


Introduction
Epiglottic or vallecular cysts are usually benign and asymptomatic. However, even those without laryngological symptoms may cause airway obstruction following intubation for induction of anaesthesia.Reference McCarthy, Coppel, Gibbons and Cosgrove1 Presenting symptoms vary with the cyst's size, age and degree of extension into the airway. If symptoms occur, they usually comprise voice change (in adults), stridor (in infants), dysphagia, pharyngeal pain or a foreign body sensation in the throat.Reference Henderson, Denney and Teichgraeber2 Rarely, epiglottic cysts may present acutely with rapidly progressive airway obstruction due to secondary infection.Reference Albert and Ali3 Generally, epiglottic cysts have been treated by the puncture technique or surgical resection.
However, these techniques can result in accidental injury to the cyst wall. As a result, the contents of the cyst may spread throughout the larynx, trachea and pharyngeal cavity. The ideal treatment of epiglottic cysts would involve complete resection without cyst perforation.
We use a completely different approach for the resection of epiglottic cysts, with successful results. Here, we introduce this method, termed the advanced phono-ultra-microsurgical technique.
Method
Firstly, a method of suturing the vocal fold epithelium is established. One difference between the advanced phono-ultra-microsurgical technique and previous techniques of surgical epiglottic cyst resection is that the cyst is sealed off before resection, in order to prevent rupture and spread of contents. To achieve this, we have developed a device to facilitate suturing of the vocal fold epithelium, utilising a knot-pusher.Reference Tsunoda and Niimi4–Reference Tsunoda, Kondou, Kaga, Niimi, Baer and Nishiyama6 This technique allows complete removal of epiglottic cysts. The surgery is performed under general anaesthesia with direct laryngoscopic vision, as per the usual phonomicrosurgical approach.
The advanced phono-ultra-microsurgical technique is as follows. Firstly, the suture thread is placed around the base of the cyst, in a similar fashion to a tonsillectomy snare (Figure 1). Secondly, the suture knot is tightened outside the laryngoscope. Thirdly, using the knot-pusher, the knot is slid down to the base of the cyst (Figure 2). Fourthly, the knot is tightened, the vallecular side of the base is dissected around the entire base of the cyst with surgical scissors (Figure 3) and the cyst with ensnared base is removed. Fifthly, after cyst removal, when the vallecular side of the base is open and the cyst bed visible (Figure 4a), the surface is opened completely and checked for bleeding.

Fig. 1 Laryngoscopic view; suture thread (red arrow) is placed around the base of the cyst, in the manner of a tonsillectomy snare (white arrows = direct laryngoscope).
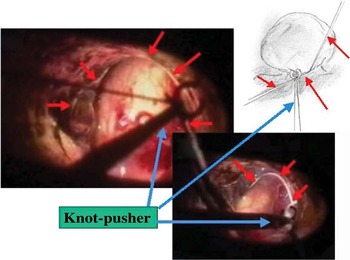
Fig. 2 Laryngoscopic view; using the knot-pusher (blue arrow), the knot is slid down to the base of the cyst. Red arrows = thread (or suture thread).
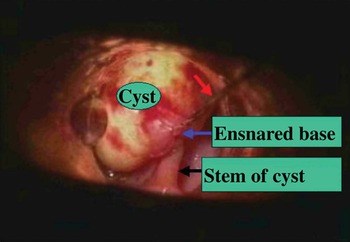
Fig. 3 Laryngoscopic view; the knot is tightened around the ensnared base of the cyst. Red arrow = thread (or suture thread).
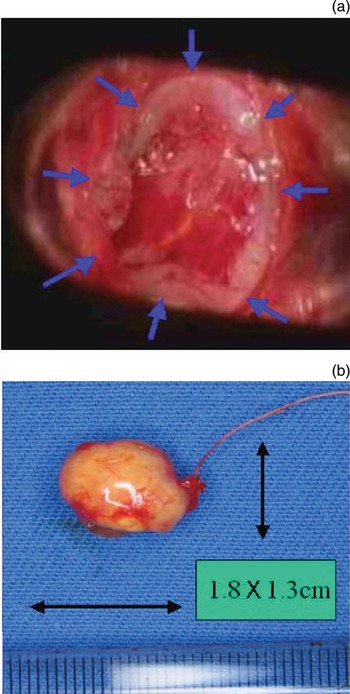
Fig. 4 Laryngoscopic view, (a) After cyst removal, the vallecular side of the base is open and the surface of the cyst bed is visible (blue arrows). (b) A 1.8 × 1.3 cm cyst, removed without rupture.
Figure 4(b) shows a 1.8 × 1.3 cm cyst removed without rupture, using the advanced phono-ultra-microsurgical technique.
We have completely resected three vallecular cysts without rupture, using the advanced phono-ultra-microsurgical technique. One year after removal, none had recurred.
Discussion
Many reports describe resection procedures for epiglottic cysts. In addition, various authors have described the use of a tonsillectomy-style snare,Reference Kawaida, Kohno, Kawasaki and Fukuda7 CO2 laser excisionReference Gutierrez, Berkowitz and Robertson8 and CO2 laser excision after needle decompression.Reference Fang, Cheng and Li9 Although these techniques have yielded clinically satisfactory results, epidermoid carcinoma of the vallecula may be suspected in cases of cervical lymphadenopathy.Reference Assor10 In such cases, our advanced phono-ultra-microsurgical technique is optimal in preventing cyst rupture and spread of contents. Furthermore, such a technique might be useful for the resection for malignant lesions.




