INTRODUCTION
Pressure ulcers are not uncommon (Hanson et al.,
1994; Bale et al., 1995; Leff et al., 2000) in dying patients because of
acquired risk factors of immobility, functional incontinence, and
compromised nutrition (Hanson et al., 1991,
1994; Bale et al.,
1995; Walding & Andrews, 1995; Chaplin, 2000). However, their management, especially
the unpleasant aspects of care (Dallam et al.,
1995; Szor & Bourguignon, 1999; Kayser-Jones et al., 2003), has received little
attention from palliative care researchers. Consistent with the
traditional standards of pressure ulcer care, most of the relevant studies
are studies of the effectiveness of nursing prevention programs in single
hospices (Hanson et al., 1991, 1994; Bale et al., 1995;
Walding & Andrews, 1995; Chaplin, 2000) or factors affecting the incidence of
pressure ulcers at the end of life in long-term care (Kayser-Jones et al., 2003).
In all settings, the management of a patient with a pressure ulcer
requires an interdisciplinary approach (Baranoski et
al., 1998; van Rijswijk & Braden,
1999), and in the home environment, care is highly reliant on
family caregivers. The burdens in general experienced by families caring
for patients with terminal illness at home have been explored (Covinsky et al., 1994; Emanuel et
al., 2000). Similarly, both the burdens (Baharestani, 1994) and positive contributions (Clarke & Kadhom, 1988) of families providing
pressure ulcer care at home for chronically ill patients have been
described. We report a qualitative description of the factors contributing
to pressure ulcer care planning for hospice patients, which was collected
as part of a broad explorative study of pressure ulcers in hospice (Eisenberger & Zeleznik, 2003).
METHODS
Interview Instrument
We developed a telephone survey instrument consisting of questions
based on a Medline and bibliographic review of the medical and nursing
literature using combinations of the search terms “hospice,”
“palliative care,” “pressure ulcer,” and
“decubitus ulcer.” The instrument was reviewed for face
validity and pilot-tested on two physicians and five nurses with
experience in wound care and end-of-life care, and a family member of a
patient who died with a pressure ulcer. The format and language were
revised in consultation with an educational researcher. Three versions
were produced for interviews with directors of clinical services,
direct-care nurses, and family members. The versions had approximately
three-quarters overlap in content in order to explore different
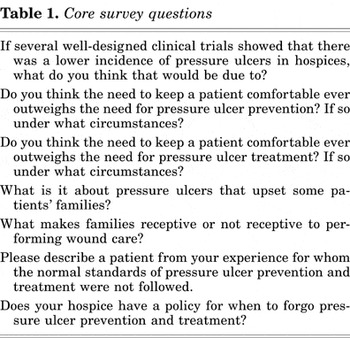
perspectives on the same clinical issue. The question formats were
open-ended and dichotomous response. The core survey questions are shown
in Table 1. The study was approved by the
Montefiore Medical Center institutional review board.
Recruitment and Interviews
A pool of hospices was purposely selected from the American Hospice
Foundation's Web site (American Hospice
Foundation, 2004) to represent various geographical regions of the
United States. A letter of introduction was sent to notify the director of
clinical services of our intention to perform a phone interview. After
verbal consent, a single investigator conducted semi-structured telephone
interviews as prearranged with each participant. At the end of the
interview, the director of clinical services was asked to provide the name
of a nurse at their institution as well as a family member of a hospice
patient who had experienced a pressure ulcer. Despite previous
participation of the families of terminally ill patients in focus groups
and surveys (Emanuel et al., 2000; Steinhauser et al., 2000), none of the hospices agreed
to allow us to interview family members of their patients. Responses were
entered verbatim as text into a Microsoft Access Database. Interviews were
continued until no new thematic concepts were obtained.
Participants
Twenty-seven of 28 hospices contacted agreed to an interview.
Saturation was reached after 28 individuals from 17 hospices were
interviewed. The participants were 18 directors of clinical services, of
whom 9 were physicians and 9 were nurses, and 10 direct-care nurses. The
characteristics of the hospices are shown in Table
2. The direct-care nurses had a mean of 4 and 18 years of hospice
and total nursing experience, respectively. Six of the direct-care nurses
worked with outpatients, three with inpatients, and one with both. None
had advanced practice training in wound care.
Characteristics of the survey participants
Data Analysis
Data were analyzed using an approach based on grounded theory (Miles & Huberman, 1994; Strauss
& Corbin, 1998). While the interviews were still being
conducted two investigators independently used a process of open-coding to
iterate broad themes by marking key phrases, sentences, or terms on
printouts of the responses. This led to the choice of hospice
team–family caregiver as the unit of analysis. After saturation had
been reached, axial coding was done by a negotiated group process on the
entire data set. Credibility was sought by presentation to an
interdisciplinary group of health care providers at a hospital that
specializes in the care of advanced cancer patients and the analysis was
subsequently revised. The illustrative quotes have been edited for ease of
reading without making substantive changes.
RESULTS
Three broad themes related to pressure ulcer care planning were
identified (Table 3). The hospice nurse is an
educator rather than a wound care provider. Family caregivers are
perceived to have barriers and burdens related to participating in
pressure ulcer care. Family caregivers collaborate with hospice providers
to establish individualized achievable goals of care for the hospice
patient. Although we collected data on institutional policy and risk
screening for pressure ulcers, the participants did not emphasize this as
significant to care planning; consequently these data are presented
separate from the qualitative analysis.
Factors related to pressure ulcer care planning in
hospice
Institutional Practice Patterns
Four of 18 hospice directors of clinical services were definitively
able to state which standardized pressure ulcer risk assessment instrument
they used. These were one each of the Braden scale (Bergstrom et al., 1987), a “modified”
Braden scale, a “4-point scale,” and an “in-house
tool.” Four hospice directors of clinical services stated that their
hospice used no formal risk assessment scale, two said that the
patient's “mobility” was assessed, and seven did not know
if they used a risk assessment scale. Five direct-care nurses did not know
what risk assessment scale they used, three said that they used none, and
two performed assessments without an instrument. Only one hospice
collected data on pressure ulcer incidence and prevalence.
There was significant variation in the use of specialty beds and
mattresses. Indications for use were related to the ulcer, the patient, or
the caregiver. The circumstances related to the ulcer ranged from
“once the skin turns red” to “a severe ulcer and [a
patient with] an unclear prognosis.” Bed utilization could also
be motivated by the “frequency of pressure ulcer occurrence and
rapidity of pressure ulcer advancement.” Patient considerations were
“once the patient can't move themselves,” or when
“the patient is at high risk and usual prevention would be very
uncomfortable.” Caregivers having “difficulty [with]
turning” was also cited as an appropriate indication. Certain
specialty beds were thought to add to patient's social isolation
because of “noise,” the patient being unable to “see and
get out of it,” or a sense of “people getting sunk.” The
actual decision to use a specialty bed was usually at the discretion of
the primary nurse, but could also be a “joint decision”
involving family caregiver preferences.
The Role of the Nurse
The direct-care nurse was universally identified as an educator rather
than as wound care provider. These nurses “do lots of hands-on
teaching,” and “preventative teaching.” The only two
nurses who did not teach family caregivers to provide pressure ulcer
related care worked solely at an inpatient hospice. Educational content
included instruction about risk factors, turning and positioning, and
topical dressing changes by the “see one, do one approach.” It
was felt that families initially have a poor understanding of the causes
of pressure ulcers, and education was considered important to reduce the
psychological impact of pressure ulcers on patients and their families.
The occurrence of a new pressure ulcer was considered a “teachable
moment,” which included emphasizing that “it's not the
family's fault.”
Barriers and Burdens
The factors cited as promoting a family's willingness to perform
wound care were the educational impact and the availability of the nurse.
Other promoting factors were pressure ulcer location, for instance,
“feet are easier than ischium,” caregiver characteristics of
“commitment,” “education level,” and
“[possessing] a feeling of control when life is out of
control.” In addition wound care performed by family caregivers
obligates the hospice team to provide a care plan that addresses
unpleasant aspects of the ulcer. Characteristics involving “sight
and smell” such as “odor,” “disfigurement,”
“ooze,” and “blood” were cited as limiting a
family's willingness to perform dressing changes. There were felt to
be limits to how much a family could participate in pressure ulcer care.
These were best described by a direct-care nurse who stated that there are
circumstances when “the level of pain and emotional difficulties for
the family outweigh pressure ulcer management.” Another nurse
remarked that “the family may refuse management because of
discomfort and the knowledge that death is imminent.” Other limiting
factors were gender and cultural barriers, “fear of
incompetence,” and fear of causing pain, expressed as
“it's scary to help someone you love.”
Incident pressure ulcers were considered burdensome to families
because of the “awful connotation reflecting neglect and
wasting.” The family caregivers were reported to experience
“guilt” that they are “not doing a good job” or
that “they [had] failed.” Pressure ulcers could also
“pull the family out of denial regarding the dying process” or
“serve as a reality check that the patient is failing.” The
development of a progressive or advanced stage pressure ulcer was also
viewed as a “care crisis” that could force admission into
inpatient hospice.
Collaboration between Family Caregivers and the Hospice
Team
For pressure ulcer prevention, care provided by well-educated families
was the most frequent reason given for a theoretical lower incidence of
pressure ulcers in hospice patients compared with patients dying in other
settings. Pressure ulcers complicate end-of-life care because “they
are a family issue.” No participant could describe a formal protocol
for deciding when to forgo preventive and healing efforts in favor of
comfort; rather they relied on the “clinical judgment” of
health care providers and considered family preferences and abilities. One
director called this the “team effect.” This process was
individualized, discussed at a “team meeting,” “deferred
to the patient and family,” or occurred when “the family
doesn't want to cause more suffering.” In this situation
hospice health care workers “need to be flexible.” Similarly,
it was also said that, “The family and patient must be in charge. If
the patient wants to stay at home and the family can't turn them,
it's better for them to stay at home and get a pressure ulcer.”
Respondents suggested that at this point it is appropriate to “focus
on symptoms” of pressure ulcers, rather than curative management. A
shift away from care related to the prevention of pressure ulcers or goals
of healing was also made when the hospice provider's clinical
judgment indicated that “death is imminent.”
DISCUSSION
These findings suggest a taxonomy of factors related to pressure ulcer
care planning in hospice that can be used for in-depth, structured surveys
of pressures ulcers at the end of life. We have identified the scope of
the hospice nurses' role as well as the barriers and burdens for
family caregivers' participation in press ulcer care. Care planning
for pressure ulcers, a condition that may occur secondarily to the hospice
diagnosis, is a model of collaborative decision making between family
caregivers. This collaboration, the “team effect,” leads to
individualized goals for pressure ulcer care in hospice patients. In
contrast institutional pressure ulcer policies and procedures were not
significantly reported to contribute to the care plan.
The role of the hospice nurse for pressure ulcers is as an educator
rather than wound care provider. This role includes teaching preventive
strategies, wound care, addressing the prognostic significance of a
pressure ulcer, and perceived feelings of guilt, failure or neglect on the
part of family caregivers. Many of these issues have been explicitly
mentioned in published care standards and guidelines (Hoffman et al., 1991; Hanson et
al., 1994; Chaplin, 2000). Clearly, in
hospice, teaching on the topic of pressure ulcers must by necessity
compete with topics such as proper use of analgesics, dietary
modifications, and review of advance directives. The relative amounts of
time spent by hospice nurses on education about the primary illness and
secondary conditions in hospice patients may warrant further study.
Family caregivers were reported to have a range of involvement in
prevention and treatment of pressure ulcers. Well-educated family
caregivers were the most frequently cited reason for a perceived lower
incidence of pressure ulcers in hospice patients. This reported
observation supports the view that care-related factors are at least as
important as patient-related factors for prevention (Clarke & Kadhom, 1988; Kayser-Jones et al., 2003). Unlike the occurrence of
symptoms of pain or dyspnea, which are attributable to the disease process
at the end of life, our participants reported that families could
attribute the occurrence of a pressure ulcer to failure of their care and
this can be a source of additional burden. With the exception of active
hemorrhaging or fungating cancers, the burden of a specific sign or
symptom is usually borne by the patient at the end of life. In addition to
pressure ulcers, there may be other conditions such as terminal delirium
for which the care plan appropriately concentrates as much education for
the caregiver as it does treatment of the patient.
The “team effect” describes family caregivers as part of
the health care team rather than surrogates of the patient or a component
of the “patient–family caregiver unit” (Raudonis & Kirschling, 1996; Brandt, 2001) who simply receive care from the health
care professionals. This term expresses that the family caregiver has
joined the interdisciplinary team not only for delivery of care related to
prevention and wound care, but also to express their own needs and to
establish individualized goals of care. Although the participation of
family members on the team was explicitly perceived to contribute to a
lower incidence of pressure ulcers in home hospice patients, the goals of
care could include acceptance of a new pressure ulcer at the end of life
in some circumstances. The team effect reported here may be the converse
of hospice nurses becoming part of the family (Raudonis
& Kirschling, 1996). The description of the team effect
confirms implicit suggestions for health care professionals to establish a
partnership with families in order to meet mutual goals (Hoffman et al., 1991; Hanson et
al., 1994; Levine & Zuckerman, 1999;
Tuch, 2003), for patients with pressure ulcers
(Maklebust & Magnan, 1992; Remsburg & Bennett, 1997; Bennett et al., 2000; Decanay,
2000), or that hospice nurses should “relinquish varying
amounts of control to family members and to include them as equal members
on the home care team” (Sergi-Swinehart, 1985 pp. 465).
The use of standardized pressure ulcer risk screening instruments
among participating hospices was low and not identified as significant for
determining the pressure ulcer care plan. This indicates an area for
improvement (Hoffman et al., 1991; Wright, 2001). Risk screening instruments designed for
use in hospitals, nursing homes, and individual hospices (Bale et al., 1995; Walding &
Andrews, 1995) have been shown to effectively reduce the incidence
of pressure ulcers, which are accepted as a source of pain (Dallam et al., 1995; Szor &
Bourguignon, 1999). A validated strategy for prevention should be
considered even at the end of life (Chaplin,
2000). One published standard of care for pressure ulcers in
hospice patients begins with a systematic risk assessment, but then
individualizes achievable prevention and healing goals (Hoffman et al., 1991). Our data suggest that the
latter, but not the former, may already be occurring in current practice.
Finally, it is important to note that even if all pressure ulcers are not
preventable, malpractice cases for alleged injuries from pressure ulcers
in other care settings have been on the basis of pain and death (Bennett et al., 2000).
Our study has several limitations. Participants were exclusively in
U.S. hospices and they may not represent the experiences and practices in
hospices in other parts of the world. Our findings regarding the use of
pressure ulcer screening instruments and specialty beds are only
suggestive and must be confirmed by formal survey of a larger random
sample of hospices. Most significantly, we are lacking a direct report
from family caregivers, which limits accuracy, but our findings are
consistent with previous direct reports of the effects of a pressure ulcer
on patients and their families (Baharestani,
1994; Langemo et al., 2000). Our
inability to interview family members is a reminder that collaboration
between hospices and researchers limits progress toward a scientific basis
for improving patient care at the end of life (Sachs,
2003).
Although our survey was conducted with nurses and physicians
practicing in hospices, it has quality-of-life and quality-assurance
implications for pressure ulcer care in terminally ill patients and their
families in hospitals, nursing homes, and home care (Keay et al., 1994; Hayley et al.,
1996; Fried et al., 1999; Baer & Hanson, 2000; Emanuel et
al., 2000; Ferrell et al., 2000; Leff et al., 2000; von Gunten et
al., 2002; Kayser-Jones et al., 2003;
Pillemer et al., 2003). The tracking of pressure
ulcer incidence rates and initiation of preventive care plans based on
established guidelines (Bergstrom et al., 1992)
is the standard of care in all hospitals and nursing homes (Moody et al., 1988; Bergstrom et
al., 1994; Bennett et al., 2000) with the
goal of absolute prevention regardless of the overall goals of patient
care. In contrast, some experts have hypothesized that not all pressure
ulcers are preventable (Hanson et al., 1994;
Bennett et al., 2000). Our data suggest that a
single standard for pressure ulcer prevention is not appropriate in all
populations, or even in all hospice patients. Contained in practice
guidelines (Bergstrom et al., 1994, p. 26) and
expert recommendations are statements that comfort goals may be more
appropriate than goals of absolute prevention or healing (Clarke & Kadhom, 1988; Moss
& La Puma, 1991; Walding & Andrews,
1995; Regnard & Tempest, 1998; Waller & Caroline, 2000). Our results do support
that quality of care evaluation should be based on the process of care for
the individual dying patients and their caregivers rather than solely on
the outcome of an incident of pressure ulcer.
ACKNOWLEDGMENTS
The authors thank Penny Grossman, Ed.D., Linda Dallam, R.N., G.N.P.,
Catherine Badillo, R.N., G.N.P., Cathy Kalinski, R.N., Mary Schnepf, R.N.,
and James Cimino, M.D. for assistance with survey instrument development.
The authors also thank the participants who shared their clinical
experiences with us. Dr. Zeleznik is supported by a Geriatric Academic
Career Award, U.S. Department of Health and Human Services,
K01-HP00001.