In emergencies, people with disabilities and those in other vulnerable groups face unique and increased risks that are often overlooked. It is vital to address these needs in emergency planning and create accessible emergency procedures that can save the lives of all residents of any affected region. 1
The Federal Emergency Management Agency (FEMA) defines individuals with functional needs as people of any age with physical, sensory, mental, cognitive, and/or intellectual disabilities that may challenge their ability to function without assistance. 1 More than 12% of the US population has a functional need, and many have multiple needs.Reference Brault 2 Historically, inadequate emergency planning has led to disparate treatment and denial of equal services to those with functional needs.Reference Kailes and Enders 3 It is the responsibility of emergency planning organizations and stakeholders to provide the best skilled care in serving vulnerable populations. 1 , Reference Robinson, Gerber, Eller and Gall 4
Federal law requires the integration and equal opportunity for individuals with functional needs in emergency situations. 5 The St Louis County Department of Health (DOH) directed the St Louis regional distribution/dispensing exercise to assess the capabilities of St Louis County to adequately integrate and provide equal opportunity for those with functional needs in the specific scenario of mass prophylaxis.
In St Louis County, approximately 114 548, or 11.6% of the population has a functional need (Figure 1). Of these, 17 695 people (1.7%) have a vision disability, 30 653 (3%) have a hearing disability, 45 256 (4.5%) have a developmental disability, 62 136 (6%) have mobility needs, and 9949 (1%) are considered to be linguistically isolated, that is, needing translation (written assistance) or interpretation (verbal assistance). 6 , 7

Figure 1 Population of St Louis County With a Functional Need.
The Centers for Disease Control and Prevention (CDC) fund each state and large metropolitan area to prepare for a bioterrorist attack for which antibiotics would need to be dispensed to an entire population in the affected region within 48 hours. The current scenario involves dispensing antibiotics to treat the effects of an aerosolized anthrax attack; however, the same planning model would apply to any need for mass dispensing or vaccination. 8 , 9
The federal requirements include developing exercises to test the jurisdiction’s preparedness. St Louis County has conducted previous exercises to determine its ability to distribute medication to a general population, publicize the points of dispensing (PODs), and transport medical supplies and other competencies outlined for health departments. In recent years, it has been reported, both locally and nationally, that inadequate focus has been given to ensuring access for those with functional needs, a key element in ensuring coverage for the entire affected population.Reference Kailes and Enders 3 , Reference Koh, Elqura and Judge 10 In May 2013, the county addressed this gap by assessing its ability to efficiently dispense medication to individuals with functional needs using the national POD model. 11
The importance of this exercise was to inform St Louis County, as well as other interested emergency planners nationally, of the nuances involved in integrating functional needs services into a mass prophylaxis event. Previous literature on the topic has been limited. Organizations such as FEMA, the National Council on Disability, and the Department of Justice have provided overarching guidelines on preparedness and access issues in accordance with the Americans With Disabilities Act (ADA). 1 , 12 – Reference Davis and Styron 14 This guidance includes providing wheelchair accessibility, creating partnerships between government agencies and community-based organizations, and developing individual emergency plans for those with disabilities. Many resources outline steps for preparing accessible emergency shelters, such as ensuring services and addressing toilet needs and mental health issues. 1 , 12 – Reference Davis and Styron 14 To our knowledge, this is the first article to document a comprehensive set of practical lessons for addressing functional needs when providing life-saving medications or vaccines in a mass dispensing venue. Leveraging such lessons can inform future planning and policy efforts incorporating functional needs into mass prophylaxis planning.
Methods
Setting Up an Open Point of Dispensing
In keeping with federal oversight, 11 , 15 the exercise was held at a public space; in this case, it was a municipal community center. In a real event requiring antibiotic or vaccine dispensing, a POD would include stations such as greiage (greeting and triage), first aid, registration, screening, dispensing, and a separate functional needs station that would combine many of these stations into one. In this exercise, the layout was designed for maximum efficiency in dispensing emergency medications.
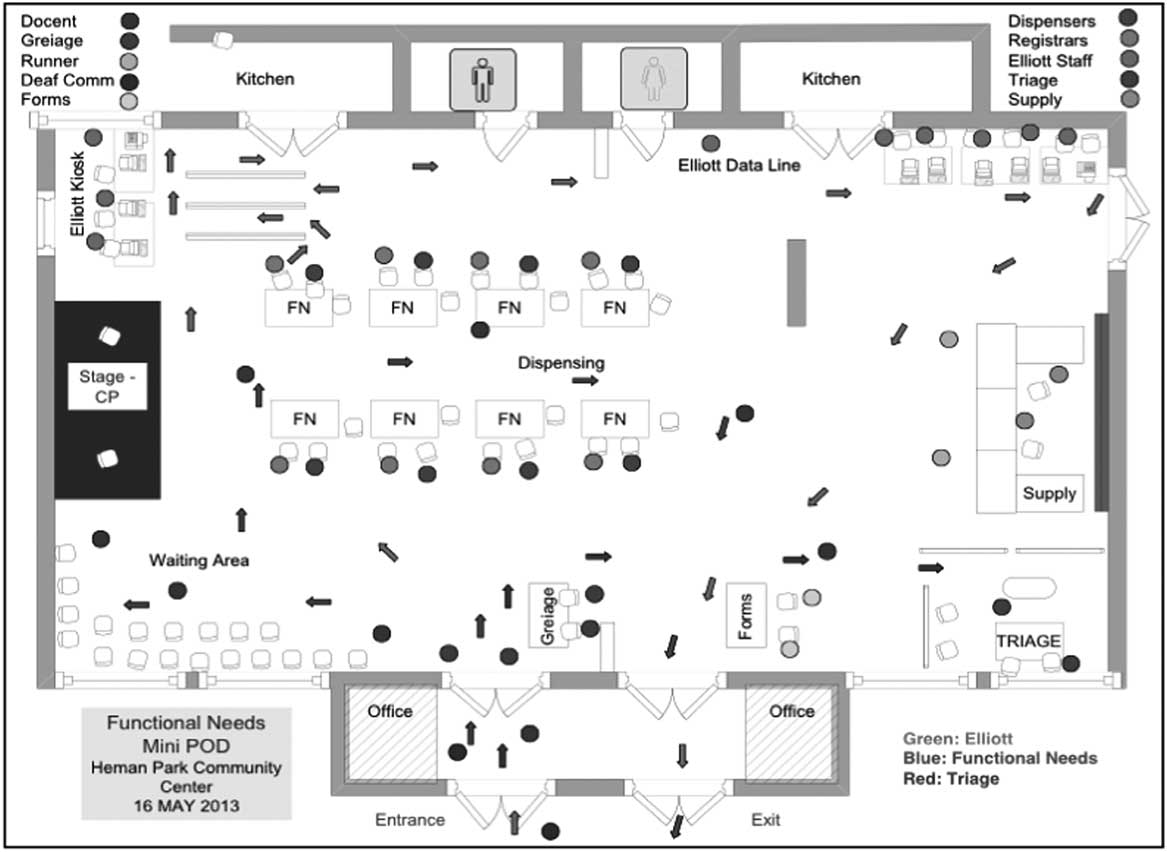
For the purpose of determining functional needs capabilities for this study, this particular exercise devoted an entire POD to functional needs services, meaning that every station (aside from a computerized lane) was prepared to meet the needs of each participant regardless of the nature of the need (Figure 2). Modeled after the setup of a functional needs process within a traditional POD, participants entering this POD went through only 2 stations: greiage and a second station to register, complete paperwork, and receive bottles of medication. The POD also included a lane intended to test a computerized dispensing system, which used other recruited participants who were without functional needs.
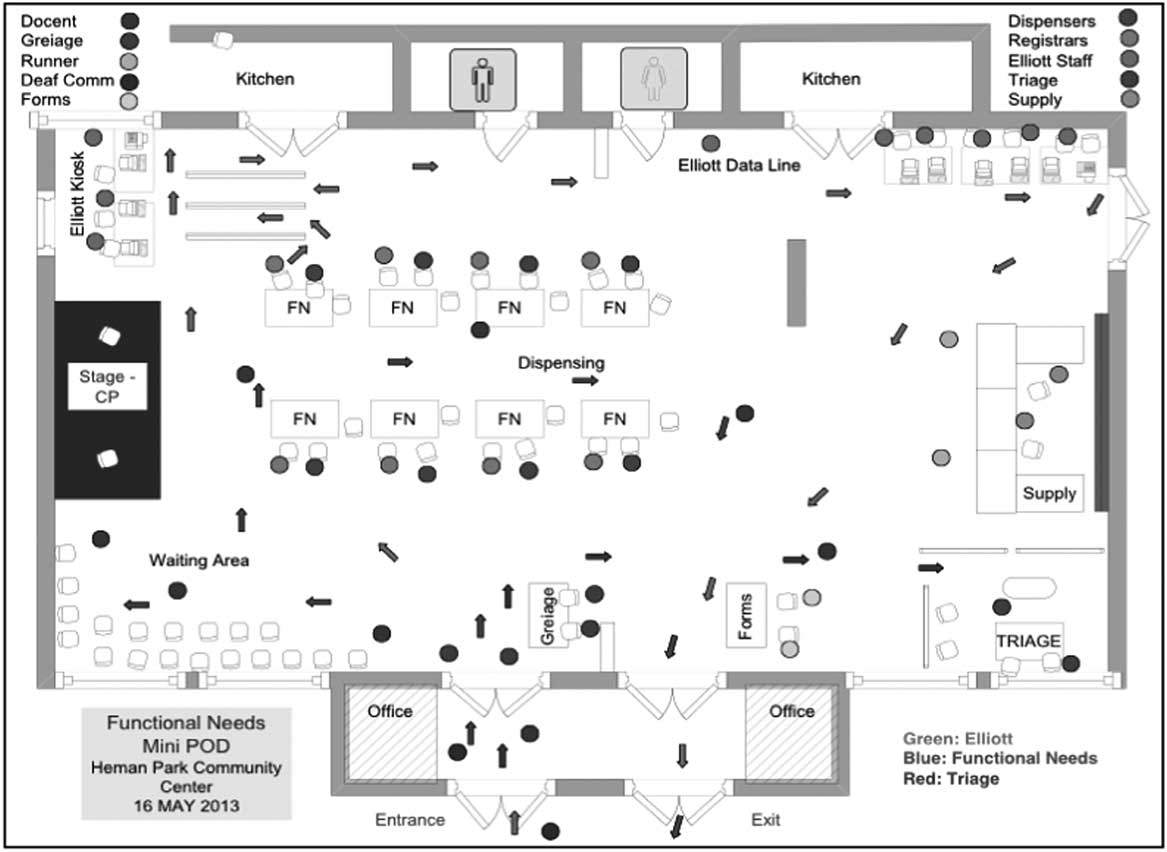
Figure 2 Open Point of Dispensing (POD) Floor Plan.
Stakeholder Engagement
New partnerships were developed with various service organizations in the St Louis region. Planners reached out to the agencies that assist individuals with disabilities and met with representatives of communities with hearing, vision, language, mobility, and developmental disabilities. While most of these key representatives were individuals with functional needs, several had a close relative or friend with a functional need, or worked closely with people who had functional needs through a service organization. The representatives were actively sought for their input regarding education on the needs of the disabled and on POD setup with these needs in mind. Before the exercise, 11 interviews and 1 focus group were held to determine the steps in setting up the exercise. Partners were invited to the planning meetings, and several gave talks to staff members on the best practices to provide functional needs services during a mass prophylaxis event.
Development of New Policies and Procedures
When walking through a POD to obtain medication, someone without a disability would typically follow signage, fill in a health assessment form, receive fact sheets about the agent and the medication, and take home a prescription bottle of medication that has instructions on it. For many people with functional needs, this process poses issues and requires specific adjustments to allow equal access.
To keep the exercise manageable, planners identified 5 types of functional needs on which to focus: low vision, low hearing, limited English proficiency, mobility, and developmental needs. In accordance with suggestions from representatives of the functional needs community, the following changes were made during the POD planning to address these needs.
Low Vision
Magnifiers were provided to facilitate reading the information sheets, forms, and other materials. All fact sheets and health assessment forms were provided in braille and large print. While small-print instructions were printed on bottle labels, the Department of Health provided tags resembling door hangers that fit around the neck of the bottle. These tags featured braille instructions on one side, and large-print instructions on the other.
In an emergency situation, entire families would pick up medication, providing 1 bottle per person. In the case of an anthrax threat, different medications (ciprofloxacin or doxycycline) may be distributed to each individual, depending on the health assessment. It is important for those with low vision to identify their own bottle. To address this, plastic sticky bumps were placed on the bottles for those with low vision to distinguish their bottle from others in their household.
Low Hearing
When involved in the POD traffic flow, many individuals would be listening for instructions. Certain accommodations were needed so that people with low hearing would be able to understand the situation and follow instructions to obtain their medication. Because some individuals with low hearing use language and others do not, a range of accommodations was provided.
So-called communication books featured pictorial descriptions of the signs and symptoms of anthrax as well as the health assessment questions. Signage was set up to explain the process of the POD using pictorial images.
An interpreter wearing a black vest featuring the symbol for American Sign Language (ASL) was available for assistance. A statement, along with the ASL symbol, was placed on the health assessment form, indicating that an ASL interpreter would be available. In addition, one tactile interpreter was present for those who were both blind and deaf.
For those who could not read these directions, 2 nonvocal communicators were available for those waiting for an interpreter. It is anticipated that anxiety and confusion would be high during a public health emergency. The purpose of the extra communicators was to minimize this confusion and keep all participants informed throughout the entire POD process. Since interpreters are limited, it was necessary to have other communicators available.
Limited English
Planners incorporated signage in the 8 most commonly spoken languages in St Louis County other than English: Vietnamese, Russian, Korean, French, Spanish, Bosnian, Chinese, and ArabicReference De Voe and Mertz 16 A sign at the front entrance identified spoken languages in each specific language. Fact sheets and the health assessment form were provided in each language.
A telephone language line service was made available for those who needed further interpretive services. Signs throughout the POD in 94 different languages were used to identify the client’s spoken language. Another sign indicated that an interpreter would be available by phone who could translate for 8 of the most common languages spoken in St Louis County.
Mobility
According to ADA regulations, 17 the tables were set at a height of 74 cm, with 150 cm between rows of tables, allowing room for wheelchairs to move through lines and have people sitting comfortably at station tables. Also provided were pen grippers, clipboards, straws, and a signature plate to assist with writing names on the forms. Adequate numbers of staff were at the stations ready to assist. Waiting areas were chosen strategically to allow for space and so that those in wheelchairs were not segregated from others who were waiting.
Developmental Disabilities
Along with conversations with representatives from the developmental disability community, several outside resourcesReference Goldstein, Winkler and Chun 18 – Reference McVeigh 20 informed etiquette guides to help staff work with clients with developmental disabilities. The training included instructions on providing a quiet environment, talking directly to the client and responding appropriately, using clear and specific language, practicing patience and repeating necessary items, condensing instructions, and using hands-on instructions. Materials were also written to remind staff to be cognizant of differences and take time to determine each person’s mental capacity and communication skills.
Just-In-Time Training
In a real event, POD staff members are predominantly volunteers with basic training to assist the community at a time of need. These volunteers are not necessarily trained before the event to serve people with functional needs but would need this capability in the event of an emergency. For this exercise, planners had developed just-in-time training materials for volunteers, with specific instructions for the day of the event. Figure 3 shows an example of a training card used to assist staff in working with individuals with low vision.

Figure 3 Example of Just-in-Time (JITT) Training for a Medication Dispenser.
Sources for these guidelines came from interviews with representatives from functional needs community organizations in St Louis, as well as online sources such as the Washington State School For the Blind, 21 Missouri Developmental Disabilities Council,Reference McVeigh 20 the US Department of Justice, 13 and the CDC. 22
Trainings included instructions on how to call the foreign language phone line, asking each patron if they needed assistance, and how to subsequently touch the arm of a person with low vision to assist that person in easily locating the guide’s elbow for walking assistance. Instructions on functional needs services were interwoven with instructions on how to dispense medication properly to each individual.
Feedback Collection and Policy Adjustment
Eight staff members and an additional 7 designated evaluators and observers submitted written evaluation forms with comments in narrative form. This feedback was vital to understanding the successful initiatives and identify in what situations staff struggled to meet the needs of the participants. Feedback from the functional needs participants was obtained through 3 focus groups and 6 interviews to collect qualitative feedback on the areas that succeeded and those that needed improvement.
Feedback was provided from nearly all participating individuals with low hearing and low vision, from 88% of participants with limited English proficiency, and from 18% of participants with mobility needs. Because people with developmental needs were difficult to reach after the exercise, an individual who serviced those with developmental needs provided feedback in an interview. Despite this limitation, valuable lessons were identified from the given comments that proved useful for future planning. Mistakes were catalogued and changes were adopted to put into the DOH’s current policy and emergency operations plan. This plan will be used to develop future exercises and provide policy on which to act in the case of an emergency.
Results
The exercise produced real scenario events that were successfully addressed. In spite of an unexpected delay in setting up, 100% of the 40 participants were dispensed medication. This included 4 participants with low vision, 10 with low hearing, 8 with limited English proficiency, 11 with mobility needs, and 4 with developmental needs. From feedback discussions, 35.9% of comments reflected communication issues, 29.3% of comments reflected staff training issues, and 34.8% of comments reflected overall exercise preparedness, which some thought could have been more robust. Participant feedback was divided into categories based on functional need. Table 1 outlines each type of comment and the number of times each issue was raised through open-ended feedback.
Table 1 Exercise Feedback by Need Category and Number of Comments per Comment Type

Low Vision
Successes included a variety of measures for participants with low vision. The door hanger-shaped applications that fit onto the bottles were applied with no problem and addressed the needs of the participants. All materials in braille were both useful and correct. Furthermore, staff members were cognizant of giving verbal directions throughout the exercise.
Several issues caused problems or prompted suggestions from participants. The provided magnifiers were blurry and useless. Although large-print documents were ready at the supply table, they were never brought to the dispensing tables and were not available to some participants. In addition, verbal identification of staff was needed, as vest colors were not seen by participants with low vision.
Recommendations from participants included enhanced instructions in disability sensitivity for the staff members and materials to address visual needs. For example, one participant noted, “Telling a blind person to ‘go over there’ is not helpful.” As far as materials, most people who are blind and do not read braille can benefit from large print or a pair of reading glasses. Also, staff members should not assume that participants can read braille, and they should read paperwork aloud to participants. A new suggestion was to crease the paper on any signature line, so the person writing would have a guide on which to write.
Low Hearing
Participants with low hearing reported experiencing more confusion than those with low vision, and they had a number of suggestions. Complaints included too much background noise, overlooked signage at the entrance, and a correction to one of the pictures on the communication board was not understandable. Confusion was due to multiple instructions and steps in the process. As one participant explained, there were “too many different instructions given and we felt lost.” While colored lines on the floor were intended to direct participants, some found them confusing.
To offset the background noise, participants suggested the use of a microphone. It was also suggested that a pen and paper be provided at each station, allowing deaf individuals to communicate with staff in the absence of an interpreter.
The need for interpreters posed a significant challenge. A sign language interpreter would need to be assigned per station. Interpreters are expensive and scarce. Because only 3 interpreters were available at this exercise, the demand was overwhelming. In the case of a real event, other PODs may need interpreters at the same time, which would cause a regional shortage of interpreters. Knowing this, one participant suggested “having deaf staff members assigned to specific areas... to explain to deaf individuals what to expect.” It would be beneficial for deaf staff members to explain the use of antibiotics and their side effects to deaf clients, because many individuals with low hearing did not read the handout, as intended. Moreover, an interpreter for deaf and blind persons should be made available.
Limited English Proficiency
The most successful aspect of the language access measures was the provision of the telephone language line service. It provided accurate and correct translations to the staff and non-English speaking clients. This language line enabled correct dispensing decisions.
Specifically in reference to this group, an inadequate amount of time was given to just-in-time training. Staff members mistakenly directed functional needs clients to the electronic dispensing lane, where the staff were not trained to provide interpreters for non-English speaking clients. In addition, staff members need to recognize the difference between a sign language interpreter and a language interpreter. One staff member mistakenly sought the help of a sign language interpreter to translate for a foreign-born individual.
In terms of staff training, one of the most challenging aspects was identifying needs. Staff members should be reminded to look for persons with language differences, and be ready to respond accordingly. Next, staff members need to understand that medical communications are more sensitive than everyday conversations, and require level 5 qualified translators to ensure full understanding. A participant noted, “Another staff person relied on a student who spoke some Spanish to interpret for the Spanish speaker. Again, this is ok for non-medical communications, but you should always use a qualified or trained interpreter for medical communications.”
Finally, due to the cumbersome nature of passing the translator service line telephone back and forth, a participant recommended investing in a tool in which people with limited English proficiency could use headphones and speak to the translator simultaneously.
Mobility
Few comments were provided on mobility measures, as participants were able to easily communicate with staff, and the ADA guidelines ensured that the POD was prepared to address their needs. Suggestions were made to allow more physical space for people with wheelchairs, guide dogs, or children accompanying a person with mobility needs. While tables were set at vertical requirements, a participant explained, “we need to think more horizontally, not just vertically.” Also, provisions were not made to address those who may have trouble leaving their cars. A suggestion was made to instruct runners to complete the paperwork and dispense medication at the car to improve efficiency.
Developmental Disabilities
Recommendations to improve access for those with developmental disabilities were focused on increasing awareness and training of staff members. Staff members experienced difficulty with effective communications, as demonstrated by a staff comment that an individual “wanted to keep his bag and did not understand why he had to turn it back in.” Since developmental disabilities are so varied, the challenges were in creating tools that would address everyone’s needs. The participants with these disabilities ended up walking through the traditional electronic dispensing line as a group. In reality, these participants should have gone through the regular, non-computerized, functional needs dispensing line.
Overall Staff Training
Additional recommendations for staff training not mentioned here included the need for more sensitivity training overall. Too many staff members mistakenly told people with low vision to “look for staff with vests” or follow where their hand was pointing. Increased explanation of why the drugs being dispensed was needed, and participants were not familiar with the medical names of the drugs, which were used casually. Specific drugs and their nature needed to be explained more in depth. It was suggested that staff be given more training in speaking through an interpreter.
Furthermore, a toolkit is needed to standardize evaluating exercises. Standardized just-in-time training exercises could limit the confusion among participants and staff members. For instance, staff members should not to tell people with low vision to cut between tables if no one else can do so. Also, instead of telling participants with low vision to look for people in vests, it is better to tell them to raise their hand if they need help.
While this exercise only measured activity inside the POD, it is necessary to note that other exercises have addressed the publicity of such PODs for functional needs, especially through social media channels. While some participants came with assistance, most used dial-a-ride services or public transportation, which enabled staff to test their own proficiency in serving the individuals directly. It was assumed that many who could not come to the POD with family members or attendants would use dial-a-ride, carpools, or public transportation, as in typical scenarios.
Discussion
The St Louis County exercise produced a number of valuable lessons for future emergency response planning. Overall, these findings highlighted the importance of working closely with the functional needs community to incorporate methods and technologies into the POD setup and staff training, reinforcing FEMA’s recommendations to include people with functional needs and agencies that serve and advocate for them into each planning stage. 1 The positive relationships formed with the local community allowed emergency planners and county officials to continue to better partner with them and provide functional needs services. The results also pointed to the power of engaging functional needs participants in the POD exercise itself. Through increased understanding of both successes and shortcomings, this exercise demonstrated the importance of staff training, including adequate just-in-time training materials and proper resources for understanding functional needs. In addition, this approach was in line with Boston’s mass prophylaxis plan, as understanding proper just-in-time training can facilitate POD flow and the ability to serve everyone’s needs in a short period of time.Reference Koh, Elqura and Judge 10
Due to the success of previous exercises that focused on the entire community and the focus of this exercise on functional needs services, traffic flow was not calculated, as would be typical. It was, however, determined that a typical POD in a real event would require 3 stations dedicated to functional needs, rather than the 1 originally predicted. This requirement was identified based on the level of confusion, demand for staff members, and time dedicated to each individual. The station calculation aligned with national guidelines for mass antibiotic dispensing infrastructure that suggest the use of separate “assisted” dispensing areas 11 within an all-inclusive community open POD.
Furthermore, as emergency preparedness initiatives are developed and planned to provide access, the need for standardization of POD activities is demonstrated. This identified need is primarily critical for planning efforts and staff training so that the dispensing activities can run as smoothly as possible. For this reason, the findings of this study point to many actions that future POD planners may use. Lessons and recommendations specific to each functional need are described in Table 2.
Table 2 Summary of Lessons Learned Based on Functional Need

Finally, an overarching lesson was to train staff members to recognize differences and use the appropriate resources, such as obtaining an interpreter and speaking to someone using one. Future exercises should involve a diverse community to expose staff members to many possible scenarios.
Conclusions
The lessons learned from the St Louis County exercise can provide critical guidance for future POD planning policies and initiatives. Understanding the actions necessary to provide equal opportunity and access is an important step in increasing the effectiveness of future mass prophylaxis programs. These lessons are available to assist emergency planners in program improvement, as they continue to work with agencies that serve persons with functional needs and bring them into planning efforts as partners.
Limitations of this study lie primarily in the lack of information and feedback on mobility and developmental needs, as well as a standard exercise evaluation method. For the developmental group, this deficit was partially due to less robust relationships with the community groups as well as small numbers of participants. Because the mobility group was more successful in navigating the POD, they provided fewer complaints and comments. Further research should continue on the needs of individuals with mobility and developmental disabilities in mass prophylaxis events, and on the formation of long-term partnerships with community organizations. Future exercises would benefit from developing a standardized method of evaluating participant experiences and recommendations to quantify and further analyze results of such efforts.