


Introduction
As European populations progressively grow older, an increasing number of people are finding themselves in need of help in carrying on their daily activities (Borg and Hallberg, Reference Borg and Hallberg2006). While 16.5 per cent of the population in Europe was aged 65 years and older in 2004, this figure had risen to 19.2 per cent by 2016. In Germany, 21.1 per cent of population was aged 65 and older in 2016, one of the highest percentages in Europe (Eurostat, 2017). The percentage of the German population aged 80 years and older was at 5.6 per cent in 2014, a figure that is expected to rise to 8.5 per cent by 2030 (Bundeszentrale für politische Bildung, 2016; Bertelsmann Stiftung, 2017). This section of the population is likely to become reliant on the help of others in their daily lives.
Even at a time when female participation in the labour market is increasing dramatically, women still tend to take on the role of main family care-giver: 76 per cent of all care-givers in Europe are women (Dentinger and Clarkberg, Reference Dentinger and Clarkberg2002; Triantafillou et al., Reference Triantafillou, Naiditch, Repkova, Stiehr, Carretero, Emilsson, Di, Rastislav, Brichtova and Ceruzzi2010). In the case of Germany, it has been shown that over 70 per cent of primary care-givers are female – usually the daughter or wife of the person they are caring for (Federal Ministry for Family Affairs, Senior Citizens, Women and Youth, 2006). The age at which women are most likely to provide care is during their forties and fifties – i.e. while they are still of working age – and they are therefore particularly likely to experience severe difficulties in reconciling the needs of paid work with those of unpaid care (Spiess and Schneider, Reference Spiess and Schneider2003; Henz, Reference Henz2004, Reference Henz2006; Meng, Reference Meng2013).
Against this backdrop, this study explores how women in the mid- to late stages of their careers combine paid work with unpaid care for sick, disabled or elderly individuals. In Germany, with its comparably elderly population structure and a growing number of women in the labour force, the issue of combining care with work has gained in significance over the last few years. While 65.0 per cent of women were in the labour force in 2006, by 2016 this number has grown to 74.5 per cent (Statistisches Bundesamt, 2017). Likewise, according to official statistics, the number of individuals in need of care has increased from 1.1 million in 1995 to 2.9 million in 2016, a figure that is expected to continue to rise into the future (Bundesministerium für Gesundheit, 2017a).
The German government has responded to these trends by introducing cash benefits and payments in kind for some individuals in need of care and by guaranteeing the right of employees to take time off from work in order to provide family care. These policy changes were aimed at enabling care-givers to combine care-giving with employment. However, empirical studies show that care-givers still remain likely to experience serious difficulties in their efforts to combine their paid work with their unpaid role as carers. Schmidt and Schneekloth (Reference Schmidt and Schneekloth2011) report that 50 per cent of all primary care-givers who were in employment at the time a family member first needed care found themselves having to either reduce their hours or give up employment entirely. In 2010, 86 per cent of care-givers stated that they found it difficult to combine their work with their care-giving role (Institut für Demoskopie Allensbach, 2010). Keck (Reference Keck2016) has found that the risk of losing one's job is significantly higher for care-givers than non-care-givers.
This article expands on these findings by identifying which care-givers experience the greatest difficulties in their efforts to combine employment with care. For our purposes, care-giving is defined as unpaid activity aimed at helping elderly, sick or disabled individuals, a definition that does not include the care of able-bodied children. The analysis makes a distinction between middle-aged women providing higher as contrasted to lower levels of care and explores which of these groups of women find themselves able to combine their care-giving activities with full- or part-time employment.Footnote 1
This article contributes to the literature in two ways. First, it provides evidence on how different intensities of care activity influence women's subsequent employment, underscoring the importance of distinguishing between differing groups of care-givers. International research has shown that women involved in high-intensity care activities are more likely to drop out of the labour market, while women with less-intensive caring roles tend to combine care and employment more successfully through part-time working [Carmichael and Charles (Reference Carmichael and Charles2003) for the United Kingdom (UK); Heitmueller (Reference Heitmueller2007) for the UK; King and Pickard (Reference King and Pickard2013) for the UK; and Lilly et al. (Reference Lilly, Laporte and Coyte2007) – a systematic review for existing studies, mostly for the United States of America (USA) and the UK)]. Thus, empirical evidence clearly emphasises how important it is to view care-givers as a heterogeneous group and to distinguish between higher- and lower-intensity care-giving. While substantial research has already been done on this topic in the UK and the USA, as shown above, similar studies have not yet been carried out for Germany. Moreover, the results of such work are not easily transferable to Germany. By comparing the UK and Germany, it becomes evident that both countries provide high levels of support for informal care and have low to medium levels of public expenditure on care as compared to other European countries (Schulz, Reference Schulz2012). Yet, at the same time, labour market regulations in Germany and the Anglo-Saxon countries are very different. Empirical evidence shows that in Germany, due to that country's higher levels of employment regulation, it is more difficult for women to re-enter the labour market or to regain their previous levels of employment than it is for women in the UK (Giesecke, Reference Giesecke2006; Dieckhoff et al., Reference Dieckhoff, Gash, Mertens and Romeu Gordo2016).
Second, this study also contributes to the literature by focusing on three specific employment transitions: from full-time to part-time employment, from full-time working to non-employment and from part-time working to non-employment. While most previous studies explore any change in working hours due to care-giving (Meng, Reference Meng2013; Kaschowitz, Reference Kaschowitz2015), studying more substantial changes would help to deepen our knowledge about care-givers’ strategies for combining employment and care-giving. Thus far in Germany, there has been only one study that specifically focuses on the employment transitions – a work by Schneider et al. (Reference Schneider, Drobnic and Blossfeld2001). It found that having a care-giver role increases (married) women's likelihood of exiting the labour market, though it does not influence their chances of leaving full-time employment for a part-time job. It remains unclear, however, how the acceptance of more- or less-demanding roles in providing care relates to women's subsequent employment decisions and transitions.
Background
In 1995, with the aim of providing support for people with care-giving responsibilities, the German government introduced the compulsory long-term insurance system. The new law allowed recipients of care to tap into transfers of public resources to help pay for both institutional and family care (Geyer and Schulz, Reference Geyer and Schulz2014). Additionally, another new law introduced in 2008 – the Pflege-Weiterentwicklungsgesetz (the law on the further development of care-giving) – aimed to help care-givers reconcile paid work and unpaid care by allowing them to take up to six months of unpaid leave and/or to take up to ten days off in emergency situations (Naegele, Reference Naegele2014).
These laws were primarily aimed at helping care-givers to combine employment and care activities by putting a clear emphasis on care in the family over institutional models. This approach also appears to have chimed well with people's needs and wishes, as it seems clear that both the majority of care-givers wish to be able to provide care at home and the majority of care recipients want to stay at home (Geyer and Schulz, Reference Geyer and Schulz2014). In 2013, 2.63 million people were classified as disabled and thus eligible to receive care insurance benefits. This number represents 3 per cent of the total population. More than 71 per cent of them (1.86 million individuals) were receiving care on an informal basis, in most cases delivered exclusively by members of their family and social network (Statistisches Bundesamt, 2015). Aside from this group, there is also a relatively large number of individuals in need of care who are not entitled to receive any kind of care insurance benefits. This situation applies to approximately 5.4 million people, the vast majority of them receiving care in their own homes (Geyer and Schulz, Reference Geyer and Schulz2014).
Caring for the sick and the elderly can act as an enormous barrier to employment. Women are particularly likely to experience the double burden of paid work and unpaid care because they are more likely than men to be engaged in care-giving while they are of working age (Spiess and Schneider, Reference Spiess and Schneider2003; Henz, Reference Henz2004, Reference Henz2006; Meng, Reference Meng2013). The difficulties involved in maintaining employment while providing care may become even more serious in future, as numbers of very old people are constantly growing and as care needs are becoming increasingly demanding and time-consuming (Carmichael and Charles, Reference Carmichael and Charles2003).
Decisions over whether to take on more- or less-onerous levels of caring responsibilities will be strongly influenced by previous lifecourse transitions, trajectories and turning points (Elder, Reference Elder1999). As employment trajectories play a role in structuring the lifecourses of individuals, previous employment histories might be expected to influence greatly women's willingness to provide care in later life. Consequently, care-givers may self-select from a pool of individuals whose labour market opportunity costs are relatively low, because they are either under-employed or outside the labour force altogether (Lilly et al., Reference Lilly, Laporte and Coyte2007). According to the cumulative (dis)advantage approach, women with prior interruptions in their employment histories may be more likely to take on onerous caring responsibilities and either leave work altogether or reduce their involvement in employment in favour of their caring role (Lilly et al., Reference Lilly, Laporte and Coyte2007). This may result in such women suffering a further accumulation of disadvantages in the labour market as they begin their care-giving activities, which may in turn lead to reduced earning potential and retirement benefits (Dannefer, Reference Dannefer2003; DiPrete and Eirich, Reference DiPrete and Eirich2006).
Furthermore, the decision to provide care is likely to depend on other aspects of women's lives, including the family configurations in which they live and their human capital endowments (Henz, Reference Henz2004). According to the rational choice perspective, individuals are likely to maximise their resources to avoid any costs in terms of time availability or forgone income. Thus, whenever a need for care arises, women possessing the most extensive labour market resources may tend to be less willing than others to leave work or reduce their employment activities, probably because they will be more likely to have the financial means to purchase institutional care. On the other hand, however, less employment-focused women in lower-paid jobs might turn out to be the least likely to give up their jobs or reduce their employment commitments because they simply cannot afford to leave or have not yet accumulated a sufficient pension (Pavalko and Artis, Reference Pavalko and Artis1997; Spiess and Schneider, Reference Spiess and Schneider2003; Keck, Reference Keck2012). Likewise, there may also be women whose low-wage or unskilled jobs may not give them the flexibility to reduce working hours or to return to their jobs after a break. The literature shows that women in skilled positions (e.g. in the public sector) have the greatest access to flexible working arrangements (Henz, Reference Henz2004).
The availability of other members of a person's family or social network may also play an important role when women are trying to combine work and care. Women with husbands or partners may be in a position to share in the household income and thus be better able to purchase care than single women would be. At the same time, women might also be more likely to accept the role of primary care-giver in the context of households in which the woman's partner is the main contributor to the household income. Furthermore, siblings or adult children may act as potential alternative care-givers, thus alleviating women's care demands by taking on some care-related or other household responsibilities that might otherwise fall to her (Finch and Mason, Reference Finch and Mason1990; Leopold et al., Reference Leopold, Raab and Engelhardt2014). However, family members may also distance themselves from care-giving roles by appealing to competing demands in employment or other spheres as ‘legitimate excuses’ for not engaging in care activities (Finch and Mason, Reference Finch and Mason1993; Leopold et al., Reference Leopold, Raab and Engelhardt2014). Additionally, other competing caring responsibilities – looking after young children, for example – may further increase the likelihood of leaving work or reducing employment as a result of care-giving commitments (Henz, Reference Henz2004).
Besides such cost-related factors, there are other factors that relate to intrinsic motivation for providing care for sick, disabled and elderly people, even if that means leaving or reducing employment or accepting serious opportunity costs. The principle of intergenerational reciprocity (Gouldner, Reference Gouldner1960) suggests that individuals may simply provide care out of the sense of moral obligation, irrespective of their level of attachment to the labour market (Bamford et al., Reference Bamford, Gregson, Farrow, Buck, Dowswell, McNamee, Bond and Wright1998). According to this principle, the social exchange ratio is marked by a generalised principle of reciprocity, in the sense that the provision of a service may imply a service in return. For example, since parents have taken care of their children while they were young, their now adult children may feel a duty to take care of their elderly parents in return. Likewise, Principi and Perek-Białas (Reference Principi and Perek-Białas2011) report emotional bonds, a sense of duty and a personal sense of obligation towards the care recipient as the main reasons for engaging in care-giving. The literature on gender norms and expectations shows that women are socially expected to take on caring roles. Women feel a stronger social pressure than men to provide care and suffer more intense feelings of guilt if they do not live up to those expectations (Matthews, Reference Matthews2002; Bittman et al., Reference Bittman, Fast, Fisher, Thomson, Folbre and Bittman2004; Leopold et al., Reference Leopold, Raab and Engelhardt2014). In the last few years, however, changes in social norms and beliefs have occurred as a result of policies aimed at changing gender stereotypes, e.g. the quotas for fathers in parental leave schemes introduced in 2007.Footnote 2 Recent research finds an increased tendency for men to become involved in care-giving and for women to remain in employment to a greater extent than in previous years. Yet the male breadwinner together with the female carer models still remain predominant in a modified form in today's German society (Schober, Reference Schober2014; Trappe et al., Reference Trappe, Pollmann-Schult and Schmitt2015; Kelle et al., Reference Kelle, Simonson and Romeu Gordo2017).
Summing up, it has been shown that women in Germany have a sense of moral obligation to provide care as well as being faced with social expectations to do so. At the same time, the amount of care they provide is likely to vary depending on their employment histories and on the resources and constraints in play, such as the finances available to purchase care or their specific family configurations (Lilly et al., Reference Lilly, Laporte and Coyte2007). As the literature finds that the intensity of care is one of the crucial factors in determining whether women are in a position to maintain their commitment to employment or not, it may be expected that women who spend more hours on unpaid care will come up against serious time restrictions if they wish to stay in employment. Likewise, women subject to less time-consuming care responsibilities should be in a position to stay in employment by reducing their leisure time accordingly.
Data and variables
The empirical analysis drew on the Socio-Economic Panel (SOEP), a longitudinal survey of the population of Germany based on the residents of randomly selected households all over the country. Since 1984, the SOEP has collected: (a) micro-data on employment, family status and earnings, collected on an annual basis; (b) a monthly calendar of economic activity; and (c) retrospective information on participants’ individual life histories on family and employment biographies on a yearly basis since the age of 15 (Wagner et al., Reference Wagner, Frick and Schupp2007).
The analyses were restricted to the time-span from 2001 to 2014 as the information on the number of hours spent giving care was only added to the survey in 2001. The sample includes a total of 6,201 women aged between 45 and 59. All women in the sample were originally employed (either full- or part-time), while some of them subsequently transitioned to other statuses (whether to part-time employment or non-employed status). Thus, the dependent variables captured three different types of transitions: (a) from full-time work to part-time work; (b) from full-time work to non-employment; and (c) from part-time work to non-employment. The ‘full-time work’, ‘part-time work’ and ‘non-employment/outside labour market’ states were defined on the basis of participants’ self-reported employment status.
The independent variables reflect the intensity of caring roles. Adding these variables into the analysis enables one to analyse: (a) whether women exercising a caring role are more likely to experience employment transitions as discussed above; and (b) whether women with highly intensive caring roles are more likely to experience such employment transitions than other women. The question asked was how many hours per day individuals spend on different activities. One possible answer option was titled ‘Care and support for persons in need of care’. This option does not include child carers as such people are covered in a separate answer category. For the purposes of this analysis, caring roles were classified as highly intensive when women provided more than ten hours of care per week and as less intensive when women provided ten hours or fewer of care per week (the reference category was set at zero hours of care). The variable ‘intensity of caring roles’ captures information about care activities provided both on weekdays and over the weekend. The threshold of ten hours per week seems most appropriate in the German context because – by definition – high-level care in Germany is defined as involving a commitment of at least 90 minutes per day (or 10.5 hours a week).Footnote 3
While the data on the intensity of caring roles comes from micro-data files provided on an annual basis, the information on employment status was collected on a monthly basis. This means that the survey is only able to capture care-giving at the time of the interview, usually during spring or early summer of the survey year. Following Schneider et al. (Reference Schneider, Drobnic and Blossfeld2001), this information on care-giving activities was extended to include a period starting from June of the previous year and ending in December of the survey year. To make sure this approach did not bias the estimates, the same analyses were conducted with a care period of 12 months, as described in the ‘Sensitivity analyses’ section. This sensitivity analysis showed comparable and robust estimates.
Three sets of control variables were also included in the analysis. First, it controls for individual characteristics: age, region and migration background. Second, the analysis accounts for women's family-related circumstance: number of children, age at birth of youngest child, marital status, and presence or absence of siblings. Third, it includes labour market-related characteristics such as the educational attainment and occupational position of both the women themselves and of their partners, personal gross monthly income and equivalised net household income, share of years spent in full-time employment, part-time employment and non-employment, along with the female unemployment rate for East and West Germany. All independent and control variables used in the analysis are explained in more detail in Table 1.
Table 1. Defining the independent and control variables

Notes: SOEP: German Socio-Economic Panel. OECD: Organisation for Economic Co-operation and Development. 1 Online: http://statistik.arbeitsagentur.de/Navigation/Statistik/Statistik-nach-Themen/Statistik-nach-Themen-Nav.html.
Methods
The study applies the proportional hazard model as proposed by Cox (Reference Cox1972; for more information, see Blossfeld et al. Reference Blossfeld, Golsch and Gotz2007). The main focus of the investigation is on two parallel processes: employment biographies and caring activities. Changes in employment status are modelled as ‘dependent events’ while changes in the caring status are considered to be ‘independent events’. Any employment episode always starts with an original state (either full- or part-time employment) and ends either with an employment transition (into part-time employment or non-employment) or without one (a right-censored episode). To account for multiple episodes (multiple employment transitions within one person), a multi-failure design is used. This modelling approach allows one, on the one hand, to locate recurrent episodes in a lifecourse and to determine the sequence and the duration of these episodes within one person; on the other, it also allows one to account for the parallel process of changes in the caring status and to analyse whether these changes may have some relationship with the woman's risk of experiencing an employment transition (Blossfeld et al., Reference Blossfeld, Golsch and Gotz2007)
The proportional hazard regression models are estimated in Stata (version 14.1) as proposed by Cox (Reference Cox1972), applying robust standard errors. A multiple destination model (Blossfeld et al., Reference Blossfeld, Golsch and Gotz2007) is calculated for women in full-time work. These models only specify a functional form for the influence of covariates, but make no assumptions about the shape of the hazard. The hazard represents the ‘risk’ that an employment transition will occur during a particular month, assuming that it has not already occurred in the previous month. In this context, the Cox models turn out to be an appropriate choice, since the main interest is on estimated coefficients rather than on the details of any time dependency (Blossfeld et al., Reference Blossfeld, Golsch and Gotz2007). The coefficients reported indicate the change in the hazard ratio of any move into one of the destination states (i.e. part-time employment or non-employment) for every one-unit change in the relevant independent or control variable. Values above 1 indicate an increase in the hazard, while values below 1 represent a decrease.
Results
Descriptive findings
Twenty-nine per cent of women in the sample provided care for a sick, disabled or elderly individual between 2001 and 2014; 40 per cent of these care-givers experienced only one episode of care-giving, 22 per cent had two and 38 per cent more than three. On average, care-givers reported having spent 2.2 consecutive years carrying out caring activities. While women with less-intensive caring roles spent an average of 6.2 hours per week in caring activities, women with more-intensive caring roles provided on average 29.2 hours of care per week.
Table 2 displays means and proportions on the individual, family- and employment-related features of the groups defined by women without caring roles, women with less-intensive caring roles and those with more-intensive caring roles. With regard to family characteristics, all three groups of women seem similar, with the exception that care-givers are somewhat more likely to be married than non-care-givers. In addition, women with more-intensive caring roles are the least likely to have more than one sibling. Turning to the employment characteristics, it is evident that women who provide more-intensive care possess lower levels of educational attainment than other women and are less likely to have held a managerial position in their last job. Likewise, women with more-intensive caring roles have the lowest individual incomes, while non-carers and carers with less-intensive caring roles are very similar in terms of their incomes. Both non-carers and lower-intensity carers are fairly similar in terms of their employment experiences too, except for the fact that lower-intensity carers seem to have gathered slightly more experience in part-time employment and non-employment. However, women who provide more-intensive care are very different from other women in this respect: they spend considerably more time in non-employment and less time in full-time work.
Table 2. Individual, family- and employment-related characteristics of women from the three groups

Notes: Information on income is deflated. There are missing values (with either no answer or not applicable) in women's education, occupation and marital status (overall less than 1 per cent). Furthermore, the information on siblings is missing in 10 per cent of cases. On top of this, variables on education and occupational position for the partner contain missing values in up to 32 per cent of cases (for detailed information on the construction of the variable, see Table 1). SD: standard deviation.
Source: German Socio-Economic Panel (SOEP) version 31.1, weighted results, own calculations.
The group of women with less-intensive caring roles hence appears to be similar to the non-care-giver group in terms of income, employment experience and education. What is more, women who provide less-intensive care have higher household incomes and higher levels of educational attainment than non-care-givers. Women with more-intensive caring roles, however, seem to constitute a highly distinct group: they spend on average fewer years in education and seem to have a weaker attachment to the labour market as compared to the other two groups of women.
These findings indicate that while women who provide less-intensive care are as equally well educated as – or even better educated and more highly qualified than – non-care-givers, women who provide more-intensive care are likely to belong to a disadvantaged group on the labour market. However, it is important to highlight the fact that the descriptive analysis shown in Table 2 cannot account for the timing of events. What this means is that such observed characteristics as last occupational status or income may run parallel to the caring episodes and will therefore not be independent of the intensity and duration of caring. Such parallel processes are accounted for in the Cox regression models.
Model estimation results
How do employment transitions of women with more-intensive caring responsibilities differ from those of women with less-intensive caring responsibilities or no caring roles? Table 3 addresses this question by showing the results of three Cox regression models that predict transition rates (a) from full-time to part-time employment; (b) from full-time to non-employment; and (c) from part-time to non-employment. Models 1 and 2 include the entire sample (care-givers providing up to ten hours of care per week, care-givers giving more than ten hours of care per week and non-care-givers) and Model 3 includes care-givers only (those with up to ten hours of care per week and those with more than ten hours of care per week). The distinction between the two samples makes it possible to compare the influence of socio-demographic factors for women depending on their care-giver status. This comparison will follow later in the paper (the full models are reported in Table A1 in the online supplementary material). First up for discussion are Models 1 and 2. While Model 1 includes variables indicating intensity of care along with the family-related variables, Model 2 controls additionally for the employment-related variables (for a detailed description of the variables, see Table 1).
Table 3. The hazard rates for the transitions from full-time to part-time and non-employment and from part-time to non-employment for the entire sample and for care-givers only (abbreviated table)
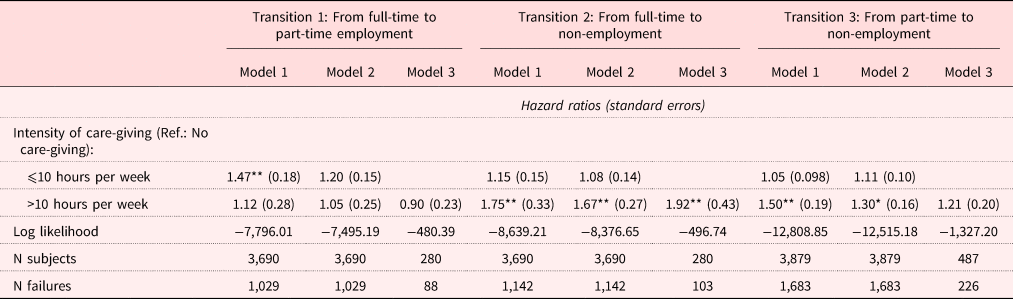
Notes: Model 1: Entire sample, reduced model (includes variables on hours spent in care and controls for individual and family-related characteristics such as age, region, migration background, age at childbirth, marital status. and presence of siblings. Model 2: Entire sample, full model (additionally accounts for employment-related characteristics: years in education (for women and their partners), occupational position (for women and their partners), individual and household income, proportion of years in full-time employment, part-time employment and out of the labour force, and female unemployment rate. Model 3: Care-givers only, full model (accounts for variables from Model 2). Information on income is deflated. Ref.: reference category.
Source: German Socio-Economic Panel (SOEP), own calculations.
Significance levels: * p < 0.05, ** p < 0.01.
The findings for Model 1 (Transition 1) – women with more-intensive caring roles (more than ten hours of care per week) – show no evidence of any statistically significant difference with non-carers in terms of their likelihood of switching from full-time to part-time employment. However, the findings for this model also indicate that women who provide less-intensive care (up to ten hours of care per week) are 47 per cent more likely to switch from full-time to part-time employment than non-carers. This indicates that even women who provide ten or fewer hours of care per week experience difficulties in maintaining their employment levels. However, in Model 2 – for lower-intensity care providers – we see that the hazard ratio of transitioning from full-time to part-time employment (Transition 1) decreases from 47 to 20 per cent. Furthermore, this variable is now no longer statistically significant. The variable becomes not statistically significant after the control variable ‘individual income’ is added to the model. Thus, the individual income factor seems to be a strong predictor of employment transitions for these women.
Furthermore, women with more-intensive caring roles are 75 per cent more likely than non-carers to transition from full-time work to non-employment (Transition 2, Model 1). Likewise, women who provide more-intensive care are more likely to go into non-employment from part-time work as well (Transition 3, Model 1), while there is no such statistical association for women providing less-intensive care. In other words, unlike women with less-intensive caring roles, who seem to be able to combine unpaid care and (part-time) employment, women with more-intensive caring roles tend to exit the labour market altogether. Adding employment-related factors (Model 2) seems to make a considerable difference: the likelihood of switching from full-time to non-employment for women providing more-intensive care goes down from 75 to 67 per cent (Transition 2) and their likelihood of moving from part-time to non-employment (Transition 3) decreases from 50 to 30 per cent.
Turning to the comparison between Model 2 (the full model, using the entire sample) and Model 3 (the full model, considering care-givers only) (see Table A1 in the online supplementary material), the first thing that becomes evident is that having a child after the age of 34 increases the risk for women in the entire sample (Model 1) of switching from full-time to part-time employment (Transition 1). There is no evidence of any such association in the ‘care-givers’ sample (Model 3), though this is possibly due to the reduced sample size. At the same time, having a child prior to the age of 34 actually decreases care-givers’ risk of transitioning from full-time to non-employment (Transition 2). Second, having a sibling turns out to be statistically significant for care-givers in part-time employment. Thus, having a brother and/or a sister increases the likelihood of leaving part-time employment (Transition 3). This is in line with previous research, which has shown that siblings tend to distance themselves from care-giving roles if the demands of their jobs, as indicated by working hours, are more onerous than those of their siblings (Leopold et al., Reference Leopold, Raab and Engelhardt2014).
With regard to the labour market factors, the analysis shows that, for the ‘care-givers’ sample, having a partner with a higher level of educational attainment prompts women to transition from full-time to part-time employment and to non-employment (Transitions 1 and 2). Furthermore, the higher the individual income, the less likely it is that women in general, and care-givers in particular, will have experienced any of the employment transitions analysed in the study. Lastly, a higher proportion of years spent in full-time and part-time employment lowers the risk run by care-givers that they end up switching into non-employment (Transitions 2 and 3). At the same time, a higher proportion of years spent in part-time employment increases the likelihood of switching from full-time into part-time employment (Transition 1).
Sensitivity analyses
In this section, the three sensitivity analyses are shown that were conducted for the study. First, different Cox regression models are compared to make sure that the assumption that hazards are proportional is not violated and that the estimates are not biased. Second, the estimates based on the 18- and 12-month caring periods are compared against one another (see the section ‘Data and variables’). Third, a variety of groupings of the control variables ‘age at birth of youngest child’ and ‘level of educational attainment’ are tested to make sure they do not influence the outcome.
First, one of the key assumptions of the Cox regression models is that the effects of covariates can induce only proportional shifts in transition rates and cannot change their shape (Blossfeld et al., Reference Blossfeld, Golsch and Gotz2007). To make sure the proportional hazard assumption is not violated, the Schoenfeld residuals test was used. The test indicated that this assumption did indeed hold for the variables measuring the intensity of care in all of the models. To elaborate on this result, three different types of Cox model regressions were estimated: (a) a basic Cox model as described above; (b) a non-proportional Cox model that accounts for the possibility that the variable ‘intensity of care’ may change in terms of its influential power over time (see e.g. Windzio, Reference Windzio2013); and (c) a stratified Cox model capable of stratifying a sample according to the ‘care variable’ (see e.g. Blossfeld et al., Reference Blossfeld, Golsch and Gotz2007). Due to the fact that all of these models showed very similar estimates, this study reported results based on the basic Cox regression models (see Table A2 in the online supplementary material).
Second, since the data on employment were collected on a monthly basis and the data on the intensity of caring roles are based on annually collected data, information on care-giving can be captured only at the time of the interview. This information was extended to a period starting from June of the previous year and ended with December of the survey year. To make sure this procedure had not biased the estimates, the same analyses were conducted under the assumption that the care period had lasted 12 months. The result of this sensitivity analysis yielded comparable and robust estimates (see Table A3 in the online supplementary material).
Lastly, to make sure the construction of the dummy variables ‘age at birth of youngest child’ and ‘level of educational attainment’ does not influence the outcome, Cox regression analyses using alternative groupings of these two variables were conducted (e.g. one of the alternative groupings of age at birth of youngest child was: up to 20 years of age, 20–40 years of age, 40 and older). None of the changes in the construction of these variables were associated with any change in the outcome.
Conclusion
The analysis asks how commitments to providing higher- or lower-intensity care for sick, disabled or elderly people influence employment transitions of women in their mid- to later career stages. To answer this question, the study distinguishes between carers who have adopted less-intensive caring roles, providing ten or fewer hours of care activity per week, and carers who have taken on more-intensive caring roles, providing more than ten hours of care per week, and also compares both of these two groups to women against those who have taken on no care-giving responsibilities at all. To learn more about the strategies that care-givers use in order to combine work and care, the study focuses on three types of employment transitions: from full-time to part-time employment, from full-time to non-employment and from part-time to non-employment.
The study argues that women in Germany both harbour a sense of moral obligation themselves and are faced with social expectations to provide care for the vulnerable people around them. At the same time, the amount of care provided is likely to vary depending on resources and on such constraints as the finances available for the purchase of care and on the woman's specific family configuration. Furthermore, from the point of view of lifecourses, the employment histories of women might be expected to be an important influence on women's willingness to provide care in later life. Women with a record of prior interruptions in their employment histories, in particular, might be expected to be more likely to take on onerous caring responsibilities and to leave their jobs or reduce the intensity of their employment in favour of caring activities. This in turn may result in reduced earning potential and less-generous retirement benefits for such women (Lilly et al., Reference Lilly, Laporte and Coyte2007).
The key finding of the study is that women who provide more-intensive care-giving are the most likely group to exit the labour market altogether, while women with less-intensive caring roles seem to be better able to combine paid work and care activities. In particular, the study first shows that women with more-intensive caring responsibilities tend to earn less and to have a weaker attachment to the labour market than other women. Thus, previous employment histories seem to play an important role in women's willingness to take on care responsibilities. However, it is important to highlight that this descriptive finding does not account for the timing of events. Second, the multivariate analysis suggests that women with higher earnings and a stronger attachment to the labour market are more likely to maintain their employment levels than other women. This result is consistent with conclusions that the rational choice framework would suggest. At the same time, the analysis shows that women with less-intensive caring roles are likely to reduce their time commitments to employment, although this coefficient loses its statistical significance once one has controlled for their individual income. This indicates that the various individual rationally calculated decisions predicted by the rational choice model cannot provide a full explanation of women's and care-givers’ employment behaviour, suggesting that intrinsic motivational factors are potentially important in understanding why it is that women are willing to accept substantial opportunity costs in order to provide care for their family members. One useful task of future research might be to disentangle further the complex relationship between women's motives in providing care and the consequences of such care-giving for their employment decisions.
German policy makers have sought to come to the assistance of care-givers by introducing laws aimed at making family care more compatible with employment. As part of these regulations, many care-givers have been granted a right to interrupt their employment without necessarily losing their entire salary. Though this measure may bring financial relief to some care-givers, there is still a need for the regulations in the area to offer an improved solution, one that better enables care-givers to reconcile their care activities with their work. This research therefore highlights the need to implement policies that support flexible working arrangements and offer respite for women with care responsibilities, hence allowing them to remain in the labour force. Such policies should aim to enable individuals who leave the labour force or drastically reduce their working hours for a period of care-giving to regain their previous levels of employment once the care period is over. In this regard, the Familienpflegezeitgesetz (the German law on family care-giving) was introduced in 2012, allowing women to request a reduction in their working hours to facilitate their care-giving activities for a two-year period (Geyer and Schulz, Reference Geyer and Schulz2014). Whether care-givers will be able to make use of this provision is something that will need to be explored in future research. This study also shows that women in lower-paid jobs with a weaker attachment to the labour market are the group at highest risk of leaving their jobs or drastically reducing their engagement in employment, despite the fact that they may be the very group with the greatest need to build up retirement benefits in order to secure their incomes in the future. This finding implies a need for institutional and professional care to be made more affordable for low- and medium-income families.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X18001423
Acknowledgements
The author is grateful to the scientists at WZB Berlin Social Science Center (WZB) and the German Center of Gerontology (DZA) who commented on earlier versions of this paper. Special thanks go to Lena Hipp and Anette Fasang, and also to the editors and the anonymous reviewers for very thoughtful suggestions and comments.





