Introduction
Dehiscence of the sigmoid sinus is a rare cause of pulsatile tinnitus.
Venous causes of pulsatile tinnitus include a high or dehiscent jugular bulb, high flow through local emissary veins (especially the condylar or mastoid vein), local venous stenosis (especially in the transverse sinus), idiopathic intracranial hypertension and idiopathic causes (venous hum). Sigmoid sinus causes are rare, with diverticulum being the most common associated abnormality; sigmoid sinus dehiscence has been reported only relatively recently.Reference Eisenman1–Reference Otto, Hudgins, Abdelkafy and Mattox4
A case series of sigmoid sinus dehiscence has been recently published, with all cases showing the dehiscence located at the transverse sigmoid junction.Reference Xue, Li, Sun and Liu5 Sigmoid sinus dehiscence has the same clinical characteristics as other venous causes of pulsatile tinnitus, including a rhythmic character in time with the patient's pulse, aggravation with head turn to the contralateral side (increasing venous flow through the ipsilateral jugular vein), and reduction with head turn to the ipsilateral side or direct compression of the ipsilateral jugular vein (reducing venous flow through the ipsilateral jugular vein).Reference Mehall, Wilner and LaRouere6
Case report
A 24-year-old woman presented to the out-patient clinic complaining of constant, right-sided, pulsatile tinnitus of four years' duration. It had begun gradually following the birth of her second child. The patient was overweight but had no other medical history.
A full head and neck examination was performed. Upon auscultation, the tinnitus could not be detected over the mastoid, ear, neck or eye, despite manoeuvres which increased the subjective sensation. Subjectively, the tinnitus sensation increased when the patient turned her head to the contralateral side, and decreased with head turning to the ipsilateral side and compression of the ipsilateral jugular vein.
Pure tone audiography and tympanometry were normal.
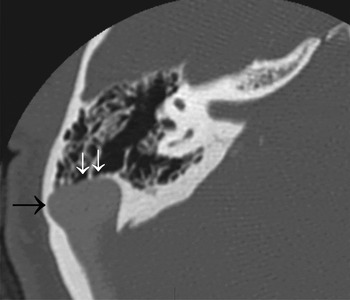
The patient underwent computer tomography and magnetic resonance imaging (including arteriography and venography) of the head, temporal bone and neck. The findings confirmed a well pneumatised temporal bone with a large, laterally placed sigmoid sinus with areas of focal dehiscence in its mid-section (see Figure 1).

Fig. 1 Axial computed tomography scan of the right temporal bone, showing a laterally placed sigmoid sinus (large arrow) and areas of dehiscence (small arrows).
After offering conservative therapy, and with full patient consent, the patient elected to undergo transmastoid resurfacing of the sigmoid sinus. The surgical steps are shown in Figure 2. After a free temporalis fascia graft was harvested, musculoperiosteal flaps were raised by incising onto the mastoid tip, superiorly behind the ear canal and then onto the zygomatic root (Figure 2a). This created a flap which included the temporalis muscle and fascia, together with a posteroinferior occipital flap extending towards the mastoid tip. A standard cortical mastoidectomy was performed, including skeletonisation of the sigmoid sinus from the transverse sinus to below the area of dehiscence, taking care inferiorly to preserve the facial nerve. Two main areas of dehiscence were found (1 and 3 cm below the transverse sigmoid junction; see Figure 2b). The overlying bone from the sigmoid was removed, and bipolar diathermy was used on a low power setting to retract the sigmoid sinus adventitia from the surrounding bone (Figure 2c). Free temporalis muscle was harvested and packed tightly into the intervening space between the mastoid and the sigmoid sinus, taking care not to significantly compromise or occlude the lumen of the sigmoid (Figure 2d). Free temporalis fascia was placed over the area (Figure 2e). The temporalis muscle was incised onto the periosteum posterosuperiorly to increase the arc of rotation of the posterior flap, which allowed it to also cover the sigmoid area. Thus, three direct soft tissue coverings were supplied to the sigmoid (Figure 2f). The skin and soft tissue were then closed in layers and a mastoid head dressing was applied.

Fig. 2 Steps in the surgical repair of right sigmoid sinus dehiscence. Surgical photographs show the right ear; the top border of the photograph indicates the anterior aspect and the left border the superior aspect. (a) A musculoperiosteal flap was created by incising onto the mastoid tip, superiorly behind the ear canal and then onto the zygomatic root. (b) Areas of dehiscence (small arrow) and eggshell-thin bone over the sigmoid sinus (large arrow). (c) The bone overlying the sigmoid sinus was removed, and low-power bipolar diathermy was used to retract the sigmoid sinus adventitia from the surrounding bone. (d) Free temporalis muscle was packed into the intervening space between the mastoid and the sigmoid sinus. (e) Free temporalis fascia was placed over the area. (f) The temporalis muscle and musculoperiosteal flap covering the sigmoid sinus.
On the post-operative ward, the patient's subjective, pulsatile tinnitus was only present in certain head positions. On the first day after surgery, it was not reproducible.
Three months post-operatively, the patient remained asymptomatic. Her post-operative audiogram was unchanged.
Discussion
The symptoms of pulsatile tinnitus due to sigmoid sinus dehiscence are presumably caused by a high level of turbulent flow through the sigmoid sinus, but also by the paucity of tissue between the sigmoid sinus and the middle ear and the resultant reduction in dampening of the sound.Reference Mehall, Wilner and LaRouere6 All previously reported cases of sigmoid sinus dehiscence causing pulsatile tinnitus have been localised to the transverse sigmoid junction.Reference Xue, Li, Sun and Liu5 The authors reporting this previous series postulated that the shape and angle of a normal transverse sigmoid junction may create turbulent flow with resonance in the mastoid cavity. The present case had an intact transverse sigmoid junction, and is the first reported case with a mid-sigmoid dehiscence. It should also be noted that our patient's sigmoid sinus was large and laterally placed, and her temporal bone was well pneumatised with no cells between the dehiscence and the antrum. The present and previously reported cases demonstrate that a diverticulum, although potentially present, is not needed to cause pulsatile tinnitus in the setting of dehiscence, and repair should therefore aim to address the dehiscence and not the diverticulum. Surgical resurfacing of the sigmoid sinus dehiscence resulted in elimination of symptoms, both in the previously reported series and in our patient.Reference Xue, Li, Sun and Liu5
• Sigmoid sinus dehiscence is a treatable cause of pulsatile tinnitus
• Extraluminal compression during repair should be avoided
In the past, internal jugular vein ligation has been used to treat venous pulsatile tinnitus; however, this has the potential devastating complication of hydrocephalus.Reference Ward, Babin, Calcaterra and Konrad7, Reference Hentzer8 Sigmoid sinus resurfacing provides a safer alternative. When considering any treatment affecting the ipsilateral venous outflow of the brain, the contralateral outflow must first be confirmed.
Care must be taken when repairing or resurfacing the sigmoid sinus in the setting of a dominant sinus. Reduction in flow through a dominant sigmoid sinus may result in hydrocephalus.Reference Wee, Song, Koo and Kim9 Wee et al. have reported a case in which the patient complained of immediate, severe headache post-operatively with clinical signs of hydrocephalus, necessitating a return to the operating theatre. Fortunately, this enabled resolution of the patient's increased intracranial pressure; however, the consequences of unresolved hydrocephalus may be severe, and should be included in the patient consent process. The present case demonstrates that full resolution of the patient's symptoms can be achieved without significant extraluminal compression. Avoiding significant extraluminal compression appears to be the key to preventing the complication of post-operative hydrocephalus.
Major complications have also been reported in the repair of sigmoid sinus diverticulum.Reference Eisenman1 Sigmoid sinus diverticulum repair techniques have been previously reviewed; the present technique is similar except that no bone or bone substitutes were used for resurfacing.Reference Eisenman1
It is unclear why our patient became symptomatic in her twenties after a second pregnancy, despite presumably having a congenital venous malformation. The sigmoid sinus, with or without the transverse sinus, is often skeletonised during mastoid surgery; however, venous, pulsatile tinnitus has not been reported as a post-operative complication. Presumably, the blood and soft tissue present post-operatively over the sigmoid sinus are enough to prevent transmission of sound to the ear.
Our patient was female and had right-sided pathology. Previous authors have noted a right-sided predominance for sigmoid sinus related tinnitus, suggesting the typical right-sided dominant venous drainage, and a female predominance, suggesting idiopathic intracranial hypertension, and have proposed that these factors may play a role in pathogenesis.Reference Eisenman1