


Introduction
Patients with asymmetrical sensorineural hearing loss are currently investigated by magnetic resonance imaging (MRI) screening in order to rule out tumours of the internal auditory meatus (IAM) or cerebellopontine angle. Acoustic neuroma is the most common such tumour, accounting for 80 per cent of all cerebellopontine angle neoplasms. More than 99 per cent of cerebellopontine angle tumours are benign. Metastatic lesions of the cerebellopontine angle are rare, accounting for 0.2 per cent of all lesions.Reference Brackmann and Bartels1 Breast, lung, kidney, stomach and larynx have been identified as the most common sites of origin for metastases to the temporal bone.Reference Hill and Kohut2 Gadolinium-enhanced MRI scanning is now the accepted ‘gold standard’ for investigation of such tumours.Reference Sidman, Carrasco, Whaley and Pillsbury3
Rapid onset, unilateral, profound sensorineural hearing loss appears to be a common first symptom of tumours of the IAM and cerebellopontine angle. There may also be tinnitus, vertigo or symptoms of imbalance. A worrying symptom which should provoke further investigation in such patients is a mild (House–Brackmann function grade two to three (of six)),Reference Arriaga, Lo and Brackmann4 unilateral facial weakness developing within weeks to months of the hearing loss.
Case report
A 79-year-old man was referred to the ENT team with a six-month history of tinnitus, right-sided profound hearing loss, unsteadiness of gait and, more recently, right facial palsy.
On examination, the patient had a right facial palsy with House–Brackmann grade three of six function. An MRI scan (T2-weighted axial and coronal images, plus T1-weighted axial images both pre- and post-contrast) revealed an enhancing soft tissue lesion lying within the right IAM (Figure 1), consistent with an acoustic neuroma. Pure tone audiography revealed profound, right-sided sensorineural hearing loss.
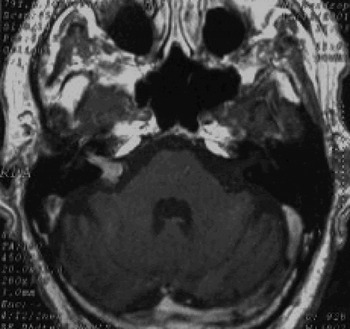
Fig. 1 Axial, contrast-enhanced magnetic resonance imaging scan showing an enhancing soft tissue lesion lying within the right internal auditory meatus. There is also probable enhancement of the geniculate ganglion of the right facial nerve.
The patient was also referred to a urologist due to extremely troublesome lower urinary symptoms, namely poor flow, dysuria and nocturia. On examination, he was found to have an enlarged prostate, together with prostate-specific antigen (PSA) levels of 269.4 µg/l, suggesting an extracapsular prostatic carcinoma. Clinically, he was diagnosed with a tumour4, fixed carcinoma. He was commenced on hormone ablative therapy and was given Casodex (AstraZeneca UK limited, Silk Road Business park, Macclesfield, Cheshire, SK10 2NA, UK) and Zoladex (AstraZeneca UK limited, Silk Road Business park, Macclesfield, Cheshire, SK10 2NA, UK) injections. A bone scan revealed widespread metastases affecting the proximal femoral shafts, proximal humerus, pelvis and spine (Figure 2).

Fig. 2 Bone scan revealing widespread metastases affecting the proximal femoral shafts, proximal humerus, pelvis and spine.
The patient's medical history also included severe ischaemic heart disease, for which he was awaiting coronary artery bypass grafting.
After three months of treatment, the patient's PSA level had dropped from 269.4 to 0.2 µg/l; it reduced further, to <0.2 µg/l at six months, and was still at that level at 20 months.
Two years after presentation, repeat MRI scanning with contrast showed no sign of the enhancing lesion originally seen in the right IAM (see Figure 3). Although initially felt to be typical of a small acoustic neuroma on the first MRI scan, the lesion was thereafter felt to represent a metastasis from the patient's coexisting prostate carcinoma, which resolved on hormonal treatment.

Fig. 3 Repeat axial, contrast-enhanced magnetic resonance imaging scan performed two years after initial presentation, showing no sign of the enhancing lesion originally seen in the right internal auditory meatus.
Clinically, the patient's right facial function improved so that the deficit was barely noticeable (House–Brackmann function grade two of six), and his hearing loss also improved slightly. At the time of writing, following four years of treatment, he enjoyed reasonably good health.
Discussion
Rare cases of metastatic deposits in the cerebellopontine angle have occasionally been reported from various known and unknown primary sources, namely: squamous cell carcinoma, malignant melanoma, malignant parotid oncocytoma,Reference Maiuri, Esposito, Del Basso De Caro and Tortora5 renal carcinoma,Reference Panarese, Turner and Fagan6 and from lung and thyroid primaries. The mechanism of spread is thought to be haematogenous. The current case represents a very rare report of prostatic metastasis in the IAM, which disappeared while the patient was receiving hormone therapy. A single case of a biopsy-proven, solitary prostatic carcinoma metastasis to the internal auditory canal has previously been reported.Reference Ueyama, Kumamoto, Narusako, Fujimoto, Goda and Isono7 We are not aware of any previous reports of resolution of such a lesion with hormonal treatment. If localised, such tumours may be amenable to surgery or other forms of treatment. A complete medical history is therefore important in patients with asymmetrical hearing loss and/or facial palsy. Rapid onset hearing loss and facial palsy are definitive clinical indicators which should prompt investigation for a malignant IAM or cerebellopontine angle tumour, although these tumours have been known to present without facial palsy.
• This paper describes a rare case of prostatic metastasis in the internal auditory meatus (IAM), which resolved with treatment
• Cases of metastatic deposits in the cerebellopontine angle have been described in the literature, from various known and unknown primary sites. The mechanism of spread is thought to be haematogenous
• Rapid-onset hearing loss and facial palsy are definitive clinical indicators which should prompt investigation for a malignant IAM or cerebellopontine angle tumour
Although there is a considerable amount of published literature on the presence of steroid hormonal receptors in acoustic neuromas,Reference Carroll, Zhang and Black8–Reference Filipo, Petrangeli, Monini, Ortolani, Gulino and Barbara10 no previous case report has suggested that an acoustic neuroma could respond to hormone therapy. Moreover, our patient's original MRI study showed probable enhancement of the geniculate ganglion of the right facial nerve, in addition to the enhancing lesion in the right vestibulocochlear nerve. This finding supports the view that the lesion of the vestibulocochlear nerve represented a metastasis from the prostate carcinoma, with a second small metastasis of the geniculate ganglion of the facial nerve, rather than an acoustic neuroma, with both lesions resolving on the follow-up MRI study.



