


Case summary
An 11-month-old child presented to the emergency department with inspiratory stridor. He had no other medical conditions or immunodeficiency. He was born at term by normal vaginal delivery. He underwent microlaryngoscopy, which confirmed the presence of laryngeal papillomas involving the vocal folds, epiglottis and false cords (Figure 1). He underwent surgical debulking using a microdebrider and carbon dioxide (CO2) laser. Initially, he required surgical debulking every four weeks to maintain an adequate airway. The requirement for debridement gradually progressed to becoming necessary every three weeks. Now, six months after his initial presentation, he requires surgical debulking every fortnight. The papillomas have extended to involve his subglottis (Figure 2). Adjuvant treatments have not been used at present. We review the literature to identify the surgical and adjuvant therapies that have been used in this age group.
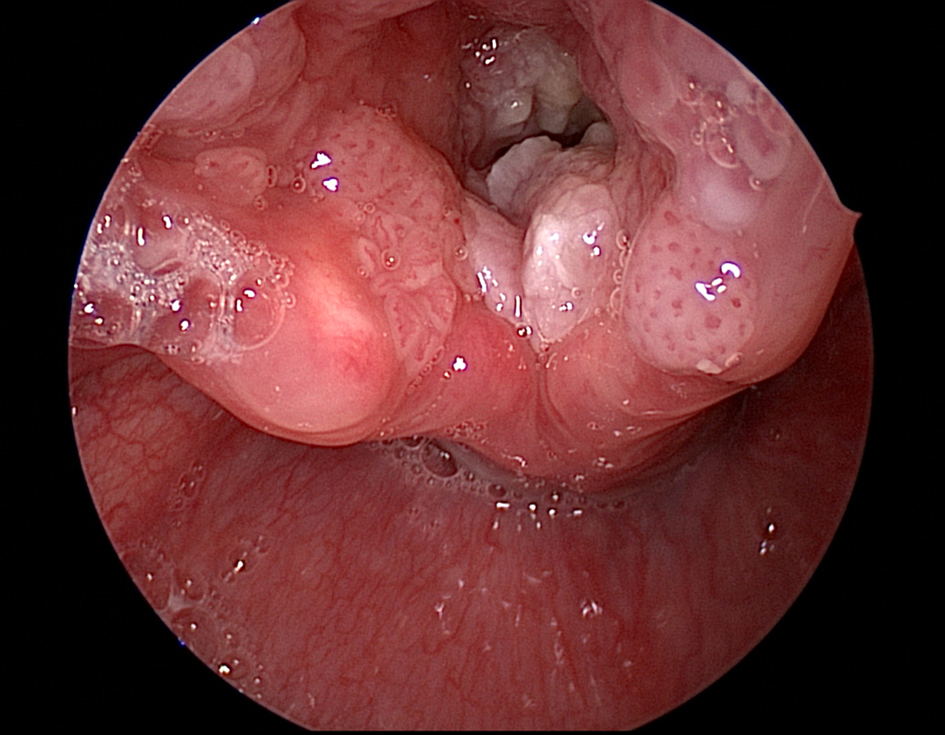
Fig. 1. Evidence of laryngeal and supraglottic papillomas.

Fig. 2. Evidence of subglottic papillomas.
Introduction
Recurrent respiratory papillomatosis is an uncommon condition characterised by the growth of exophytic lesions within the larynx and trachea. It presents with hoarseness or stridor and carries significant morbidity. Currently, the principal aim of management is maintenance of an adequate airway with surgical debulking. This process is repeated at appropriate intervals whilst awaiting spontaneous resolution of the condition. A number of adjuvant therapies have been used with varying effect to expedite the cessation of papillomas.
Recurrent respiratory papillomatosis is categorised as juvenile-onset or adult-onset.Reference Wiatrak1 In the paediatric population, the incidence varies between 2 and 4 per 100 000.Reference Derkay2,Reference Larson and Derkay3 Juvenile-onset recurrent respiratory papillomatosis is more aggressive than the adult-onset form. The most severe cases present in children aged under three years.Reference Armstrong, Derkay and Reeves4,Reference Derkay and Darrow5 Children under three years are 3.6 times more likely to require at least four debulking procedures per year.Reference Armstrong, Derkay and Reeves4
The papillomas are histologically benign. Recurrent respiratory papillomatosis is caused primarily by human papilloma virus (HPV) types 6 and 11.Reference Mounts, Shah and Kashima6 Several studies have supported the theory of vertical transmission from affected mothers.Reference Silverberg, Thorsen, Lindeberg, Grant and Shah7,Reference Shah, Kashima, Polk, Shah, Abbey and Abramson8 Vaginal warts are also caused by HPV types 6 and 11, which supports the hypothesis of vertical transmission from mother to child during childbirth. However, recurrent respiratory papillomatosis has also affected children born by caesarean section, and this raises the possibility of in utero transmission.Reference Shah, Kashima, Polk, Shah, Abbey and Abramson8,Reference Loyo, Pai, Netto and Tunkel9 Caesarean section does reduce the risk of recurrent respiratory papillomatosis by more than four times.Reference Shah, Stern, Shah, Bishai and Kashima10
Most commonly, the exophytic lesions are confined to the larynx, but they can be seeded into the trachea, bronchi and oesophagus. Rarely, recurrent respiratory papillomatosis can be fatal, mostly because of acute airway obstruction, diffuse bronchopulmonary spread or malignant change.Reference Solomon, Smith, Kashima and Leventhal11
Adjuvant therapies are traditionally considered when more than four to six debridements are required per year. Several medical adjuvant treatments have been used for recurrent respiratory papillomatosis in both juvenile and adult-onset cases, although none has demonstrated a curative result.Reference Wiatrak1 Recent systematic reviews are available on adjuvant therapies in paediatric recurrent respiratory papillomatosis.Reference Soma and Albert12–Reference Shehab, Sweet and Hogikyan14 Given that the most aggressive recurrent respiratory papillomatosis presents in the youngest children, it is most likely that a child within this age group would need to be considered for adjuvant therapy. Therefore, the current evidence base on adjuvant treatments relating to children who present under three years of age has been reviewed. This appraisal can augment the existing published literature that has already examined adjuvant therapies in wider age groups. Together, they can assist clinicians in applying evidence-based medicine to this complex clinical case.
Methods
A literature review of articles in Cochrane, PubMed and Embase databases was carried out. Abstracts were then studied, and articles that focused on the management of recurrent respiratory papillomatosis in children aged under three years were included. The references of qualifying articles were also searched for relevant papers. We excluded articles if the patient's age at first presentation was unclear or was greater than three years.
Results
The papers that met the inclusion criteria have been summarised in Tables 1 and 2. Given the rarity of the condition in its infantile form, all the literature relates to case reports and case series.
Table 1. Summary of case reports relating to adjuvant treatments used in recurrent respiratory papillomatosis in children aged under three years

*After initiation of adjuvant therapy. Mth = months; HPV = human papilloma virus; y = years; PEG-IFN = pegylated interferon
Table 2. Summary of case series relating to adjuvant treatments used in recurrent respiratory papillomatosis in children aged under three years

*Since last injection. Mth = months
No randomised, controlled trials or systematic reviews have been carried out on this specific age group. For completeness, relevant randomised trials and systematic reviews have been summarised in Table 3, although these do not isolate the results in children aged under three years specifically.
Table 3. Summary of controlled trials or systematic reviews*

* These reviews do not relate specifically to children aged under three years. RCT = randomised, controlled trial; IFN = interferon
Discussion
Recurrent respiratory papillomatosis presenting under three years of age represents the most aggressive form of the disease.Reference Armstrong, Derkay and Reeves4 Given the relative rarity of this condition, most literature relates to level 4 and 5 evidence in the form of case reports and small case series. The knowledge base is strongly dependent on larger case series, systematic reviews and a few randomised, controlled trials in the older age groups.
Surgical procedures
All the literature confirms the need for regular surgical debulking of papillomas.Reference Wiatrak1,Reference Fusconi, Grasso, Greco, Gallo, Campo and Remacle15,Reference Ivancic, Iqbal, deSilva, Pan and Matrka16 The papilloma bulk is reduced in order to maintain a patent airway and to avoid damaging the underlying tissue. The surgical techniques used include cold steel, CO2/potassium-titanyl-phosphate (KTP) laser, microdebridement or a combination of these.Reference Ivancic, Iqbal, deSilva, Pan and Matrka16 Some reports have indicated the need for tracheostomy, which is not unusual given the aggression of recurrent respiratory papillomatosis in this age group.Reference Ivancic, Iqbal, deSilva, Pan and Matrka16–Reference Maunsell and Bellomo-Brandao18
The risk of laryngeal scarring (anterior/posterior glottis, supraglottis or trachea) with CO2 laser in children is well described.Reference Ivancic, Iqbal, deSilva, Pan and Matrka16,Reference Saleh19 None of the reviewed articles reported any long-term complications relating to the surgical technique in our intended age group. This is most likely related to the short follow-up periods.
Adjuvant therapies
To reduce the burden of this disease and increase the interval between surgical debulking procedures, several adjuvant therapies have been used to varying effect. These therapies have been used in adults and children. Although there is no specific indication for the use of adjuvant treatment, it is widely considered when the need for surgical debulking is frequent (more than four to six times per year) or if the papillomas begin spreading beyond the larynx. In 21 per cent of juvenile-onset recurrent respiratory papillomatosis cases in the USA, an adjuvant therapy is used in conjunction with repeated debulking surgery.Reference Schraff, Derkay, Burke and Lawson20 In 2012, Chadha and James published a Cochrane review update on the use of adjuvant therapies for recurrent respiratory papillomatosis in adults and children.Reference Chadha and James21 They concluded that there was insufficient evidence from controlled trials to support any adjuvant treatment.
The following adjuvant therapies have been used in children who presented under three years of age: quadrivalent HPV vaccine, intralesional cidofovir, pegylated interferon, alpha-interferon, cimetidine and cetuximab.
Quadrivalent vaccine
The quadrivalent HPV vaccine (level 5 evidence) induces antibodies against HPV types 6, 11, 16 and 18. In July 2018, it was announced that this vaccine will be added to the UK vaccination programme for all children aged 12–13 years to protect against cervical and oropharyngeal cancers. This follows the vaccination programme already in place in other countries internationally.Reference Katsuta, Miyaji, Offit and Feemster22 Vaccination aims to generate immunity prior to HPV exposure and thus induce direct protection. There are no known adverse effects from the vaccine at present.Reference Arbyn and Xu23
Recurrent respiratory papillomatosis is principally caused by HPV types 6 and 11.Reference Mounts, Shah and Kashima6 There are four case reports on use of the quadrivalent HPV vaccine in children with recurrent respiratory papillomatosis presenting under three years of age. Following three doses, three cases reported complete remission of papillomas at follow up.Reference Mudry, Vavrina, Mazanek, Machalova, Litzman and Sterba24–Reference Forster, Boltze, Seidel, Pawlita and Muller26 One reported no therapeutic effect.Reference Katsuta, Miyaji, Offit and Feemster22 The proposed mechanism of action is unclear. It is hypothesised that vaccination causes sufficiently high antibody titres to prevent papilloma recurrence following surgical debulking.Reference Young, Moore and Halstead27
Intralesional cidofovir
Cidofovir (level 4/5 evidence) is a cytosine nucleoside analogue. It has antiviral activity against DNA viruses such as HPV. It has been the most widely used adjuvant treatment in recent years. Systemic treatment has been associated with severe adverse effects, including nephrotoxicity and neutropenia.Reference Tjon Pian Gi, Ilmarinen, van den Heuvel, Aaltonen, Andersen and Brunings28 This has been evaluated by Naiman et al., who investigated the systemic cidofovir levels following intralesional application and confirmed that the systemic levels are not high enough to cause toxicity.Reference Naiman, Roger, Gagnieu, Bordenave, Mathaut and Ayari29 Intralesional treatment has been associated with reports of oncogenicity in rodent studies.Reference Shehab, Sweet and Hogikyan14 In humans, there has been no correlation with adenocarcinoma as suggested in animal studies.Reference Shehab, Sweet and Hogikyan14,Reference Dikkers30 There have been reports of verrucous carcinoma in adults, which is argued to be HPV-related as opposed to being induced by cidofovir.Reference Shehab, Sweet and Hogikyan14 However, this requires further investigation with long-term follow up.
A systematic review by Soma and Albert identified complete response rates to intralesional cidofovir in children and adults to be approximately 60 per cent.Reference Soma and Albert12
We have identified 27 children who presented aged under three years who were treated with intralesional cidofovir. These data have been extrapolated from a number of case series and reports (Tables 1 and 2).Reference Milczuk31–Reference Durvasula and Richter38 Five children (18.5 per cent) demonstrated complete response, 11 (40.7 per cent) demonstrated partial response and 11 (40.7 per cent) demonstrated no response. This indicates a variable response to intralesional cidofovir. None of these studies incorporated controls, and thus it is possible that the demonstrated response actually represents the natural history of the condition. Ksiazek et al. described a four-month-old child with laryngeal and pulmonary papillomas who demonstrated complete response to nebulised cidofovir.Reference Ksiazek, Prager, Sun, Wood and Arjmand39
It is important to note that the doses of intralesional cidofovir in these studies are highly variable. This aspect was reviewed by Clamp and Saunders in an attempt to determine a reasonable dosing consensus.Reference Clamp and Saunders13 A response to their paper highlighted that because of the systemic effects of cidofovir, it is not licensed in many countries and therefore should be used with extreme caution.Reference Dikkers40
Alpha-interferon and pegylated interferon
Alpha-interferon (level 5 evidence) is a cytokine with antiviral and anti-proliferative properties. It was the initial adjuvant drug used for recurrent respiratory papillomatosis. Its use has largely ceased following a randomised controlled trial by Healy et al. in 1988, which showed an inadequate sustained response in 123 patients.Reference Healy, Gelber, Trowbridge, Grundfast, Ruben and Price41 Recently, two treatment-resistant infants were treated with alpha-interferon, but neither demonstrated any reasonable improvement.Reference Ksiazek, Prager, Sun, Wood and Arjmand39,Reference Bostrom, Sidman, Marker, Lander and Drehner42
Pegylated interferon is the novel counterpart. It increases the half-life of the drug, reduces immunogenicity and improves the pharmacokinetics. It is significantly more effective than alpha-interferon at treating hepatitis C.Reference Maunsell and Bellomo-Brandao18
One case report is available relating to pegylated interferon.Reference Maunsell and Bellomo-Brandao18 A 14-month-old child with recurrent respiratory papillomatosis was treated with surgical debulking on a 2-weekly basis and required a tracheostomy. The child had no improvement with intralesional cidofovir and developed pulmonary papillomas at the age of three years. The child was intolerant to bevacizumab, and subsequent treatment with pegylated interferon reduced the need for surgical debulking to three-monthly. Unfortunately, because of deranged liver function this treatment was stopped.
• Juvenile-onset recurrent respiratory papillomatosis is more aggressive than the adult-onset form
• Recurrent respiratory papillomatosis presenting in those aged under three years represents the most aggressive form of the disease
• Several adjuvant therapies have been used to varying effect to reduce the burden of this disease and increase the interval between surgical debulking.
• The literature relating to management of infantile recurrent respiratory papillomatosis is based on case reports and small case series
• Quadrivalent human papilloma virus vaccine, intralesional cidofovir, pegylated interferon, alpha-interferon, cimetidine and cetuximab have been used in those presenting aged under three years
Cimetidine
Cimetidine (level 5 evidence) is an H2 receptor antagonist most commonly used to reduce gastric acid secretion. At high doses, it has been noted to have immunomodulatory effects and therefore has been used for cutaneous warts.
One case report has shown a positive response in a child with treatment-resistant recurrent respiratory papillomatosis.Reference Harcourt, Worley and Leighton17 A five-month-old child presented with laryngeal papillomas, which rapidly progressed to the trachea, bronchi and lung parenchyma. A tracheostomy was inserted and regular surgical debulking was carried out by laser. Alpha-interferon, acyclovir and ribavirin were used without any convincing effect over a number of years. At age 10 years, the child underwent treatment with systemic cimetidine, and within 4 weeks had visible improvement in her airway, which has been sustained following cessation.
Cetuximab
Cetuximab (level 5 evidence) is an anti-epidermal growth factor receptor monoclonal antibody. Immunostaining has identified epidermal growth factor receptor-positive cells in 30 per cent of papilloma tissue.Reference Loyo, Pai, Netto and Tunkel9 On this basis, Loyo et al. used systemic cetuximab on an infant with laryngeal and tracheal papillomas.Reference Loyo, Pai, Netto and Tunkel9 The disease progressed despite this adjuvant treatment.
Conclusion
The literature relating to the management of infantile recurrent respiratory papillomatosis is based on case reports and small case series. The majority of papers relate to the successful use of adjuvant treatments, but it is likely that a number of failed treatments remain unreported. The natural history of recurrent respiratory papillomatosis results in spontaneous improvement following the development of immunity. It must be noted that the majority of current evidence does not include any control group to allow for spontaneous improvement. Similarly, several reports have combined adjuvant therapies, which hinders appropriate conclusions.
The decision to use adjuvant therapies must be based on current evidence in full knowledge of the risks and benefits – this must be individualised. None of the adjuvant treatments mentioned are licensed for treating recurrent respiratory papillomatosis. The rarity of the condition does not allow reasonable controlled studies to further evaluate this topic. Therefore, multicentre collaborations will be required to develop powered studies, which can produce valid conclusions and stronger evidence.
Competing interests
None declared





