


Introduction
Syndromic surveillance is the real-time (or near real-time) collection, analysis, interpretation, and dissemination of health-related data to enable the early identification of the impact (or absence of impact) of potential human or veterinary public-health threats which require effective public-health action.Reference Triple 1
Syndromic surveillance systems have been demonstrated to provide early warning of increasing disease activity, for example rises in seasonal influenzaReference Cooper, Verlander and Elliot 2 and norovirus,Reference Edge, Pollari and Ng 3 or monitoring pandemic influenza.Reference Smith, Smith and Olowokure 4 The Real-Time Syndromic Surveillance Team (ReSST) within Public Health England (PHE; United Kingdom) coordinates a national program of syndromic surveillance systems, which includes general practitioner (GP),Reference Harcourt, Fletcher and Loveridge 5 sentinel emergency department (ED),Reference Elliot, Hughes and Hughes 6 and telehealth systems (National Health Service [NHS] 111).Reference Harcourt, Morbey and Loveridge 7
In the United Kingdom (UK), ambulance services usually deploy ambulances in response to callers with clinical conditions that are triaged as serious and/or severe in line with their existing algorithms. As part of the continuous improvement of the syndromic surveillance systems and activities, the Ambulance Data Syndromic Surveillance System (ADSSS) was identified as a system that may complement existing systems by providing an additional measure of the “severe” end of the clinical disease spectrum. Syndromic surveillance of severe illness is currently monitored by the sentinel ED surveillance system which monitors 36 sentinel EDs; however, this system does not have nation-wide coverage and each individual ED requires bespoke individual arrangements. In the UK, ambulance services are provided by only 14 NHS organizations (11 in England), which is a feasible number to engage with to develop an ambulance data surveillance system with nation-wide coverage.
Ambulance data have been used for syndromic surveillance purposes in other countries with varying results regarding its utility. In New York City (New York USA)Reference Greenko, Mostashari and Fine 8 and Denmark,Reference Harder, Andersen and Bæhr 9 ambulance data have been effectively used to monitor trends in influenza-like illness, but the experience in Melbourne, Australia highlighted difficulties in interpretation due to an observed high degree of background “noise” associated with ambulance data.Reference Coory, Kelly and Tippett 10
In the UK, ambulance data have been used to demonstrate that extreme weather has an impact on number of emergency call-outs and response times of ambulances,Reference Thornes, Fisher and Rayment-Bishop 11 but these data have not yet been used as part of a routine, real-time syndromic surveillance system.
To determine the feasibility and utility of using ambulance data as part of routine syndromic surveillance activities, an ADSSS was developed and piloted in the West Midlands (WM) region of England.
Methods
From September 1, 2015 through March 1, 2016, a pilot syndromic surveillance system utilizing ambulance data from the West Midlands Ambulance Service (WMAS) NHS Foundation Trust was designed, implemented, and prospectively assessed. The WMAS is an ambulance service provider which serves a population of 5.6 million people in the WM region of England and is the sole provider of emergency ambulatory services in the WM. 12
The WMAS provided a line listing of daily call data (for the previous day 00:00 to 23:59 hours) via an automated Secure File Transfer Protocol service. This daily dataset included anonymized information on time and date of call, partial postcode of location of call, age of patient, chief presenting complaints (CPCs), and severity of call as determined by the call operator algorithm.
The CPC was assigned to each call by an ambulance call operator from a list of 32 based on their immediate assessment of the call. Eleven CPCs were selected (Table 1) for inclusion in the ADSSS dataset based upon their public-health importance and analogy to existing indicators used in other PHE syndromic surveillance systems.
Table 1 List of Selected ADSSS Chief Presenting Complaints Monitored during the Pilot, September 1, 2015 through March 1, 2016

Abbreviations: ADSSS, Ambulance Data Syndromic Surveillance System; CPC, chief presenting complaint.
Surveillance cases were defined as calls to the WMAS regarding patients who were assigned any of 11 specified CPCs from September 1, 2015 through March 1, 2016.
Descriptive analyses of the ADSSS dataset was undertaken, including time series plots to visually examine trends over the study period. On a weekly basis, daily data were plotted and assessed and then compared against a baseline and deviations from the expected baseline recorded. In the existing suite of syndromic surveillance system coordinated by PHE, analysis of data is undertaken on a daily basis; with the pilot ambulance system, data were analyzed prospectively on a weekly basis. The rationale behind this decision was that it was a timely enough period to triangulate findings with existing systems on a near real-time basis; secondly, public-health alerts would not be made based on a syndromic surveillance system until the pilot period had been completed, and thus daily analysis was unnecessary; and finally, undertaking weekly analysis reduced the impact and resource requirement on the team. Statistical alarms (Rising Activity, Multi-Level Mixed Effects, Indicator Emphasis [RAMMIE])Reference Morbey, Elliot and Charlett 13 were run prospectively daily and reviewed on a weekly basis.
The WMAS provided comparable historical data from the two-year period preceding the pilot (August 31, 2013 to August 31, 2015; Table 1). This was used to parameterize a multi-level hierarchical mixed effects model (RAMMIE) that compares contemporaneous data to historical data to detect significant increases in call numbers for specific CPCs (statistical alarms) compared to recent (“spike alarm”) and baseline (“historic” alarm) call numbers.Reference Morbey, Elliot and Charlett 13 This model enabled the generation of the “baseline.”
Time series plots of the respiratory ADDSSS CPCs were compared with national respiratory syncytial virus (RSV) and influenza virus laboratory confirmations during the same time period. National laboratory confirmations were used due to small numbers of laboratory confirmations at a regional level.
Preliminary assessment of the pilot ADSSS was conducted based on selected aspects of the guidelines proposed by Klaucke, et al,Reference Klaucke, Buehler and Thacker 14 specifically:
-
∙ A description of selected system attributes, including stability (the ability to collect, manage, and provide data properly without failure), data quality (the completeness and usability of the data recorded in the system), and timeliness;
-
∙ Description of findings of public-health relevance and triangulation with known incidents/events (for example, changes in burden of seasonal respiratory infections, extreme events, or mass gatherings) and data from other syndromic surveillance systems; and
-
∙ Estimation of resource requirements, in terms of time-resources used to operate the system daily, identifying and describing challenges and key lessons throughout the pilot period and solutions that were implemented.
Results
Descriptive Epidemiology
From September 1, 2015 through March 1, 2016, the ADSSS collected 207,331 individual anonymized records (daily mean=1,133; range=923-1,350). The total number of calls by day of the week were similar to one another, with no “weekend effect” apparent. There were 107,680 female patients (51.9%), 46.6% were males, and 1.5% of indeterminate gender. The median age of patient was 49 years (range 0-108), although this differed by CPC (Table 1).
Visual inspection of the time series of daily call numbers showed that only one CPC, “breathing problems,” appeared to demonstrate seasonality. Breathing problems calls increased during September 2015, peaked on January 6, 2016, and decreased throughout February 2016 (Figure 1). This pattern correlated with the seasonal increase in respiratory indicators in other syndromic surveillance systems and coincided with the winter seasonal influenza activity.
Of the 11 CPC indicators to which the statistical algorithm was applied, there were 49 statistical alarms generated during the study period. The majority (n=30) were for the breathing problems CPC. The statistical alarms for the breathing problems CPC observed during September 2015 coincided with an increase in calls for breathing problems among persons aged one to four years. This increase also coincided with a peak in laboratory reports of RSV infection (Figure 1). The age group one to four years demonstrated a peak in calls which appeared similar to the pattern of national RSV confirmations (Figure 1).
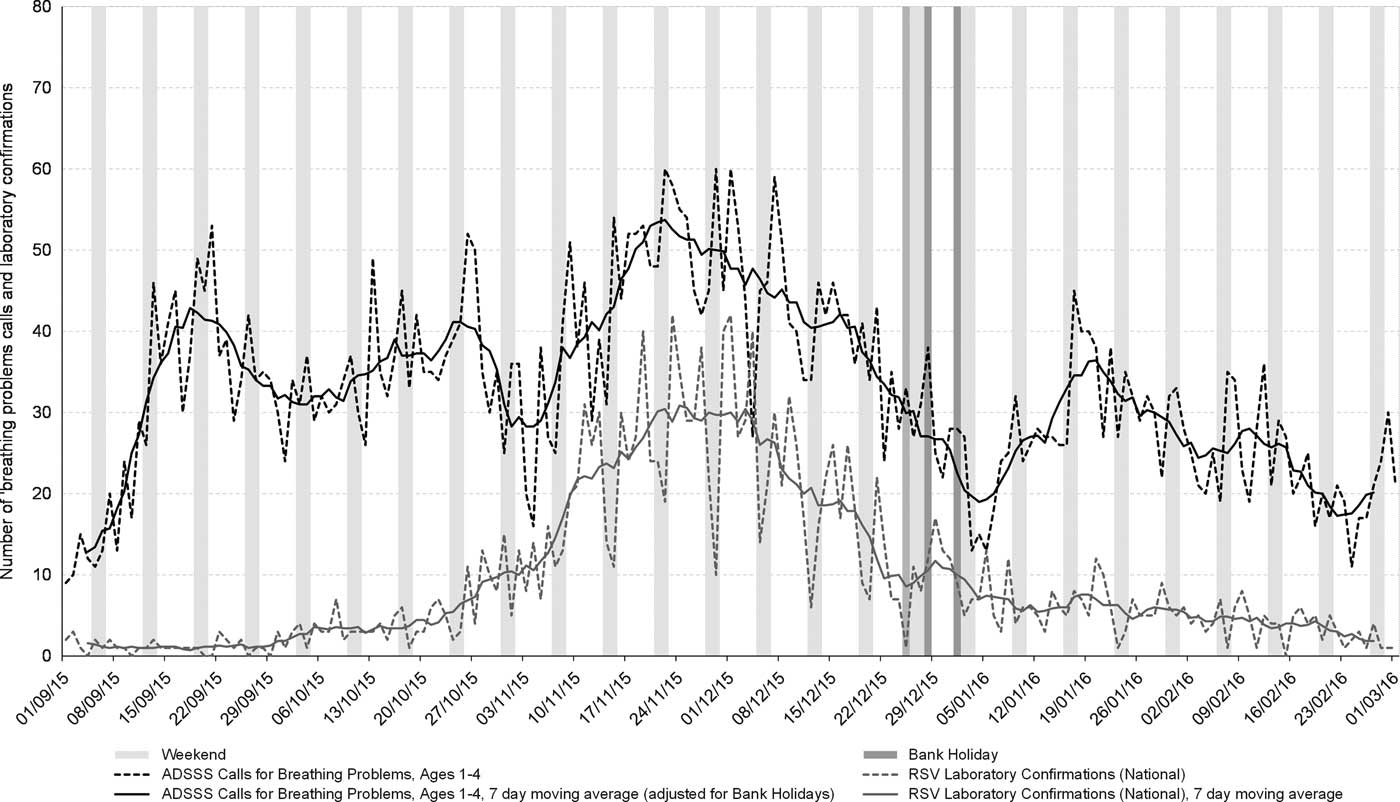
Figure 1 Daily Number of Ambulance Calls for Breathing Problems among Persons Aged One to Four Years Compared with RSV Laboratory Reports, WM and National, September 1, 2015 to March 1, 2015. Abbreviations: ADSSS, Ambulance Data Syndromic Surveillance System; RSV, respiratory syncytial virus; WM, West Midlands.
A further statistical alarm was observed in January 2016, highlighting an increase in breathing problems calls in the 45+ age group.
There were two statistical alarms for ambulance calls for “overdose/ingestion/poisoning” on October 31/November 1, 2015 (Halloween) and January 1, 2016 (New Year’s Day; Figure 2). Call volume was highest in the 15-24 years age group.

Figure 2 Number of Ambulance Calls for Overdose/Ingestion/Poisoning, All Ages, September 1, 2015 to March 1, 2016. Note: Arrows highlight alarm generated on October 31/November 1, 2015 and January 1, 2016.
Three of the CPC indicators (abdominal pains, stroke/CVA, and sick person - specific diagnosis) demonstrated excessively “noisy” data and proved difficult to interpret. During the assessment period, there were no mass gatherings or extreme events, so it was not possible to assess the utility of the ADSSS in this context; although, the feasibility of collecting the data feeds in real-time was demonstrated.
System Attributes
Stability, Data Quality, and Timeliness
Throughout the pilot period, delivery of the ADSSS dataset was stable and was automatically delivered on a daily basis by WMAS to PHE at 08:15 hours (including weekends) the day following the call. Data quality remained consistently high; the ADSSS collected 209,418 individual call records during the pilot period, of which 207,331 (98.3%) were usable. Data quality was ensured by regular checking of data feeds with the data provider to ensure data in the surveillance system matched those held by WMAS, triangulation with data and trends from other syndromic surveillance systems, and comparison with baselines generated from historical data.
Feasibility
To operate the system with weekly review of the data, it was observed that approximately two hours of an information officer’s time was needed to review the data quality, an initial review of the trends and alarms, and produce a bulletin. An additional 30 minutes of a senior scientist’s time and 30 minutes of consultant epidemiologist’s time was required for further review and assurance.
Discussion
The feasibility and utility of establishing an ADSSS was examined.
A daily automated feed of ambulance data from a large ambulance trust in the WM region was established and a role for ambulance data in monitoring changing trends in emergency community morbidity due to respiratory problems was demonstrated, some of which appears to be caused by a common respiratory pathogen (RSV). Importantly, interpretation of results and subsequent (possible) public-health alerts would have been made with triangulation with data and alarms from other syndromic surveillance systems.
The identification and near real-time monitoring of trends in community morbidity, such as the rise in respiratory problems in different age groups, may supplement information from the existing suite of systems and allow for timely, reactive public-health actions. The rise in the one to four (years) age group appears to follow the pattern of RSV laboratory confirmations, but also other rises appear to coincide with the return of children to school from summer holidays, which is observed in other UK syndromic surveillance systems and described elsewhere.Reference Sears and Johnston 15 Furthermore, although an increase in ambulance calls for overdose or ingestion around New Year’s Eve is perhaps unsurprising, the ADSSS offers new insights by allowing interrogation of the excess by age group and geographical location. As with the excess seen during Halloween, these alerts may be amenable to further investigation and targeted public-health activity by relevant health promotion teams. Although some of this information might be gathered by existing public-health routes at a local level, a national ambulance surveillance system might allow the monitoring of intelligence across regional boundaries.
In addition, usable data feeds and alarms have been established which could be of use during mass gatherings or extreme events; but this potential remains untested.
Operating the system appeared feasible; extrapolating from the observed time to operate on a weekly basis, it was estimated that on a near real-time daily basis, expanding to national coverage would require approximately five hours of an information officer’s time, two and a half hours of a senior scientist’s, and one hour of a consultant epidemiologist’s time per week.
The results are consistent with other studies which demonstrated usefulness of ambulance data for monitoring influenza-like illnessReference Greenko, Mostashari and Fine 8 , Reference Harder, Andersen and Bæhr 9 , Reference Mostashari, Fine and Das 16 and adds to the developing evidence base to support such systems. The sharing of expertise on the development of syndromic surveillance systems is of interest to the international community as syndromic surveillance is increasingly used for public-health purposes.Reference Harcourt, Morbey and Loveridge 7
A number of operational challenges were identified and lessons learned:
-
∙ Operational challenges included an unavoidable change in the way some indicators, additional to the selected 11 CPCs, were categorized close to the start of the pilot, precluding their inclusion in the pilot. As with all syndromic surveillance systems, which are passive by their nature, control is often dependent upon external factors or organizations and a pragmatic approach is necessary;
-
∙ Ensuring effective “buy-in” and collaboration from the service provider is critical to the effective development and operation of such systems;
-
∙ Although automation of output requires individual tailoring to systems, the principles remain similar between existing syndromic surveillance systems, which can speed the development process (for example, the alarm algorithms were based on those already in operation within the PHE syndromic surveillance service);
-
∙ Operation of the system as part of a “suite,” rather than stand-alone, provided multiple benefits, allowing observed events to be triangulated with information from other systems (and vice versa), the sharing of development and operational expertise, and additional resilience in the event of problems with a single system; and
-
∙ Extreme events or mass gathering are rare events, and demonstrating the value of a system where the primary benefit may be during such events is challenging.
Next Steps
The system was limited to one ambulance trust and geographical region; based on the results of this pilot, future development could include incorporating other UK ambulance trusts, increasing the coverage of the system. This report presents preliminary findings, but a comprehensive evaluation covering all relevant surveillance attributesReference Klaucke, Buehler and Thacker 14 would provide greater insight into the value of ambulance data for syndromic surveillance purposes. In addition, time-series analysis techniques might further elucidate the relationship between ambulance data and respiratory pathogens.
Limitations
The ADSSS itself was limited to the CPCs, rather than more granular clinical information initially collected by ambulance paramedics at initial contact with the patient, potentially reducing the sensitivity of the system. The study is limited to the geographical location served by WMAS and may not be externally valid. In addition, the alarm system itself requires further validation for ambulance data.
Conclusions
Further validation is necessary; however, the results from this initial descriptive study suggest that selected, but not all, ambulance data appear to have some utility for syndromic surveillance purposes in England, and the lessons learned may be of use to others setting up such systems.
Acknowledgements
The authors thank Dr. Sue Ibbotson, Centre Director, Public Health England; and Dr. Anthony Marsh, Chief Executive Officer, West Midlands Ambulance Service NHS Foundation Trust for their support in the initial phases of this work.



