Introduction
Sinonasal organised haematoma is an uncommon, non-neoplastic, benign condition with locally destructive behaviour. Organised haematoma can result from haemorrhage caused by various factors, and progresses via chronic haematoma formation followed by a process of organisation through fibrosis and neovascularisation. Since the first report by Ozhan et al., fewer that 40 cases of sinonasal organised haematoma have been reported in the English literature.Reference Ozhan, Arac, Isik, Oznur, Atilla and Kemaloglu1 This condition most commonly affects the maxillary sinus, presenting as an expansile soft tissue mass with erosion of the adjacent sinus walls.Reference Lee, Park and Heo2–Reference Kim, Kim, Chung, Dhong, Kim and Yim9 Surgical resection is usually curative. Correct pre-operative diagnosis is therefore imperative in order to avoid potentially harmful interventions. Although radiographic evaluation is useful, operative findings and histological evaluation are often necessary to provide a definitive diagnosis.
Here, we report a case of organised haematoma of the sphenoid sinus which mimicked the extrasellar extension of a pituitary tumour.
Case report
An 85-year-old woman with diabetes, hypertension and hyperlipidaemia initially presented at a general hospital complaining of a floating sensation. Magnetic resonance imaging (MRI) was performed to screen for intracranial lesions. This showed a mass extending from the sella turcica into the left sphenoid sinus. The initial diagnosis was extrasellar extension of a pituitary tumour, and radiotherapy was planned. The patient was sent to Kyoto University Hospital for a consultation on the differential diagnosis.
Rhinoscopy revealed deviation of the nasal septum, but there were no notable findings (such as discharge from the sphenoid ostium) in other regions of the nose. The findings of a further head and neck examination were unremarkable.
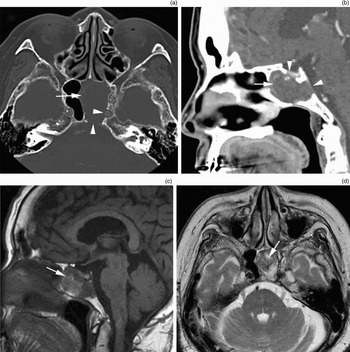
Computed tomography (CT) scanning revealed an expansile soft tissue mass in the left sphenoid sinus, with bony destruction of the lateral and posterior walls of the sinus (Figure 1a). Contrast-enhanced CT images showed patchy enhancement of the lesion (Figure 1b). No calcification was identified within the mass lesion. T1-weighted MR images showed a mass with heterogeneous intensity (Figure 1c), while T2-weighted MR images revealed that the mass contained high-intensity regions and a hypointense peripheral rim (Figure 1d). These radiographic findings were compatible with extrasellar extension of a pituitary tumour and an intratumour haemorrhage. Sphenoid fungal sinusitis was also included in the differential diagnosis.

Fig. 1 (a) Axial computed tomography (CT) and (b) sagittal, contrast-enhanced CT images, showing a heterogeneous mass (arrow) with bone erosion (arrowheads). (c) Sagittal, T1-weighted and (d) axial, T2-weighted magnetic resonance images, showing a heterogeneous mass with highly intense regions within the mass (arrows).
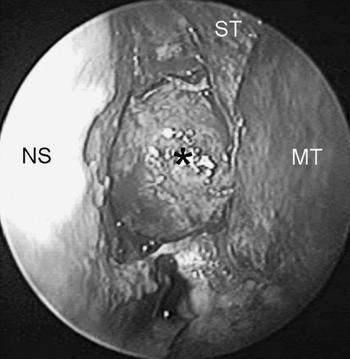
The patient underwent endoscopic, transsphenoidal excision of the tumour under general anaesthesia. A mucoperiosteal flap on the left side of the nose was separated from the nasal septum and the anterior wall of the sphenoid sinus. The bone of the anterior wall of the sphenoid sinus was thickened. Removal of the anterior wall of the sphenoid sinus and the vomer exposed a mass occupying the left sphenoid sinus (Figure 2). An incision was made in the tumour capsule and the contents were removed. These consisted of dark brown fluid and necrotic and fibrous tissues. Histological examination of a frozen section demonstrated coagulation and regions of old haemorrhage surrounded by fibrous tissues, indicating organised haematoma. After removal of the tumour contents, the capsule was subtotally excised. As the tumour had strongly adhered to the exposed dura mater in the hypophyseal fossa and the prominence of the internal carotid artery, the fibrous tissues of the capsule were left in place at the points of attachment. No cerebrospinal fluid leakage or bleeding occurred during the surgery.

Fig. 2 Endoscopic view of the sphenoid tumour. An expansile tumour is seen to occupy the left sphenoid sinus (asterisk). ST = superior turbinate; NS = nasal septum; MT = middle turbinate
Microscopic examination of the surgical specimen identified regions of old haemorrhage surrounded by fibrous tissue and neovascularisation (Figure 3), consistent with an organised haematoma.

Fig. 3 Photomicrograph of the surgical specimen, showing old haematoma (arrowheads), fibrous tissue (white arrows) and vascular neogenesis (black arrow) (H&E; ×40).
The patient had an uneventful post-operative course. No recurrence was detected during the three-month follow-up period.
Discussion
Although the aetiology of sinonasal organised haematoma has yet to be elucidated, it is believed to originate from an accumulation of blood in the paranasal sinus due to various factors.Reference Lee, Park and Heo2–Reference Yoon, Kim and Cho6 Regardless of the initial cause of the bleeding, poor ventilation and drainage, accompanied by the formation of a fibrous capsule, prevent reabsorption of the haematoma, resulting in neovascularisation and fibrosis with recurrent intracapsular bleeding, eventually leading to the development of an organised haematoma. This process accounts for the progressive expansion and the local bony erosion associated with organised haematoma.
Correct pre-operative diagnosis of sinonasal organised haematoma is essential for therapeutic planning, because complete surgical resection by endoscopic sinus surgery or the Caldwell–Luc operation is usually curative.Reference Lee, Smoker, Lee, Kim and Cho3, Reference Yoon, Kim and Cho6, Reference Song, Jang, Chung and Lee7 However, organised haematoma of the maxillary sinus might be mistaken for a malignant or locally aggressive neoplasm, as it can present as an expansile soft tissue mass with erosion of the adjacent sinus walls. In the present case, an expansile soft tissue mass in the sphenoid sinus with bony erosion mimicked a pituitary tumour with extrasellar extension.
It is thus essential to be aware of the characteristic signs of sinonasal organised haematoma on CT or MRI. The reported CT features are relatively nonspecific. Typically, such a lesion appears as a large mass causing expansion of the sinus with bony erosion and heterogeneous high attenuation on precontrast CT scans.Reference Lee, Smoker, Lee, Kim and Cho3, Reference Yoon, Kim and Cho6–Reference Kim, Kim, Chung, Dhong, Kim and Yim9 Patchy or papillary enhancement on contrast-enhanced CT images is also one of the characteristic findings for sinonasal organised haematoma, and was observed in the present case.Reference Lee, Smoker, Lee, Kim and Cho3, Reference Nishiguchi, Nakamura, Mochizuki, Tokuhara, Yamane and Inoue8, Reference Kim, Kim, Chung, Dhong, Kim and Yim9 Magnetic resonance imaging provides a better view of the internal characteristics of the lesion, by demonstrating various signal intensities. The heterogeneous signal intensity on MR images reflects the various components of the lesion, including distinct stages of haemorrhage and fibrosis and differing amounts of vascular proliferation. Song et al. described a hypointense peripheral rim revealed on T2-weighted images of all their studied lesions, which corresponded histologically to a fibrous pseudocapsule.Reference Song, Jang, Chung and Lee7 These MRI characteristics were also identified in the present case.
• Sinonasal organised haematoma is an uncommon, non-neoplastic, benign condition with locally destructive behaviour
• This paper describes the case of an expansile soft tissue mass in the left sphenoid sinus presenting with bony destruction of the sella turcica, which mimicked the extrasellar extension of a pituitary tumour
• Organised haematoma should be included in the differential diagnosis of extensive sphenoid lesions
To our knowledge, this is the first published report on organised haematoma of the sphenoid sinus. Our findings indicate that organised haematoma should be included in the differential diagnosis of an expansile mass that appears heterogeneous with patchy enhancement on CT and/or heterogeneous with a hypointense peripheral rim on T2-weighted MRI, in the sphenoid sinus as well as the maxillary sinus. Histological examination is essential for definitive diagnosis. Surgical decompression with partial resection of the capsule wall to spare vital structures has thus far proved to be an effective treatment.