Introduction
Hearing impairment is the most common chronic sensory disorder in adults worldwide.Reference Nash, Cruickshanks, Klein, Klein, Nieto and Huang1 Population-based epidemiological prevalence estimates range from 14.1 to 20.6 per cent in middle-aged adults, and up to 90 per cent in adults older than 80 years.Reference Nash, Cruickshanks, Klein, Klein, Nieto and Huang1–Reference Agrawal, Platz and Niparko3 Hearing impairment is known to cause social and emotional problems that disrupt patients' quality of life (QoL).Reference Cruickshanks, Wiley, Tweed, Klein, Klein and Mares-Perlman2, Reference Baumann, Gerendas, Plinkert and Praetorius4, Reference Monzani, Galeazzi, Genovese, Marrara and Martini5 Problems such as emotional issues, reduced social activities and increased difficulty in daily activities are thought to be three- to fivefold more common in deaf people compared with normally hearing people.Reference de Graaf and Bijl6, Reference Fellinger, Holzinger, Dobner, Gerich, Lehner and Lenz7 Outward indications of deafness have been noted to cause various emotional and social reactions in others.
It is reasonable to anticipate that communication problems related to deafness may also affect a person's sexual function. We propose that hearing loss may be a causal factor in the development of erectile dysfunction, defined as the inability to achieve and maintain an erection sufficient for satisfactory sexual intercourse.Reference Esposito and Giugliano8 Similar to hearing loss, erectile dysfunction is a common disorder, especially in older men.Reference Johannes, Araujo, Felman, Derby, Kleinman and McKinlay9 The aetiology of erectile dysfunction includes physiological, psychological and organic causes.Reference Esposito and Giugliano8
To date, only a few reported studies have investigated ear disorders as a potential organic causal factor for erectile dysfunction. The impact of Ménière's disease and tinnitus on sexual health has been previously investigated.Reference Zapata and López-Escámez10, Reference Muluk, Başar, Oğuztürk and Dikici11 However, to our knowledge the effect of deafness per se on erectile function has not been studied, nor are we aware of any research investigating the influence of hearing impairment on general sexual health.
Clinicians have recognised that hearing impairment is a multifaceted condition with many medical and social aspects; however, it would seem that the relationship between hearing loss and sexual health remains unstudied.
To our knowledge, the current study is the first reported research examining sexual health, including erectile dysfunction, in patients with hearing loss. This study used the International Index of Erectile Function questionnaire to assess the sexual health of men with acquired, bilateral, sensorineural hearing loss (SNHL), and compared the results with those for healthy men. We also investigated whether high-level hearing loss had any additional negative effect on sexual function.
Materials and methods
Study design
This study was designed as a prospective case–control study. It was conducted in collaboration with the ENT department and urology clinic of our institution.
Institutional ethics committee approval was obtained (permit number 2010/186). The study was conducted in accordance with the Declaration of Helsinki, as amended in 2008. Written, informed consent was obtained from all participants.
Demographic data were recorded for all participants, including age, body mass index (BMI), educational status, marital status and number of children.
Selection of patients and healthy control subjects
The hearing loss group comprised men with acquired, bilateral SNHL of more than one year's duration, who fulfilled the inclusion criteria.
The inclusion criteria were: aged 18 years or older; mild, moderate or moderately severe SNHL; literate; married; able to complete the study forms; and having full legal capacity.
The exclusion criteria were: aged below 18 years; severe or profound SNHL; lack of full legal capacity; widowed or unmarried; and female. Additional exclusion factors included: BMI of 30 kg/m2 or more; sexual disorder(s) in the patient's spouse; psychiatric disorders or use of psychiatric medication; chronic drug use for erectile dysfunction or any other disease; any additional systemic or chronic disease apart from hearing loss; miscommunication due to deafness; prelingual hearing loss; acute hearing loss; newly or successfully treated sudden hearing loss; unilateral SNHL due to causes such as chronic suppurative otitis media, chronic non-suppurative otitis media or otosclerosis; use of a hearing device; a history of ear or urinary tract surgery; and refusal to participate in the study.
The control group comprised healthy, adult, married men who were demonstrated to have normal hearing levels. The control group was selected with consideration to achieving a similar distribution of gender, BMI and age.
Data collection took place between September 2010 and December 2011.
Hearing assessment
Definitive diagnosis of hearing impairment primarily involved clinical examination and audiological testing in the ENT clinic.
Clinical examination included a careful and detailed history, general ENT examination, otoscopic evaluation and hearing assessment. Subjective hearing was assessed with a tuning fork.
All participants underwent objective hearing assessment using pure tone audiometry (PTA) conducted within a soundproof booth, according to the guidelines of the American Speech-Language-Hearing Association.12 Pure tone air-conduction thresholds were obtained for each ear at 500, 1000, 2000, 3000, 4000, 6000 and 8000 Hz. Bone-conduction thresholds were measured at two frequencies at baseline (500 and 4000 Hz) and three at follow up (500, 2000 and 4000 Hz). Hearing loss was defined as the presence of PTA hearing thresholds of greater than 15 dBHL at 500, 1000, 2000 and 4000 Hz.
The duration and severity of auditory impairment were also recorded.
After ENT examination, patients were referred to the urology department for an assessment of their sexual function.
Assessment of sexual function
Sexual function, including the presence or absence of erectile dysfunction, was assessed using the International Index of Erectile Function questionnaire. This questionnaire has been widely used to evaluate male sexual function in general and erectile dysfunction in particular. It consists of 15 items grouped into 5 sexual function domains: erectile function (six questions); orgasmic function (two questions); sexual desire (two questions); sexual intercourse satisfaction (three questions); and overall satisfaction (two questions).Reference Rosen, Riley, Wagner, Osterloh, Kirkpatrick and Mishra13 Each question was scored from 1 to 5. As shown in Table I, the individual scores in each domain were rated to indicate the degree of clinical dysfunction; rating numbers were defined as follows: 5 = no dysfunction, 4 = mild dysfunction, 3 = mild-to-moderate, 2 = moderate and 1 = severe. The dysfunction severity rating scale was the same for all domains, although the individual score ranges assigned to each rating number differed between domains (Table I). Lower question scores corresponded to higher degrees of dysfunction, while higher scores reflected healthier sexual function. All questions referred to the past four weeks.
Table I Clinical dysfunction rating of iief domain scores

Participants were informed about the questionnaire in advance, and questions were answered confidentially over a period of 30 minutes. Men who did not complete the questionnaire were excluded from statistical analysis.
Assessment of health-related quality of life
The Medical Outcomes Study 36-Item Short-Form Health Survey, a widely used and self-reported scale, was administered to assess participants' perceived general health status. This questionnaire has previously been used successfully to evaluate patients with medical or psychological disorders as well as healthy subjects. The questionnaire assesses both positive and negative aspects of health, and is regarded as sensitive to small changes in disability status. It assesses QoL in eight domains, namely physical functioning, physical role difficulty, bodily pain, general health perception, vitality, social functioning, emotional role difficulty and mental health. Each dimension score is standardised and ranges from 0 to 100, with higher scores reflecting better QoL. The questionnaire has previously been used with patients with Ménière's disease and benign paroxysmal positional vertigo.Reference Zapata and López-Escámez10, Reference López-Escámez, Gamiz, Fernández-Pérez and Gómez-Fiñana14
Statistics
Statistical evaluation was carried out using SPSS software (version 15.0; IBM, Armonk, New York, USA). Normally distributed continuous variables in both groups were tested using Student's t-test. The Mann–Whitney U test was used to compare continuous variables for which data were not normally distributed. Comparisons of categorical variables were made using the chi-square test. P values of less than 0.05 were considered to indicate statistical significance.
Results
A total of 76 adult, male subjects were enrolled in the present study (mean age ± standard deviation (SD), 35.9 ± 8.2 years). All subjects were married and were sexually active. The study group consisted of 36 patients with acquired, bilateral SNHL. The study group mean age ± SD was 37.8 ± 8.7 years (range, 25–57 years). The control group consisted of 40 healthy volunteers with a mean age ± SD of 34.3 ± 7.5 years (range, 24–55 years). The two groups were statistically similar in terms of age (p = 0.059), body mass index (p = 0.598), duration of marriage (p = 0.181), duration of education (p = 0.087) and number of children (p = 0.511). Demographic data for both groups are shown in Table II.
Table II Demographic results

Patient data are given as means ± standard deviations. *n=36; †n = 40. HL = hearing loss; y = years; BMI = body mass index; durn = duration
Table III summarises both groups' results for the 36-Item Short-Form Health Survey. Scores for physical function, bodily pain, general health perception, vitality, emotional difficulty and mental health did not differ significantly between the two groups. However, hearing loss patients had poorer scores for the social functioning and physical role difficulty domains, compared with controls.
Table III Quality of life scores*

* 36-Item Short-Form Health Survey scores, given as means ± standard deviations. *n=36; †n = 40. ‡Significant difference between the two groups. HL = hearing loss
Table IV compares the two groups' results for the International Index of Erectile Functions questionnaire. The hearing loss group had significantly lower scores for all five domains, i.e. erectile function (p < 0.001), orgasmic function (p = 0.004), sexual desire (p = 0.011), intercourse satisfaction (p = 0.007) and overall satisfaction (p < 0.001), as well as a significantly lower total score (p < 0.001), compared with the control group.
Table IV Sexual function scores*

* International Index of Erectile Functions questionnaire (IIEF) scores, given as means ± standard deviations. †n = 36; ‡n = 40. **Significant difference between the two groups. HL = hearing loss
Table V shows the distribution of the hearing loss and control subjects according to their degree of clinical dysfunction as per the five International Index of Erectile Functions questionnaire domains, as calculated by domain scores. No subjects in either group had severe dysfunction, in any domain; likewise, none had moderate dysfunction except in the case of sexual desire. The prevalence of mild and mild-to-moderate sexual dysfunction was generally found to be significantly higher in the hearing loss group, especially for the erectile function, intercourse satisfaction and overall satisfaction domains, compared with the control group.
Table V Severity of sexual dysfunction by iief domain

*Significant difference in domain results between the two groups. IIEF = International Index of Erectile Functions questionnaire; HL = hearing loss
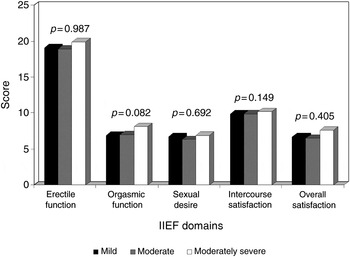
The hearing loss subjects had suffered from bilateral SNHL for a mean ± SD duration of 16.5 ± 7.8 years (range, 4–28 years). Hearing loss was mild in 13 (36.1 per cent) patients, moderate in 15 (41.7 per cent) and moderately severe in eight (22.2 per cent), according to the American Speech-Language-Hearing Association guidelines. When the SNHL patients were grouped according to the severity of their hearing loss (i.e. mild, moderate or moderately severe), no statistically significant differences in results were seen for any of the five International Index of Erectile Functions questionnaire domains (Figure 1).

Fig. 1 Patients' International Index of Erectile Functions questionnaire domain scores by degree of hearing loss.
Discussion
Both SNHL and erectile dysfunction are common, and much research has been published on each topic separately. However, surprisingly, the effects of hearing loss on sexual health has been neglected in the literature and very little is known. However, there have been some recent reports.Reference Zapata and López-Escámez10, Reference Muluk, Başar, Oğuztürk and Dikici11 One study investigated the effects of tinnitus, and found that tinnitus patients became accustomed to living with their disease, and that loss of sexual performance was not observed over the long term.Reference Muluk, Başar, Oğuztürk and Dikici11 Zapata and López-Escámez evaluated sexual health in patients with Ménière's disease, and suggested that this condition may be associated with erectile dysfunction in men.Reference Zapata and López-Escámez10 Similarly, our results indicate that deafness adversely affects men's sexual function. Our hearing loss patients had poorer scores for all domains of the International Index of Erectile Functions questionnaire; indeed, they showed twice the prevalence of erectile dysfunction compared with control subjects (Table V).
Although hearing problems increase dramatically with age, hearing impairment is not an uncommon condition in middle-aged adults.Reference Nash, Cruickshanks, Klein, Klein, Nieto and Huang1, Reference Tambs15 Tambs found that hearing loss had a moderate effect on mental health in young and middle-aged people, and a negligible effect in elderly people.Reference Tambs15 However, this does not mean that age-related hearing loss should be ignored, because it is a major public health issue. It would appear that elderly people accept their hearing loss more readily because it is considered to occur normally with ageing.
Similarly, it can be argued that the subjective effects of sexual dysfunction related to hearing loss may be more severe in young and middle-aged people than in elderly people. The present study included only young and middle-aged men, because elderly men are known to have many other risk factors for erectile dysfunction (in addition to old age), such as metabolic syndrome, hypertension and diabetes.Reference Nash, Cruickshanks, Klein, Klein, Nieto and Huang1, Reference Gündüz, Gümüs and Sekuri16
Additionally, epidemiological studies suggest that obesity (i.e. a BMI of 30 kg/m2 or more) is associated with an increased risk of erectile dysfunction.Reference Esposito and Giugliano8 To preclude the added adverse effects of obesity, and to limit our assessment solely to the impact of hearing loss, our study included only healthy young and middle-aged adults with a BMI of less than 30 kg/m2.
This study assessed health-related QoL with a widely used and validated instrument, the Medical Outcomes Study 36-Item Short-Form Health Survey. This questionnaire has been widely used to study the outcome of chronic disease.Reference López-Escámez, Gamiz, Fernández-Pérez and Gómez-Fiñana14 Our results indicated that hearing loss patients had poorer QoL scores only for the social functioning and physical role difficulty domains of this questionnaire, compared with controls (Table III); there were no significant differences for other domains, i.e. physical functioning, bodily pain, general health perception, vitality, emotional role difficulty and mental health. These results suggest that our hearing loss patients did not suffer serious psychiatric problems, in contrast with some previous studies. Other reports have suggested that hearing loss may impair patients' QoL.Reference Baumann, Gerendas, Plinkert and Praetorius4, Reference de Graaf and Bijl6 However, these authors' study populations differed from ours in terms of severity of hearing loss, i.e. they included mostly subjects with severe hearing loss. Our study did not include patients with hearing loss worse than moderately severe, as specified in our inclusion and exclusion criteria.
Our hearing loss patients' scores for the various domains of the International Index of Erectile Functions questionnaire did not differ according to patients' degree of hearing loss, i.e. patients with moderately severe hearing loss did not have significantly different sexual function results to those with mild or moderate hearing loss (Figure 1). This indicates that the severity of hearing loss was not closely associated with sexual function. However, when interpreting this result it should be kept in mind that our findings compared only the categories of mild, moderate and moderately severe hearing loss.
Although the present study's small sample size does not permit generalisation of our results, our observation of a relationship between hearing loss and sexual health should not be ignored. We acknowledge that our study's lack of patients with conductive hearing loss, mixed hearing loss or severe SNHL may represent a further limitation that should be taken into account when interpreting our results.
• The effect of general hearing loss on sexual health has not previously been assessed
• This study assessed sexual function and quality of life in young and middle-aged men with bilateral sensorineural hearing loss
• Patients had poorer sexual health than normal-hearing controls
Further studies are needed in order to understand the sexual function of patients with severe versus mild to moderate hearing loss, and also to investigate this association in middle-aged versus elderly adults. Future studies should also consider the effects of postlingual versus prelingual hearing loss, and the effects of using hearing devices.
Conclusion
Men with bilateral SNHL seem to have poorer sexual health, compared with healthy, normal-hearing men. The role of hearing loss in the deterioration of sexual function should be kept in mind.
Acknowledgements
The authors thank Yılmaz Palancı, Assistant Professor, Department of Public Health, Dicle University School of Medicine, for his valuable statistical assistance.