Identifying healthcare practices of uncertain effectiveness and reducing costs without compromising quality of care have become a focus of many healthcare systems (Reference Pearson and Littlejohns1–Reference Watt, Hiller and Braunack-Mayer3). This involves the assessment and prioritization of new and existing health technologies that may consequently lead to investment or disinvestment. The latter, defined as the partial or complete withdrawal of ineffective existing healthcare practices (Reference Elshaug, Hiller, Tunis and Moss2), can be challenging because clinical, political, and other barriers may oppose the proposed change. In this study, disinvestment relates to the partial withdrawal of an existing health technology. The high level of evidence, within accepted hierarchies of research design (4), expected for disinvestment decisions can be disproportionate to the paucity of evidence under which use of the technology was initially funded and/or currently defended. While there is no one universally accepted hierarchy, randomized controlled trials (RCTs) are considered to be the design least susceptible to bias. In this analysis, we present a case study that focuses on vitamin B12 (cobalamin) deficiency among adult patients newly presenting with unexplained fatigue in general practice to demonstrate how disinvestment can be recommended even with insufficient high-level evidence.
Population prevalence estimates of vitamin B12 deficiency range from 1.5 percent to 20 percent (Reference Lindenbaum, Rosenberg, Wilson, Stabler and Allen5–7), with higher prevalence in people older than 65 years. The diagnostic accuracy of tests currently used to diagnose deficiency has been repeatedly questioned and deemed unreliable (7–Reference Solomon9). Consequently, the true prevalence of cobalamin deficiency in the general population is unknown (Reference Stabler6). The under- or over-estimation of cobalamin deficiency is likely due to the different cut-points used in clinical practice along with the relatively nonspecific clinical manifestations of this condition (Reference Stabler6). For example, some of the reported nonspecific symptoms are identical to those associated with chronic fatigue and fibromyalgia, including exhaustion, difficulty in maintaining balance, depression, insomnia, muscular soreness, and numbness or tingling in hands and feet (Reference Gallagher, Thomas, Hamilton and White10;Reference Sharpe and Wilks11). For that reason, dieticians often recommend vitamin B12 supplements to treat unexplained symptoms of fatigue (Reference Werbach12).
Approximately one-sixth of primary care visits occur for unexplained symptoms for which no somatic pathology is apparent (Reference Rolfe and Burton13). Such unexplained symptoms with low pretest probability of serious disease pose a dilemma for clinicians whether to order diagnostic tests and if so, which tests (Reference Kassirer and Milstein14). Of all symptoms, fatigue is the most commonly presented (Reference Kenter, Okkes, Oskam and Lamberts15–Reference Britt, Miller and Charles17). In the United Kingdom, doctors classify approximately 12 new presentations of “malaise, fatigue, debility, and tiredness” per 1,000 patients seen in 1 year, with total annual consultation rates for fatigue at 18 per 1,000 (16). In Australia, fatigue/tiredness is the fifth most common problem associated with pathology testing. In 2010/11, in more than 65 percent of all Australian general practitioner (GP)-patient encounters for fatigue, a decision was made to order at least one pathology test; often multiple tests were ordered with a rate of 387.6 laboratory tests per 100 tested encounters (Reference Britt, Miller and Charles17). These routinely ordered batteries of pathology tests that are ordered to aid in diagnosis include the serum vitamin B12 test whose ordering has increased rapidly in Australia, the United Kingdom, and other developed countries, observed in all age groups (Reference Kenter, Okkes, Oskam and Lamberts15–19).
The paucity of high level evidence of cobalamin deficiency among the fatigued relates mainly to the lack of diagnostic and treatment guidelines, the uncertainty regarding the prevalence of the condition together with the uncertain natural medical history of patients with borderline deficiency. Similarly, the quality of life measures associated with the diagnosis or misdiagnosis of cobalamin deficiency have not been reported to date. Because empirical data on this study population are not available, using best available evidence, we conducted a 3-month incremental cost-effectiveness analysis comparing five diagnostic/therapeutic strategies in adult patients hypothetically presenting with a new episode of unexplained fatigue in general practice using Australian cost input metrics. A complaint was considered new if it had not been presented to the GP within the previous 6 months (Reference Koch, van Bokhoven and ter Riet18). The first consultation was considered and all screening tests that could have been ordered on the first consultation—other than serum cobalamin—were not included. A favorable outcome was to correctly diagnose and treat cobalamin deficiency within 3 months of first consultation.
This project was conducted as a component of the ASTUTE Health Study (Reference Watt, Hiller and Braunack-Mayer3;Reference Willis, Elshaug and Milverton8), examining disinvestment as a policy approach to healthcare safety and quality improvement and highlighting evidence challenges in supporting such a policy.
METHODS
Literature Search
A literature search, restricted to the English language, was performed using Medline / PubMed (1990-) and Embase (1990-) to identify peer-reviewed published studies on: (i) diagnosis and treatment of cobalamin deficiency, and (ii) prevalence and management of unexplained fatigue in general practice. We also conducted a systematic search to find guidelines on the management of unexplained fatigue in the general practice setting. The structured search was done for both keywords only and keywords with medical subject headings (MeSH) including the following terms: Tiredness OR fatigue OR lethargy OR weakness OR exhaustion, AND (general practice OR primary care). For this topic, we only targeted Australia and other closely related health systems (New Zealand, Europe, and Canada). Australian government reports were also searched.
All disease-related fatigue, mental- and emotional-related, injury-related, work-related conditions, and studies including children (ages 17 or younger) were excluded.
Diagnostic Pathology Test
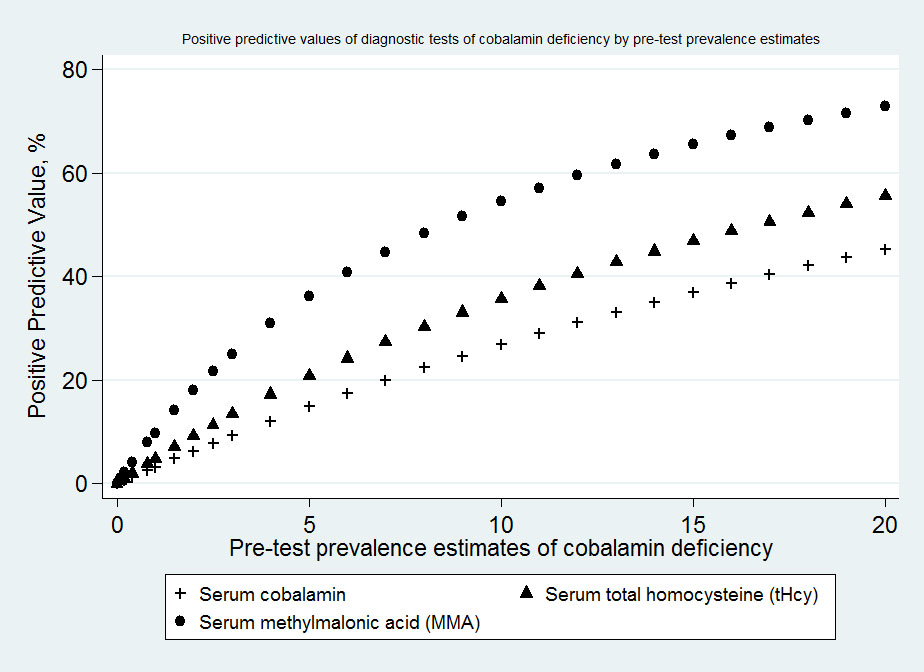
Available pathology tests that diagnose cobalamin deficiency include serum cobalamin, serum methylmalonic acid (MMA), serum total homocysteine (tHcy), and serum holo-transcobalamin (holo-TC) (Reference Lindenbaum, Rosenberg, Wilson, Stabler and Allen5–Reference Solomon9). Of all four tests, we chose to investigate serum cobalamin because it is the most accessible and most commonly used diagnostic test (Reference Stabler6;7). Our choice was supported by the substantial rise in per capita rate of claiming for Medicare Benefits Schedule (MBS) items ordered to diagnose cobalamin deficiency. Over a period of 14 years, the usage of MBS item 66602 (serum B12 and red cell folate and, if required, serum folate) rose from 926 tests per 100,000 population in 2000 to 9,575 tests per 100,000 population in 2013 (Supplementary Document 1) (19). In 2013, approximately 2.9 million pathology tests (either MBS item 66602 or 66599 [serum B12 or red cell folate and, if required, serum folate]) were ordered in Australia incurring more than USD100 million to the health system in an approximate population of 23 million (19). Most of these tests (approximately 91 percent) were ordered once per patient per year indicating that they were being undertaken for the purpose of screening/diagnosing rather than monitoring (Reference Britt, Miller and Charles17). This rise in usage was not deterred by the test's relative low positive predictive value as compared to the other more sensitive diagnostic tests as demonstrated in Supplementary Document 2.
The sensitivity and specificity of the serum cobalamin test were respectively set at 0.73, 95 percent confidence interval (CI), 0.38–0.92 and 0.78, 95 percent CI, 0.36–0.96, as reported in a meta-analysis of studies that used clinical reference as the criterion standard (Reference Willis, Elshaug and Milverton8). Because the prevalence of vitamin B12 deficiency is not known in patients presenting with unexplained fatigue, we used several plausible prevalence levels that were based on the Centers for Disease Control and Prevention estimates (7) and other epidemiological studies (Reference Lindenbaum, Rosenberg, Wilson, Stabler and Allen5;Reference Solomon9). Using these sensitivity and specificity measures we estimated the true positive (TP), the false negative (FN), the true negative (TN), and the false positive (FP) values of the test.
Eligible Population and Comparator Strategies
We defined the eligible population as adult persons (18 years of age or older) newly presenting in general practice with fatigue whose symptoms could not be explained by medical assessment and who had a low pretest probability of serious illness. The first consultation was considered and all screening tests that could have been ordered on the first consultation—other than serum cobalamin—were not included in this economic evaluation. Conditions that are most commonly associated with unexplained fatigue, for which various pathology tests could be ordered, include anemia, infection, autoimmune disease, cancer, diabetes, hypothyroidism, hypoadrenalism, multiple sclerosis, obstructive sleep apnea, pregnancy, and organ disease, for example, liver, kidney, heart, or lung (Reference Sharpe and Wilks11).
The five mutually exclusive diagnostic-therapeutic strategies examined were the following: Strategy 1: order serum cobalamin pathology test and treat accordingly with hydroxocobalamin intramuscular (IM) injections; Strategy 2: order serum cobalamin pathology test and treat accordingly with oral crystalline cyanocobalamin supplements; Strategy 3: do not test, but treat all with hydroxocobalamin IM injections; Strategy 4: do not test, but treat all with oral crystalline cyanocobalamin supplements; Strategy 5: do not test and do not treat, if symptoms continue, reassess after a period of 3 months.
Management Algorithm and Decision Tree
The natural history and management pathways for patients presenting with unexplained fatigue due to cobalamin deficiency are unknown. We therefore used best available evidence to construct a plausible management algorithm for our patient population. The algorithm, presented in Supplementary Document 3, was based on guidelines from Canada (Reference Godwin, Delva and Miller20), The Netherlands (Reference Kenter, Okkes, Oskam and Lamberts15), and New Zealand (21). The Canadian Family Practice Guidelines Development Group recommends a limited number of pathology tests in adult patients with fatigue only for those over 65 years of age, or younger patients with specified risk factors for certain conditions (Reference Godwin, Delva and Miller20). The Best Practice Advocacy Centre (BPac) New Zealand guidance recommends testing by risk groups (21) while the Dutch College of General Practitioners (DCGP) recommends postponing tests until patients are reviewed a month after initial presentation, and they recommend a restricted set of tests including full blood count (FBC), erythrocyte sedimentation rate (ESR), thyroid function tests (TFTs) and glucose (Reference Kenter, Okkes, Oskam and Lamberts15). Our management algorithm was supplemented by expert opinion (clinical co-authors Metz and Frank plus an external clinical expert).
Informed by the guidelines-supported management algorithm, we constructed a decision tree (Table 1) to compare the five study strategies. The tree depicts the presence or absence of cobalamin deficiency together with the study diagnostic and therapeutic strategies to represent the following clinical outcomes at the terminal nodes: (i) cobalamin deficient, correctly treated; (ii) non-cobalamin deficient, erroneously treated; (iii) cobalamin deficient, untreated; and (iv) non-cobalamin deficient, correctly ruled out.
Table 1. Decision Tree for Diagnostic/Therapeutic Strategies for Cobalamin-Deficiency Fatigue

b Estimated using cobalamin deficiency prevalence of 10 percent.
We limited the study horizon to 3 months assuming that correctly diagnosed and treated cobalamin-deficiency-fatigue would typically resolve within 3 months (Reference Nijrolder, van der Horst and van der Windt22). Non-cobalamin-deficient patients who are falsely identified as cobalamin deficient (test false positives) or those treated without testing may incur a delay in the identification of the true cause of their fatigue. In the absence of reliable data on the clinical pathways for these patients, it was assumed that resolution of symptoms would be delayed by 3 months. For the nontreated cobalamin deficient patients (the FNs in the “test and treat” strategy and the cobalamin deficient in the “do not test, do not treat” strategy), it was assumed these patients would be referred to a medical specialist to continue the evaluation of the unexplained fatigue and the treatment with B12 supplements would commence after 3 months.
Efficacy Measure and Treatment
Fatigue is accompanied by diverse symptoms: discomfort, anxiety, pain, and problems performing usual activities may be the most predominant (Reference Gallagher, Thomas, Hamilton and White10). We used the EuroQol-5D (EQ-5D) multi-attribute utility instrument to assign utility scores for each of the four 3-month endpoints listed above based on various stages in the diagnostic-therapeutic process (Reference Brooks23). We chose EQ-5D because this tool has been used to describe health-related quality of life among those with fatigue or fatigue-related conditions in primary care settings as reported by Richardson et al. (Reference Richardson, Epstein and Chew-Graham24). Table 2 illustrates the calculation of the utility scores, which was based on the assignment of levels for each of the five EuroQol-5D attributes (mobility, self-care, usual activity, pain/discomfort, and anxiety/depression) to each endpoint. We used the systematic review on fatigue prognosis (Reference Nijrolder, van der Horst and van der Windt22), together with expert opinion, to suggest different scenarios relating to fatigue symptoms in our 3-month study period. For the untreated and erroneously treated patient endpoints, we assumed three possible scenarios: (i) deterioration in symptoms, (ii) improvement in symptoms, or (iii) no change in symptoms by the end of the 3 months (Reference Nijrolder, van der Horst and van der Windt22).
Table 2. Description of Assumed Utility Scores by EuroQol-5D Health State

Note. Examples of estimation of utility score per scenario: The overall score for the 3-month period for a patient who had cobalamin deficiency and who was properly treated is: [0.5(0.689+0.76) + 0.5(0.76+0.883) + 0.5(0.883+1)] / 3 = 0.829. For all other patients whose symptoms of fatigue were not resolved by the treatment strategy, the baseline and 3-month utility scores were assumed to: (i) remain stable (i.e., utility score = 0.689), (ii) deteriorate by an assumed 10% of the initial starting utility score, or (iii) improve by an assumed 10% of the initial starting utility score.
The Centers for Disease Control and Prevention (CDC) treatment recommendations were adopted (7). IM or subcutaneous crystalline cobalamin is currently the standard treatment option (Reference Stabler6). This parenteral route includes the weekly administration of 1 milligram (1,000 μg) hydroxocobalamin for 8 weeks followed by once monthly. The alternative and increasingly supported oral regimen includes 1 milligram (1,000 μg) crystalline cyanocobalamin consumed daily (Reference Stabler6;Reference Lederle25;Reference Seal, Metz, Flicker and Melny26). Intranasal treatment is uncommon and thus not represented here. The oral and the parenteral regimens were assumed to be equally effective (as indicated in a systematic review of randomized controlled trials) (Reference Butler, Vidal-Alaball and Cannings-John27), safe, and well tolerated by patients (7;Reference Seal, Metz, Flicker and Melny26;Reference Butler, Vidal-Alaball and Cannings-John27). The water-soluble vitamin B12 is also considered safe at levels much higher than the recommended dose (7), even in geriatric patients as shown by Seal et al. randomized controlled trial (Reference Seal, Metz, Flicker and Melny26). We assumed full compliance, gradual relief of symptoms over time (Reference Nijrolder, van der Horst and van der Windt22), and that treatment started 1 week after the blood test was ordered in those whose test indicated a deficiency.
Costs
We included the Australian costs associated with the diagnosis and treatment of cobalamin deficiency, including Medicare Benefits for GP consultations, cobalamin serum pathology tests, and Patient Episode Initiation (PEI) paid to pathology practices for specimen collection, and parenteral and oral treatment fees (19;28). All above listed fees and costs are subsidized by Medicare Australia or the Australian Pharmaceutical Benefits Scheme (PBS), except for oral vitamin B12 supplements which are available over-the-counter without prescription. Discounting of costs and effects was unnecessary, because the time horizon did not exceed 1 year. All costs are full Medicare Benefits Scheme (MBS) fees and are in American dollars. The 31 December 2013 American to Australian dollar exchange rate was used (i.e., USD 1 = AUD 0.8931). The unit costs of the health services used are presented in Table 3.
Table 3. Unit Costs of Healthcare Services

Note. Bases on 2013 prices.
a Patients with a pathology test ordered will have to consult with their GP twice: once when the test is ordered and the second time to plan the intervention based on the test results. Therefore, such patients are assumed to pay this fee twice (i.e., USD 93.4)
b Based on 31 December 2013 American dollar: Australian dollar exchange rate of USD 1 = AUD 0.8931.
Economic Analysis
In the base-case analysis, GP consultation costs were assumed to be equal across all strategies. Expected costs and expected utility scores were calculated for all five diagnostic-therapeutic strategies at a 10 percent cobalamin deficiency prevalence level. We then ranked all five strategies according to increasing cost and eliminated strategies by using simple dominance (i.e., strategies that were less effective and more costly) and extended dominance (i.e., strategies with an incremental cost-effectiveness ratio (ICER) that was greater than that of a more effective strategy) (Reference Drummond, Sculpher, Torrance, O’Brien and Stoddart29). Of the remaining strategies, ICERs are reported for each strategy relative to the next less costly strategy. Using similar methods as reported by Evans et al. (Reference Evans, Boan, Evans and Shuaib30), we calculated subtotals summing up each mutually exclusive diagnostic/treatment strategy. Expected values were based on the summation of the pathway values weighted by the pathway probabilities.
Sensitivity Analysis
A probabilistic sensitivity analysis (PSA) was performed to represent uncertainty in the sensitivity and specificity, cost, and utility model input parameter values. The means and upper and lower estimated values for the cost and utility score parameters, together with the confidence intervals of the sensitivity and specificity measures informed probability distributions for the respective parameters in the PSA. Because the prevalence of cobalamin deficiency is unknown, we conducted 1,000 Monte Carlo simulations at cobalamin deficiency prevalence levels of 1 percent, 5 percent, 10 percent, and 20 percent. For each simulation, the probabilities and utility scores were sampled from defined beta distributions, while for the range of cost estimates we used a discrete uniform distribution. From the conducted simulations, a cost-effectiveness acceptability curve was derived to give an estimate of the proportion of the posterior sampled distributions of costs and quality-adjusted life-years (QALYs) in which each strategy was identified as the most cost-effective strategy, given alternative monetary values of a QALY gained. Similarly, we conducted one way sensitivity analyses to assess the individual effects of uncertainty in each of the parameters. Supplementary Document 4 lists the main study assumptions together the respective level of evidence based on the Australian National Health and Medical research Council (NHMRC) guidelines (4).
The analyses were conducted using Excel (Microsoft) and Stata (version 12, StataCorp, College Station, TX).
RESULTS
Table 1 shows the expected costs, utilities and incremental cost per QALY of the five mutually exclusive diagnostic/therapeutic strategies with a 10 percent prevalence of cobalamin deficiency. Among the strategies, not testing and not treating was the reference strategy as it had the lowest costs and QALY gains. Strategies involving intramuscular injections were dominated, that is, cost more and gained fewer QALYs than at least one other strategy. The strategy of testing and treating with oral supplements was dominated by extended dominance. (Extended dominance occurs when a strategy has an incremental cost-effectiveness ratio greater than that of a more effective competing strategy.) This left the “do not test, but treat all with oral supplements” strategy as the most cost-effective. Compared with the reference strategy (do not test, do not treat), the ICER for treating all with oral supplements without ordering a serum cobalamin pathology test was USD 4,466 per QALY gained.
The cost-effectiveness acceptability curves from the probabilistic sensitivity analyses (also supported by the one way sensitivity analyses) showed that at relatively low cobalamin deficiency prevalence levels (e.g., 1 percent), the “do not test, do not treat” strategy was the most cost-effective up to the threshold level of USD 62,517 per QALY (equivalent to AUD 70,000 per QALY) (Figure 1). At higher prevalence values (i.e., more than 1 percent), not testing but treating all those presenting with unexplained fatigue with oral supplements was the most cost-effective strategy.

Figure 1. Cost-effectiveness of diagnostic/treatment strategies of cobalamin deficiency among patients with unexplained fatigue shown by acceptability curves.
DISCUSSION
Focusing on unexplained fatigue in general practice and using the best evidence available, we have shown that testing for vitamin B12 deficiency using serum cobalamin in a population with a low pretest probability of serious illness is not cost-effective. The poor diagnostic accuracy of serum cobalamin, its high safety, and high cumulative cost, together with the low pretest probability of deficiency enabled us to conduct this current economic evaluation despite the uncertainty in available evidence.
Evidence is needed to differentiate between effective and less effective tests or interventions. Diagnosing and treating suspected cobalamin deficiency in general practice is costly and often uncertain, especially among patients presenting with nonspecific symptoms such as fatigue that may be caused by a range of other medical conditions, including psychological or mental conditions. Inappropriate test ordering among clinicians has been found to be a primary reason for increased laboratory use. The British National Pathology Alliance Benchmarking Review reported an annual rise of 5 percent to 10 percent in requests for laboratory tests in the United Kingdom (31), with vitamin B12 and folate pathology tests being among the most repeated and inappropriately requested tests. This increased usage of serum vitamin B12 tests observed in the UK, Australia and elsewhere seems not to be influenced by the test's low diagnostic accuracy or high costs, indicating that a physician's decision to order a serum vitamin B12 test may involve more than just scientific evidence. Over-ordering may be the result of a common perception among physicians that the unit cost of vitamin B12 test is cheap. However, physicians often disregard the fact that these tests have a high cumulative cost. Concerns about missing an important serious diagnosis may be another incentive for the increased ordering of routine or battery of tests (Reference Kassirer and Milstein14). Despite the numerous tests ordered, no more than 10 percent of patients presenting with fatigue in general practice will have a somatic illness based on pathology ordered (Reference Sharpe and Wilks11;Reference Britt, Miller and Charles17). In a clustered randomized trial that assessed the yield of ordering blood tests for patients presenting with unexplained fatigue in general practice, Koch et al. (Reference Koch, van Bokhoven and ter Riet18) found that 14 of the 173 patients (8 percent), for whom pathology tests were ordered, had a somatic illness. Vitamin B12 deficiency was diagnosed in one person (0.6 percent). The remaining 13 patients had a range of conditions. In patients with a higher pretest probability of deficiency than appears to be the case in those presenting with unexplained tiredness, our results recommend a trial of treatment with oral supplements without testing for deficiency.
Currently, no diagnostic criterion standard for cobalamin deficiency exists. All available tests have disadvantages. Serum MMA, tHcy, and holo-TC are sensitive metabolic markers of cobalamin tissue deficiency (7;Reference Carmel32), whereas elevated MMA is specific to cobalamin deficiency except in renal insufficiency and other metabolic diseases (Reference Carmel, Green, Rosenblatt and Watkins33;Reference Savage, Lindenbaum, Stabler and Allen34). In addition, serum tHcy levels may be elevated in various medical conditions (e.g., folate deficiency, levodopa therapy, renal insufficiency, alcoholism, hypothyroidism, leukemia, and other metabolic and inborn conditions) (Reference Carmel32–Reference Savage, Lindenbaum, Stabler and Allen34). Therefore, the usefulness of tHcy as the sole diagnostic test is limited. Of all tests, serum holo-TC is the least accessible. Our study found that ordering serum cobalamin is not cost-effective in diagnosing cobalamin deficiency in patients presenting with unexplained fatigue. More research is required to evaluate the cost-effectiveness of other currently used pathology tests.
Streamlining the diagnostic process of cobalamin deficiency in general practice or partially disinvesting in this health technology, as we suggest in this analysis, is challenging because there are a myriad of factors that affect health professionals’ or consumers’ behavior. One factor relates to how healthcare providers are paid. At present Australia heavily relies on provider payment methods considered by the World Health Organization to be the least effective way of curbing expenditure growth: fee-for-service payments and activity-based funding, both giving strong incentives to increase the volume of care delivered and therefore overall expenditure (35). A possible way to curb expenditure among subjects with a low probability of serious disease is to encourage greater role substitution, for example by increasing the services of nurse practitioners or physicians’ assistants and by recommending a restricted set of pathology tests as is currently done in The Netherlands and Canada (Reference Kenter, Okkes, Oskam and Lamberts15;Reference Godwin, Delva and Miller20). To help control health expenditure growth, jurisdictions often request economic data in support of their decision-making processes for the pricing, reimbursement, streaming or disinvestment of health technologies. Because the conduct of this cost-effectiveness study, and owing to other on-going studies, MBS item 66602 has been split such that the current pathology test investigating cobalamin deficiency does not include both serum B12 and red cell folate (19). This in turn may lead to a reduction in use.
The lack of a definitive management pathway for patients presenting with unexplained fatigue, and the associated uncertainty regarding the eligible population and the distribution of cobalamin deficiency prevalence levels comprise the main limitations of this study. Our utility scores have been derived with the use of hypothetical health state scenarios, and there is a need to compare our hypothesized model with an empirical one with actual data on patients when these become available. Despite these limitations, the results of this study suggest that the increasing demands for cobalamin pathology testing observed in the United Kingdom, Australia, and elsewhere are not warranted given the poor test characteristics and the associated high aggregate intervention costs. Inappropriate testing or over-testing potentially increases the number of false positive results which in turn may lead to a cascade of further investigations incurring additional costs and inappropriate or unnecessary treatment.
CONCLUSION
There is a need to improve the appropriateness of test ordering for patients presenting with unexplained fatigue in the primary care setting. Changes in the approach to B12 testing suggested by our analysis would also alter the current approach to treatment decisions. The evidence base behind much routine laboratory testing is limited and inappropriate pathology testing is common practice. Despite the test's inaccuracy and lack of evidence of its cost-effectiveness, the number of pathology tests investigating cobalamin deficiency has increased in all age groups in Australia. When evidence for existing technologies is limited, disinvestment may prove difficult. Inadequate resources for primary research into such established technologies, and lack of political, clinical, and administrative will to support such disinvestment in the absence of definitive evidence of lack of cost-effectiveness are further factors which may impede the disinvestment process. However, lack of data should not be a reason for rejecting economic modeling in healthcare studies (Reference Karnon, Carlton, Czoski-Murray and Smith36). Our analysis should inform debate on improving practice by making requests for B12 pathology tests more rational and cost-effective. Our work illustrates the significant potential for minimizing waste thus improving quality in health care. The conclusions reached here would not compromise patient care, yet they would yield significant savings, allowing redistributions toward higher-value healthcare interventions.
SUPPLEMENTARY MATERIAL
Supplementary Documents 1–4 http://dx.doi.org/10.1017/S0266462315000331
CONFLICTS OF INTEREST
GM, JK, JRM and MM declare that they have no conflicts of interest. JEH and AGE sit on the Australian Government Safety, Quality and Sustainability Forum, which considers services for review as to their appropriateness on Medicare. ORF declares a potential conflict of interest due to his appointment as a member of the Pathology Services Advisory Committee of the Australian Government Department of Health and Ageing.