, often with calcified material.Reference Grosjean and Weber 1 , Reference Songu, Unlu, Gunhan, Ilker and Nese 2 , Reference Robey, O'Brien, Richardson, Baker, Poage and Leopold 8 , Reference Lee 9 The next most common CT finding is thickening or erosion of the bony sinus wall.Reference Robey, O'Brien, Richardson, Baker, Poage and Leopold 8 In our patient, a high-density, heterogeneous material filled the right middle turbinate.
-
• Paranasal sinus fungus balls most commonly involve the maxillary and sphenoid sinuses
-
• A fungus ball in the concha bullosa is presented, without paranasal sinus involvement
-
• Surgery is the advised management for sinus fungus balls
The diagnosis of fungus ball is based on identification of characteristic macroscopic and microscopic features. Macroscopically, fungus balls are characterised by grumous, friable, cheese-like material that can be green, yellow, brown or black and is easily peeled off the mucosa. Microscopically, there is an aggregate of tightly packed hyphae.Reference Grosjean and Weber 1 , Reference Songu, Unlu, Gunhan, Ilker and Nese 2 In our patient's case, the excised specimen showed septated aspergillus hyphae on periodic acid Schiff staining. Positive fungal cultures are reported in only 20–50 per cent of patients, probably due to the poor viability of fungal elements in fungus balls.Reference Grosjean and Weber 1 , Reference Lee 9 In our case, fungal culture of the excised material was negative, probably for this same reason.
Surgery of paranasal fungus balls is generally curative, and no local or systemic antifungal therapy is required.Reference Grosjean and Weber 1 Transnasal endoscopic surgery is the preferred approach due to its rapid recovery time, minimal complications and short hospitalisation period.Reference Lee 9
Conclusion
Although rare, fungus balls should be considered in the differential diagnosis of middle turbinate and sinonasal pathology. Surgery remains the primary treatment. Nasal endoscopic inspection should be performed during post-operative follow-up visits.



