



The developmental window between early and late adolescence constitutes a period of peak risk for the onset and expression of bulimic symptomatology among girls (Lewinsohn, Striegel-Moore, & Seeley, Reference Lewinsohn, Striegel-Moore and Seeley2000). Bulimia threatens the well-being of as many as 17% of middle school and high school girls (Neumark-Sztainer et al., Reference Neumark-Sztainer, Croll, Story, Hannan, French and Perry2002) and 18% of college girls (Crowther, Armey, Luce, Dalton, & Leahey, Reference Crowther, Armey, Luce, Dalton and Leahey2008), of which an estimated 1.2% to 4% meet full diagnostic criteria for bulimia nervosa (Stice, Marti, & Rhode, Reference Stice, Marti and Rhode2013). Both subclinical and clinical levels of bulimic pathology often take an unremitting course and portend significant functional impairment, psychological distress, medical problems, and long-lasting sequelae (Spoor, Stice, Burton, & Bohon, Reference Spoor, Stice, Burton and Bohon2007). Reducing the health burden of bulimia on adolescent girls is therefore crucial, and warrants concerted attempts at clarifying risk factors and processes that contribute to symptom presentation.
Investigations into the etiology of bulimia have generally taken two directions. One approach has considered whether nonbulimic and bulimic individuals differ on specified risk variables by degree or kind (Gleaves, Brown, & Warren, Reference Gleaves, Brown and Warren2004). Findings from this literature are mixed, but broadly fit the structure of a two-component model that predicts membership in groups with varying levels of disordered eating severity (Garner, Olmsted, & Polivy, Reference Garner, Olmsted and Polivy1983). In short, symptomatic youth seem to both (a) overprize the importance of weight and shape (e.g., strong endorsement of the thin ideal, high drive for thinness) and (b) exhibit ego deficits (e.g., poor interoceptive awareness, pervading sense of ineffectiveness) to a significantly greater degree than those who are asymptomatic (Lowe et al., Reference Lowe, Gleaves, DiSimone-Weiss, Furgueson, Gayda, Kolsky and McKinney1996; Mintz & Betz, Reference Mintz and Betz1988). Importantly, this research has furthered our understanding of when bulimic symptoms may arise.
The other common approach has considered processes through which risk factors work together to foster bulimia. Although numerous multivariate etiologic models have been proposed, most remain untested, unreplicated, or confined to cross-sectional analysis, with two notable exceptions (i.e., Stice, Reference Stice1994, Reference Stice2001; Thompson, Heinberg, Altabe, & Tantleff-Dunn, Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999). Namely, Stice's dual-pathway model suggests that perceived sociocultural pressure to be thin and thin-ideal internalization lead to body dissatisfaction. Resultant elevated levels of body dissatisfaction then lead to negative affect and dieting, each of which, in turn, predicts bulimic behavior. A second influential account is Thompson and colleagues’ tripartite-influence model, which posits that parental, peer, and media pressures to be thin intensify social comparison and thin-ideal internalization, leading to greater body dissatisfaction. Body dissatisfaction, in turn, promotes dieting, which later gives rise to bulimia. Importantly, this research has furthered our understanding of how bulimic symptoms may arise.
Despite the unique contributions of the two-component model and the dual-pathway and tripartite-influence models, they share key limitations that merit further attention. First, rather than continuing to examine questions of when or how, there may be much theoretical and applied value to integrating what we know about when with what we know about how as a means to address the when of the how. Indeed, because the two-component model has differentiated symptomatic from asymptomatic youth (Lowe et al., Reference Lowe, Gleaves, DiSimone-Weiss, Furgueson, Gayda, Kolsky and McKinney1996; Mintz & Betz, Reference Mintz and Betz1988), and the dual-pathway and tripartite-influence models both culminate in bulimic symptoms, it is possible that the mediational paths comprising process models are somehow contingent on the degree to which adolescent girls both overvalue thinness and show ego deficits.
Another limitation of current etiologic models is their uniform application to early-, mid-, and late-adolescent girls—not because age differences in patterns of risk for bulimia do not exist, but because they remain largely unassessed. The eating disorders literature is saturated with studies focused on one age group or aggregated data from multiple age groups. In fact, we know of just two investigations of age-related variation in the salience of risk factors for eating disturbances (i.e., Gralen, Levine, Smolak, & Murnen, Reference Gralen, Levine, Smolak and Murnen1990; Wertheim, Koerner, & Paxton, Reference Wertheim, Koerner and Paxton2001). Both studies involved samples of early- and mid-adolescent girls, but not late-adolescent girls, and neither study made inferential comparisons (e.g., moderation, multiple-group analysis) between the substages—that is, “differences” were interpreted by visually inspecting separate regression-based models for each age group. Efforts to test etiologic models with greater sensitivity to developmental context and statistical rigor would shed new light on girls’ risk within the diverse physical, cognitive, and socioemotional terrain of early to late adolescence.
The present study addresses these gaps through a developmental psychopathology lens, which promulgates the multiplicity of paths between risk factors and outcomes (i.e., equifinality and multifinality; Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996) in addition to chronological age, developmental stage, and the like as defining features of context for human adaptation and maladaptation (Cicchetti & Aber, Reference Cicchetti and Aber1998). Specifically, we explore whether the restraint pathway—that is, the mediational chain from body dissatisfaction to bulimia through dieting, common to both the dual-pathway and tripartite-influence models—varies as a function of thin-ideal internalization (i.e., “component one”) and interoceptive deficits (i.e., “component two”) for three different age groups of adolescent girls (i.e., middle school, high school, and college).
Why reexamine the restraint pathway as a conditional process?
It is noteworthy that explanations of how bulimia develops include some mention of the restraint pathway. In theory, body dissatisfaction leads to dieting due to the pervasive belief that dieting is an effective strategy for achieving a thinner, more desirable physique (Fairburn & Garner, Reference Fairburn, Garner, Garner and Garfinkel1988). To produce weight loss, however, dieting must yield a negative energy balance—an altered metabolic state that, when regularly met, precipitates physiological and psychological vulnerabilities to bulimic eating patterns (Polivy & Herman, Reference Polivy and Herman1985). Dieters may binge due to the effects of caloric deprivation (e.g., tryptophan depletion) or lapses in cognitive control over food intake (e.g., “I already blew my diet by eating a cookie, so I might as well eat a dozen”), then may purge, fast, and/or exercise compulsively to prevent weight gain, assuage guilt, and reorient to strict dietary rules (Fairburn, Reference Fairburn, Clark and Fairburn1997).
Research generally supports these theoretical claims. Longitudinal studies, for example, suggest that higher levels of body dissatisfaction predict future increases in dieting (Stice & Shaw, Reference Stice and Shaw2003) and that elevations in dieting predict the onset of and future increases in bulimia (Field, Camargo, Taylor, Berkey, & Coldiz, Reference Field, Camargo, Taylor, Berkey and Colditz1999). Although body dissatisfaction may also predict bulimic-symptom onset and exacerbation (Cooley & Toray, Reference Cooley and Toray2001), dieting is broadly accepted as a more proximal predictor (Polivy & Herman, Reference Polivy and Herman1985) given evidence that binging episodes tend to be preceded by periods of caloric restriction as compared to normal eating (Pyle, Mitchell, & Eckert, Reference Pyle, Mitchell and Eckert1981) and that a majority of bulimic patients report that their symptoms first appeared while dieting (Bulik, Sullivan, Carter, & Joyce, Reference Bulik, Sullivan, Carter and Joyce1997). Moreover, in direct support of the restraint pathway, Stice (Reference Stice2001) found that the link between adolescent girls’ body dissatisfaction and subsequent growth in bulimic behavior became nonsignificant after dieting was entered as an intermediary variable. Many studies have corroborated these mediational findings (e.g., Allen, Byrne, & McLean, Reference Allen, Byrne and McLean2012; Blodgett Salafia & Gondoli, Reference Blodgett Salafia and Gondoli2010), contributing, overall, to a rich empirical base highlighting body dissatisfaction and dieting as important, and plausibly interlinked, precursors to bulimia (Stice, Reference Stice2002).
Notwithstanding the above, the restraint pathway suffers a problematic shortcoming that has not yet been investigated. Prevalence data have long indicated that among adolescent girls, bulimic pathology is relatively rare, but body dissatisfaction and dieting are so common as to be considered “a normative discontent” (Rodin, Silberstein, & Striegel-Moore, Reference Rodin, Silberstein and Striegel-Moore1984, p. 267) and “normal eating” (Polivy & Herman, Reference Polivy and Herman1987, p. 635), respectively. Why do so few adolescent girls exhibit symptomatology if body dissatisfaction and dieting are so rife and are implicated in a causal process resulting in bulimia? It may not be the case that symptomatic individuals are simply more dissatisfied with their bodies and restrictive of their eating than are asymptomatic others, as some studies have shown that bulimic-like individuals are virtually indistinguishable from mere dieters based on these factors (Mintz & Betz, Reference Mintz and Betz1988; Ruderman & Besbeas, Reference Ruderman and Besbeas1992). Consequently, what separates the subset of adolescent girls who cross the line into pathology from those who experience comparably high levels of body dissatisfaction and dieting, yet remain symptom-free?
It is not sensible to continue purporting the validity of the restraint pathway at the omission of this question. A more integrative approach involves reframing the restraint pathway as a conditional process. Doing so preserves the longstanding body dissatisfaction → dieting → bulimia view while acknowledging that this path must have boundary conditions that determine whether the mediating effect is strong versus weak or present versus absent. Accordingly, we explore how certain individual-difference factors (i.e., thin-ideal internalization, interoceptive deficits, and age) might modify adolescent girls’ responses to elevated body dissatisfaction and dieting, conferring increased risk for or protection from bulimic-symptom expression. Given the complexity of our hypothesized model (see Figure 1), moderators are individually discussed as the link that they are expected to alter is presented.

Figure 1. Hypothesized first- and second-stage moderated mediation model wherein the indirect effect of body dissatisfaction on bulimic symptoms through dieting is conditional on thin-ideal internalization, interoceptive deficits, and age, while controlling for BMI (i.e., body mass index) and depressive symptoms.
Thin-ideal internalization as a moderator of the body dissatisfaction–dieting link
Although body dissatisfaction is the strongest known predictor of dieting among adolescent girls (Mendes, Araújo, Lopes, & Ramos, Reference Mendes, Araújo, Lopes and Ramos2014), researchers should take care not to oversimplify this relation. Both body dissatisfaction and dieting are multifaceted constructs—the former comprising a range of cognitions, emotions, and self-perceptions regarding one's physical appearance (Cash & Pruzinsky, Reference Cash and Pruzinsky1990), and the latter comprising a range of health-promoting and health-compromising behaviors intended to change or maintain one's physical appearance via weight control (Hill, Reference Hill, Fairburn and Brownell2002). It is high-frequency dieting, rather than dieting per se, that is a prominent mechanism underlying adolescent girls’ eating disorder risk (Kenardy, Brown, & Vogt, Reference Kenardy, Brown and Vogt2001), and body dissatisfaction may not universally foster restriction to such a harmful degree. Of interest, then, is whether the prediction of high-frequency dieting can be refined by concomitantly examining other variables that may exacerbate the deleterious effects of body dissatisfaction.
To this end, we consider the moderating role of thin-ideal internalization. This construct captures the extent to which an individual endorses Western culture's feminine beauty norms, which emphatically prescribe an ultrathin figure (that is physiologically impossible for most to attain) as requisite for attractiveness, status, happiness, and overall success (Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999). In line with dissonance theory (Festinger, Reference Festinger1957)—which states that when individuals harbor psychologically inconsistent cognitions, they feel uncomfortable and are driven to make changes that they believe will restore consistency—it seems that thin-ideal internalization could interact with body dissatisfaction to promote the level of dietary restraint that is most strongly associated with bulimia. The combination of subscribing to the thin ideal and being dissatisfied with one's body is more dissonant than any other combination of the two variables, as it implies a perceived discrepancy between one's coveted body and one's actual body that rigid diets are touted to fix. Because body-dissatisfied internalizers are presumably more susceptible to weight-loss propaganda than body-dissatisfied noninternalizers, and are presumably more likely than body-satisfied internalizers to desire changing their bodies to approximate the ideal, we propose that body-dissatisfied internalizers’ eating habits are significantly more restrictive.
No research, to date, has explicitly tested the moderating effect of thin-ideal internalization on the relation of body dissatisfaction to dieting, but some suggestive findings exist. Studies involving nonclinical samples of early-, mid-, or late-adolescent girls, who are categorized into risk groups and subsequently compared on other risk variables, seem telling. For instance, Hill and associates (Reference Hill, Oliver and Rogers1992) found that middle school girls classified as highly restrained expressed greater body dissatisfaction and endorsed a significantly slimmer ideal body type than other same-age dieters. Additionally, data obtained from high school girls suggests that relative to dieters who use exclusively moderate weight-control methods (e.g., eating a balanced diet inclusive of food groups, eating less sugar and fats), highly restrictive dieters were more dissatisfied with their bodies and fixated on pursuing the thin ideal (Neumark-Sztainer, Butler, & Palti, Reference Neumark-Sztainer, Butler and Palti1995). In a similar vein, college girls whose dieting motivation was strongly cosmetic, versus health-based, reported higher levels of body dissatisfaction and restrained eating (Putterman & Linden, Reference Putterman and Linden2004). Further indirect support for this hypothesized interaction can be gleaned from extensive cross-sectional, longitudinal, and experimental studies that identify thin-ideal internalization as an important correlate and predictor of dieting, as well as a causal risk factor for bulimic symptoms (Thompson & Stice, Reference Thompson and Stice2001).
Interoceptive deficits as a moderator of the dieting–bulimia link
It is unlikely that high-frequency dieting will, on its own, sufficiently explain which adolescent girls are prone to bulimic episodes. Indeed, despite their 18-fold increased risk for developing pathological eating patterns (Patton, Selzer, Coffey, Carlin, & Wolfe, Reference Patton, Selzer, Coffey, Carlin and Wolfe1999), only a minority of highly-restrictive dieters actually do. A population-based study indicated, for example, that of 2,992 mid- to late-adolescent girls who initially reported high dietary restraint, less than 3.5% developed an eating disorder within the next two years (Fairburn, Cooper, Doll, & Davies, Reference Fairburn, Cooper, Doll and Davies2014). Such findings suggest that individual-difference factors may determine which high-frequency dieters succumb to the physiological and cognitive disinhibitors that putatively trigger the binge-purge cycle.
On that account, we consider whether variability in interoceptive awareness influences the strength of the relation between dieting and bulimia. The accurate identification of internal stimuli that indicate hunger, satiety, and specific emotions is a cornerstone of competent self-regulatory functioning, as it facilitates one's capacity to choose and execute an appropriate behavioral response (Cannon, Reference Cannon1932; Farb et al., Reference Farb, Daubenmier, Price, Gard, Kerr, Dunn and Mehling2015; Kleckner et al., Reference Kleckner, Zhang, Toroutoglou, Chanes, Xia, Simmons and Barrett2017). Those who are deficient in this essential skill have a primitive experience of internal states, such that appetite cues and emotions, alike, are perceived as a vague sense of distress or contentment (Bruch, Reference Bruch1973). Consequently, these individuals rely on external cues and sources for self-regulation, which are often arbitrary or based on short-term consequences and are thus ineffective (Saarni, Reference Saarni1999). In the context of high dietary restraint, such deficits may be particularly troublesome, as a great deal of self-regulation is needed to overcome cravings, mood changes, and social pressures to indulge (Herman & Polivy, Reference Herman, Polivy, Baumeister and Vohs2004). The uncomfortable emotions evoked by these challenges are theoretically met with adaptive coping strategies by dieters who are attuned to their interoceptive signals. In contrast, those with interoceptive deficits may seek to escape their ambiguous discomfort by feeding it, then have difficulty stopping (given their blunted ability to detect satiety), and purge and/or intensify dieting efforts to curb current or avoid future over-fullness and guilt (Schmidt & Treasure, Reference Schmidt and Treasure2006).
Although there are no known tests of interoceptive deficits as a moderator of dieting on bulimic symptoms, several studies offer indirect support for this interaction. Most notably, relative to asymptomatic dieters (Lowe et al., Reference Lowe, Gleaves, DiSimone-Weiss, Furgueson, Gayda, Kolsky and McKinney1996) and late-adolescent girls with no history of mental health problems (Fassino, Piero, Gramaglia, & Abbate-Daga, Reference Fassino, Piero, Gramaglia and Abbate-Daga2004), bulimic individuals reported significantly poorer interoceptive awareness. Furthermore, in large community samples of middle- and high school girls, interoceptive deficits predicted onset of bulimia over one-year (Leon, Fulkerson, Perry, & Early-Zald, Reference Leon, Fulkerson, Perry and Early-Zald1995) and four-year intervals (Killen et al., Reference Killen, Taylor, Hayward, Haydel, Wilson, Hammer and Strachowski1996). Owing to their diminished capacity to interpret hunger and fullness, more specifically, bulimic patients reported inconsistent levels of satiety in response to a fixed amount of food that they consumed in the laboratory over several discrete occasions, and reported greater levels of hunger post-meal than controls (Hadigan, Walsh, Devlin, LaChaussée, & Kissileff, Reference Hadigan, Walsh, Devlin, LaChaussée and Kissileff1992). Also, an experimental study by Sim and Zeman (Reference Sim and Zeman2004) demonstrated bulimic patients’ nebulous experience of emotional states. When asked to recall a situation that elicited high or low levels of negative emotion, symptomatic high school girls took significantly longer to label their emotions and were more likely to use nonspecific descriptors (e.g., “upset”) than girls in the community control group, regardless of condition. Taken together, then, interoceptive deficits may be one factor that bridges the gap between high-frequency dieting and bulimia.
Is the harmful effect of a dieting by interoceptive deficits interaction magnified in late adolescence?
From a more speculative standpoint, it is interesting to consider whether high dietary restraint and interoceptive deficits could differentially affect girls in early, middle, and late adolescence (about ages 10–13, 14–17, and 18–25, respectively). Whereas each substage presents unique events and changes that may increase girls’ vulnerability to eating problems (Shisslak, Crago, Estes, & Gray, Reference Shisslak, Crago, Estes, Gray, Smolak, Levine and Striegel-Moore1996), it is worth noting that bulimic-symptom onset most commonly occurs during late adolescence (Stice, Marti, Shaw, & Jaconis, Reference Stice, Marti, Shaw and Jaconis2009). This suggests that adaptation to the developmental demands of this substage takes the form of disordered eating more often than in early or middle adolescence (Woodside & Garfinkel, Reference Woodside and Garfinkel1992).
What is it about late adolescence, particularly, that may amplify the detrimental effects of engaging in high-frequency dieting and having an impaired ability to discriminate physiological and emotional states? First, although increasingly mature behavior is expected as girls traverse early to middle adolescence, also expected is the daily instrumental, emotional, and informational support of the family. The late-adolescent transition typically involves heightened separation-individuation from parents, experienced most often as moving from the home into a more independent living situation, managing one's own social calendar and school/work responsibilities, and establishing a lifestyle and identity reflective of one's goals and values (Waterman, Reference Waterman1982). This sharp surge toward autonomy does not happen during early or middle adolescence, and tests the adequacy of late-adolescent girls’ coping skills.
Furthermore, some features of college life may exacerbate developmental stressors and support the likelihood of maladaptive outcomes, including bulimic pathology. Academic pressures, standards of attractiveness, and dating/sexual pressures are often intensified by the college environment at the same time that having left home results in at least a brief reduction in social support (Striegel-Moore, Reference Striegel-Moore, Fairburn and Wilson1993). For girls who manage these challenges via weight control, the buffet-style, readily-available food surplus in dining halls coupled with the difficulty of storing fresh, healthy food in dorm rooms may perpetually test dietary vigilance and promote overeating (Nelson, Kocos, Lytle, & Perry, Reference Nelson, Kocos, Lytle and Perry2009). Overall, it seems that late adolescence is a less accommodating context for high-frequency dieting and interoceptive deficits than previous substages, and that this effect could be evidenced in greater levels of bulimia in college girls.
Current study
If the restraint pathway is etiologically relevant to bulimia, as decades of theory and research suggest, then there must be specific conditions under which the mediating effect does and does not occur, given decades of discordance between the prevalence of bulimia relative to its proposed antecedents. Driven by this view, we examined whether variables that have previously distinguished symptomatic from asymptomatic youth (i.e., thin-ideal internalization and interoceptive deficits) also distinguish when body dissatisfaction and dieting are linked, in a meditational sequence, with bulimic symptoms among girls in different developmental contexts (i.e., middle school, high school, and college). More specifically, we tested a conditional process model in which body dissatisfaction interacts with thin-ideal internalization to predict high-frequency dieting, which, in turn, interacts with interoceptive deficits and age to predict bulimia. In light of evidence indicating that body mass index (BMI) and depressive symptoms may promote eating pathology (Stice, Reference Stice2002), we controlled for these factors in all primary analyses.
We hypothesized that:
1. thin-ideal internalization moderates the positive link between body dissatisfaction and dieting, such that body-dissatisfied girls who report high, versus low, endorsement of sociocultural standards for thinness engage in significantly greater dietary restraint;
2a. interoceptive deficits moderates the positive link between dieting and bulimia such that only dieters who struggle to perceive internal body cues express bulimic symptoms, but
2b. this interaction is significantly stronger for college girls than for middle- and high school girls; and
3a. the indirect effect of body dissatisfaction on bulimia through dieting is exclusive to those who report high thin-ideal internalization and high interoceptive deficits, but
3b. this effect is significantly stronger for college girls than for middle- and high school girls.
Method
Participants
Data were drawn from a larger study focused on mother and daughter eating- and weight-related attitudes and behaviors across three age cohorts of daughters (i.e., middle school, high school, and college). Participants were recruited from area schools and a private university in a medium-sized, Midwestern US city. To recruit middle- and high school girls, letters were mailed by schools to all mothers of girls in 7th, 8th, 10th, and 11th grades. College girls were recruited through psychology courses. College girls and mothers of middle- and high school girls were instructed to contact the research office should they like to participate.
Of the 391 who initially agreed to participate, 353 (90.28%) mother–daughter pairs completed the study. Twenty-four (6.14%) of those who dropped did not attempt to complete any aspect of the study and were unresponsive to repeated contact efforts. Six dyads (1.53%) shared that they were no longer interested in participating, and eight others (2.05%) fell out of contact for unknown reasons after partially completing the study.
The current major analyses focus on daughter self-reports. Mothers provided household demographic data, which are summarized below. The daughter sample consisted of 353 adolescent girls (n MIDDLE SCHOOL = 115, n HIGH SCHOOL = 112, n COLLEGE = 126) who were between the ages of 11 and 22 years, M age = 16.14, SD age = 2.93. The middle school participants were 72 7th graders and 43 8th graders (M age = 12.77, SD age = 0.78), and the high school cohort was comprised of 69 10th graders and 43 11th graders (M age = 15.95, SD age = 0.79). Although nearly half of participating college girls were freshmen (n = 59), 25 sophomores, 20 juniors, and 22 seniors also participated (M age = 19.39, SD age = 1.37).
Most girls were European American (77.05%). Fewer identified as African American (3.68%), Asian American (2.83%), Hispanic/Latina (2.55%), Native American (0.85%), multiethnic (11.05%), or other (1.42%). Participants were generally from two-parent, well-educated families, as a majority of mothers were married (81.02%) and had completed at least a two-year college degree (78.80%). The sample was less homogenous economically, with annual household incomes ranging from $13,000 to $900,000 (Mdn = $90,000, M = $117,932, SD = $107,799). In terms of weight status, the mean body mass index (BMI) z-score of the sample was 22.24 (SD = 4.46, range: 13.90–47.20). According to established BMI-for-age cut-points (Kuczmarski et al., Reference Kuczmarski, Ogden, Guo, Grummer-Strawn, Flegal, Mei and Johnson2000; Ogden et al., Reference Ogden, Kuczmarski, Flegal, Mei, Guo, Wei and Johnson2002), most participants were of normal weight (75.92%), whereas approximately one fifth were overweight (14.73%) or obese (7.08%), and a small percentage were underweight (2.27%). Overall, the sample was demographically typical of the community and university student populations from which it was derived.
Procedure
Online questionnaires were configured using the Qualtrics secure survey software program (Qualtrics, Provo, UT). Each web-based packet consisted of informed consent or assent forms, parental consent forms (as applicable to mothers of minors), and a set of self-report measures that took roughly one hour to complete. Middle- and high school girls were emailed a link and instructed to independently complete their online packet in one sitting, whereas college girls visited an on-campus psychology laboratory to access and complete theirs. Following this step, female doctoral-level research assistants conducted private in-school or on-campus appointments to obtain daughters’ height and weight measurements for the calculation of BMI.
Participants were each compensated $10.00 for their involvement in the study. In some cases, college girls opted to receive course credit in lieu of payment. All aspects of this research were approved by the university's Institutional Review Board (IRB) prior to implementation.
Measures
Body dissatisfaction
An abbreviated version of the 25-item Satisfaction and Dissatisfaction with Body Parts Scale (Berscheid, Walster, & Bohrnstedt, Reference Berscheid, Walster and Bohrnstedt1973; Stice & Shaw, Reference Stice and Shaw1994) was used to assess body dissatisfaction. Respondents rate the extent to which they are satisfied with eight commonly critiqued size- or shape-related dimensions of the female body (e.g., thighs, stomach) on a 6-point Likert-type scale ranging from 1 (extremely satisfied) to 6 (extremely dissatisfied). Higher scores indicate greater body dissatisfaction. Within the current sample, Cronbach's alpha was .93.
Dieting
The 10-item Dutch Restrained Eating Scale (DRES; van Strien, Frijters, Bergers, & Defares, Reference van Strien, Frijters, Bergers and Defares1986) was used to assess intention to diet and frequency of caloric restriction for weight-control purposes. Respondents indicate how often dieting cognitions and behaviors dictated their eating patterns within the past week on a 5-point Likert-type scale that ranges from 1 (never) to 5 (always). A sample item includes, “How often did you deliberately eat less in order to not become heavier?” Higher scores indicate greater levels of dieting. In the present study, Cronbach's alpha was .95.
Thin-ideal internalization
Internalization of the thin ideal was measured using the 9-item Internalization–General subscale of the Sociocultural Attitudes Towards Appearance Questionnaire–3 (SATAQ–3–IG; Thompson, van den Berg, Roehrig, Guarda, & Heinberg, Reference Thompson, van den Berg, Roehrig, Guarda and Heinberg2004). Respondents indicate their endorsement of media-promoted female body standards (e.g., “I would like my body to look like the models who appear in magazines”) on a 5-point Likert-type scale ranging from 1 (definitely disagree) to 5 (definitely agree). Higher scores indicate greater levels of thin-ideal internalization. Cronbach's alpha was .93 in the present sample.
Interoceptive deficits
The 10-item Interoceptive Awareness subscale of the Eating Disorder Inventory (EDI-IA; Garner et al., Reference Garner, Olmsted and Polivy1983) was used to assess interoceptive deficits. Respondents indicate the degree to which they have difficulty recognizing hunger and satiety cues (e.g., “I get confused as to whether or not I am hungry”) and emotional states (e.g., “When I am upset, I don't know if I am sad, frightened, or angry”) on a 6-point Likert-type scale ranging from 0 (never) to 5 (always), with higher scores indicating greater interoceptive deficits. In contrast to manual instructions (Garner & Olmsted, Reference Garner and Olmsted1984), we did not weight responses from 0 to 3 prior to summing, as research has shown that the 0–5 item scoring system is more appropriate for nonclinical populations (Schoemaker, van Strien, van der Staak, Reference Schoemaker, van Strien and van der Staak1994). In the current study, Cronbach's alpha was .88.
Age
Participants reported their current age, in years, on a general demographics form.
Bulimic symptoms
The 7-item Bulimia subscale of the EDI (EDI-B; Garner et al., Reference Garner, Olmsted and Polivy1983) was used to assess inclinations toward uncontrollable binging and self-induced purging. Example items include, “I have gone on eating binges where I felt that I could not stop” and “I have thought of trying to vomit in order to lose weight.” Respondents indicate the frequency with which they engage in the specified behaviors on a 6-point Likert-type scale ranging from 0 (never) to 5 (always). As previously noted for the EDI-IA, we chose to retain the untransformed (i.e., 0–5) item scoring system. Higher scores indicate greater levels of bulimic symptomatology. Cronbach's alpha was .86 in the present study.
BMI
Participants’ sex, birthdate, weight, and height were entered into the Mayo Clinic's Online Child BMI Calculator (www.mayoclinic.com). To compute BMI z-scores, this tool multiplies weight [lbs.] by 703/height [in.2] while controlling for variations in measurements due to sex and age.
Depressive symptoms
The Children's Depression Inventory (CDI; Kovacs, Reference Kovacs1992) was used to assess depressive symptoms for the middle- and high school cohorts. For each item, respondents select one of three choices that best describes them, listed in order of increasing severity: 0 (no symptom), 1 (mild symptom), or 2 (definite symptom). A sample item includes, “I feel like crying once in awhile,” “I feel like crying many days,” and “I feel like crying everyday.” Higher scores indicate greater depressive symptoms. Per the request of the university's IRB, the item that assesses suicidal thoughts was omitted; thus, the original 27-item CDI was reduced to 26 for the current study. Cronbach's alpha was .89.
For the college cohort, depressive symptoms were assessed using the 21-item Beck Depression Inventory-II (BDI-II; Beck, Steer, & Brown, Reference Beck, Steer and Brown1996). Each item is a group of four statements, rated 0 to 3 from least to most symptomatic, and respondents select the statement that best describes how they have been feeling during the past two weeks. A sample item includes, “I do not feel sad,” “I feel sad much of the time,” “I am sad all the time,” and “I am so sad or unhappy I can't stand it.” Higher scores indicate greater depressive symptoms. As requested by the university's IRB, the item assessing suicidal thoughts was omitted. The resulting 20-item scale yielded a Cronbach's alpha of .82 in the present sample.
To form a single composite variable, total scores on the CDI were translated to the scale of the BDI-II via the linear equating method (Livingston, Reference Livingston2004). Linear equating is conceptually identical to standardization, and both approaches produce the same rank ordering; however, results are expressed in a meaningful unit rather than a scale-free, standardized unit.
Results
All analyses were performed using IBM SPSS Statistics version 22 software. Prior to substantive analysis, we screened the data (i.e., missing values, ordinary least squares assumptions, outliers) and examined descriptive statistics (i.e., means, standard deviations) for and bivariate correlations among all study variables.
Following the guidelines for testing conditional process models outlined by Hayes (Reference Hayes2013, pp. 393–397), study hypotheses were addressed in two broad, interlinked steps. First, two hierarchical multiple linear regression models were specified, with dieting and bulimic symptoms as the dependent variables. Next, we assessed the presence of moderation, mediation, and moderated mediation using the PROCESS macro for SPSS (Hayes, Reference Hayes2013; available at www.afhayes.com). Specifically, (a) significant interactions (i.e., Hypotheses 1, 2a, and 2b) were probed by calculating and plotting simple slopes at selected values of the moderators (Aiken & West, Reference Aiken and West1991), (b) a test of the unmoderated indirect effect of body dissatisfaction on bulimic symptoms through dieting was performed using bootstrap procedures recommended by Preacher and Hayes (Reference Preacher and Hayes2004), and (c) moderated mediation (i.e., Hypotheses 3a and 3b) was assessed by constructing 95% bias-corrected bootstrap confidence intervals for the indirect effect at selected values of the moderators (Preacher, Rucker, & Hayes, Reference Preacher, Rucker and Hayes2007).
Data screening
Missing data accounted for .0019% of collected records, appeared sporadic, and were imputed using the mean of the participant's nonmissing responses to the remainder of the scale or subscale if only one item was missing, which was unanimously the case. Data for the full sample of 353 adolescent girls were therefore available for analysis.
We ensured that the errors in estimation did not violate the ordinary least squares assumptions of independence, homoscedasticity, and normality by means of both visual inspection and statistical tests. Based on scatterplots in which the residuals of each variable were plotted against their corresponding predicted values, the assumptions appeared tenable. We reached the same conclusion using more objective methods, including the Durbin-Watson test (to assess independence; Durbin & Watson, Reference Durbin and Watson1951), regressing raw residuals on both sets of predictor variables (to assess homoscedasticity; Darlington, Reference Darlington1990), and examining absolute values of skewness and kurtosis for all study variables (to assess normality; Kline, Reference Kline1998).
To screen for outliers, we examined standardized DFFITS and DFBETA values for each model using ±1.00 as a cutoff (Cohen, Cohen, West, & Aiken, Reference Cohen, Cohen, West and Aiken2003). Although all DFBETA values fell within an acceptable range, regression diagnostics revealed three cases with standardized DFFITS > 1.00 for the model predicting bulimic symptoms. Whether these cases were left as is, retained with a natural log transformation applied to bulimia (which pulled the initially problematic standardized DFFITS values below 1.00), or removed from the data set, the same pattern of findings emerged. Therefore, to aid interpretation, all analyses were conducted using untransformed data for the full sample.
Descriptive statistics and bivariate correlations
Means, standard deviations, and intercorrelations among study variables are shown in Table 1. Correlations were statistically significant, positive, and small to moderate in magnitude, aside from the nonsignificant age–interoceptive deficits and age–depressive symptoms associations as well as five bivariate associations that were substantial (i.e., r ≥ .50; Cohen, Reference Cohen1988). Regarding the latter observation, we note that other studies involving nonclinical samples of adolescent girls have reported similarly strong contemporaneous correlations between the same measures of body dissatisfaction and dieting (Stice, Mazotti, Krebs, & Martin, Reference Stice, Mazotti, Krebs and Martin1998), body dissatisfaction and thin-ideal internalization (Utschig, Presnell, Madeley, & Smits, Reference Utschig, Presnell, Madeley and Smits2010), dieting and thin-ideal internalization (Homan, Reference Homan2010), interoceptive deficits and bulimia (Anestis, Selby, Fink, & Joiner, Reference Anestis, Selby, Fink and Joiner2007), and interoceptive deficits and depressive symptoms (Ouwens, van Strien, van Leeuwe, & van der Staak, Reference Ouwens, van Strien, van Leeuwe and van der Staak2009). Nevertheless, these constructs are upheld in the literature as separate, yet related, and we found that multicollinearity between independent variables was not a problem in either regression model (i.e., condition indices < 15, variance inflation factors < 10, tolerance values > .10; Ho, Reference Ho2006, p. 267). In sum, observed correlations were in accord with previous research and provided initial support for the hypothesized relations.
Table 1. Means, standard deviations, and intercorrelations among study variables, N = 353

Note: ***p < .001.
Hierarchical multiple linear regressions and simple slopes tests
Dieting
The first of two hierarchical regression analyses was conducted using dieting as the dependent variable (see Table 2). At initial entry, all independent variables significantly increased the proportion of variance accounted for in the model. Control variables (i.e., BMI and depressive symptoms) did not uniquely contribute to variation in dieting beyond Step 1, but body dissatisfaction (entered at Step 2) and thin-ideal internalization (entered at Step 3) remained significant positive predictors through the final step of the analysis. More critically, we detected a significant Body dissatisfaction x Thin-ideal internalization interaction.
Table 2. Hierarchical regression analysis predicting dieting, N = 353

Note: First-order terms were mean-centered for analysis, and interaction terms were computed as the product of mean-centered predictor and moderator variables. Effect size was estimated by Cohen's f 2 (Cohen, Reference Cohen1988) and considered small (<.15), medium (.15 to .34), or large (≥.35). *p < .05 ***p < .001.
To probe the nature of the observed interaction, simple slopes for the regression of dieting on body dissatisfaction were evaluated for significance at low (i.e., −1 SD from the mean) and high (i.e., +1 SD from the mean) levels of thin-ideal internalization. Both of the regression lines were statistically different from zero, suggesting that the positive association between body dissatisfaction and dieting is relevant to low internalizers [t (347) = 4.48, p < .001] and high internalizers [t (347) = 6.83, p < .001]. Still, as expected, body-dissatisfied girls who reported a high, versus low, endorsement of the thin ideal engaged in a significantly greater level of dietary restraint [t (347) = 2.54, p < .05].
Bulimic symptoms
The second regression model is presented in Table 3. Excluding the Dieting x Interoceptive deficits and Interoceptive deficits x Age interactions (which were nonsignificant when added at Step 4), the variables added to the model at each step explained a significant amount of unique variance in bulimia. Depressive symptoms remained positively related to the outcome until Step 3, when interoceptive deficits and age were entered. In the final step, BMI, body dissatisfaction, dieting, and interoceptive deficits still emerged as significant predictors of greater bulimic symptoms, but age became nonsignificant in the presence of two significant higher-order terms: the two-way interaction between dieting and age and the three-way interaction between dieting, interoceptive deficits, and age.
Table 3. Hierarchical regression analysis predicting bulimia, N = 353

Note: First-order terms were mean-centered for analysis, and interaction terms were computed as the product of mean-centered predictor and moderator variables. Effect size was estimated by Cohen's f 2 (Cohen, Reference Cohen1988) and considered small (<.15), medium (.15 to .34), or large (≥.35). *p < .05, **p < .01 ***p < .001.
To interpret the significant Dieting x Age interaction, simple slopes for the regression of bulimia on dieting were calculated at the mean age value for each subsample: 12.77 (middle school), 15.95 (high school), and 19.39 (college). The analysis revealed that dieting was a significant positive predictor of bulimic symptoms in college girls [t (342) = 3.42, p < .001], but not in middle school [t (342) = −.08, p > .05] or high school [t (342) = 1.87, p > .05] girls.
In light of the significant three-way interaction (see Figure 2), we further probed the Dieting x Age interaction at low (-1 SD from the mean) and high (+1 SD from the mean) values of interoceptive deficits. We found that high-frequency dieting was only associated with greater bulimic symptoms in college girls who reported high interoceptive deficits [t (342) = 3.47, p < .001]. At low levels of interoceptive deficits, regardless of whether middle school [t (342) = .83, p > .05], high school [t (342) = 1.56, p > .05], or college [t (342) = 1.50, p > .05] girls were considered, no relation between dieting and bulimia was observed. Although the same was true for middle school [t (342) = −1.41, p > .05] and high school [t (342) = 1.56, p > .05] girls who reported high interoceptive deficits, visual inspection of the plots suggests a positive main effect of interoceptive deficits on bulimic symptoms for these age groups.

Figure 2. Regression lines for relations between dieting and bulimic symptoms as moderated by interoceptive deficits and age (a significant three-way interaction). ***p < .001. B = unstandardized simple slope estimate, MS = middle school, HS = high school, COL = college.
Simple mediation analysis
A test of simple mediation was performed to determine whether the well-documented indirect effect of body dissatisfaction on bulimic symptoms through dieting could be replicated in the present data. Parameter estimates for paths a (i.e., body dissatisfaction → dieting) and b (i.e., dieting → bulimia) were obtained in Step 2 of both hierarchical regression models, and bias-corrected bootstrapping methods were employed to assess the significance of the specific indirect effect (ab). There is consensus among methodologists (e.g., Preacher & Hayes, Reference Preacher and Hayes2004) that this approach is more powerful and less stringent than traditional methods for evaluating mediation (e.g., Baron & Kenny, Reference Baron and Kenny1986). Accordingly, 5,000 bootstrap samples of size n = 353 were generated with replacement from the original sample, the indirect effect ab was computed for each sample, and all 5,000 point estimates of ab were sorted from low to high, around which a 95% confidence interval ranging from .03 to .13 was derived. Because the confidence interval did not include zero, the specific indirect effect was significant at p < .05.
Moderated mediation analysis
The analyses executed up to this point provide a piecemeal understanding of the interaction effects and specific indirect effect housed within the larger hypothesized moderated mediation model. To sufficiently address Hypotheses 3a and 3b, however, these effects must be integrated via conditional process analysis. Using methods directly analogous to those used to assess moderation, the conditional indirect effect (i.e., the product of paths a and b conditioned on values of the moderator variables) of body dissatisfaction on bulimic symptoms through dieting was examined at all possible combinations of low (−1 SD from the mean) and high (+1 SD from the mean) levels of thin-ideal internalization and interoceptive deficits for middle school (at M age = 12.77), high school (at M age = 15.95), and college (at M age = 19.39) girls. Bootstrap confidence intervals for the 12 resultant conditional indirect effect estimates were constructed in exactly the same way as previously described for simple mediation, were inferred as significant at p < .05 if they did not contain zero, and are shown in Table 4. As depicted, the indirect effect was exclusively observed in college girls who reported high interoceptive deficits, regardless of the degree to which they endorsed the thin ideal. A comparison of the difference between the two significant ab point estimates revealed, however, that the indirect effect for the college/high/high girls was stronger than for the college/low/high girls, 95% CI [.04, .07].
Table 4. Conditional indirect effects of body dissatisfaction on bulimia through dieting at levels of thin-ideal internalization, interoceptive deficits, and age
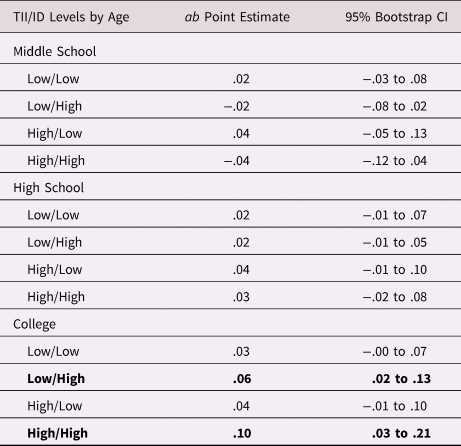
Note: Bootstrap confidence intervals were constructed using 5,000 resamples. “Low” and “high” refer to ±1 SD from the mean. Significant conditional indirect effects are depicted in bold. TII = thin-ideal internalization, ID = interoceptive deficits.
Discussion
Summary and interpretation of findings
Since the earliest writing on eating disorders (e.g., Bruch, Reference Bruch1973; Russell, Reference Russell1979), a pressing question has been, “Why some, but not others?” The purpose of this study was to explore that question in the context of the restraint pathway—a mediational process from body dissatisfaction through dieting to bulimia that is a fixture of two of the most prominent, widely studied etiological accounts of bulimic pathology (i.e., Stice, Reference Stice1994, Reference Stice2001; Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999), yet suffers conceptual limitations that, until now, have not been a focus of empirical attention. We approached the paradox of how the prevalence of body dissatisfaction and dieting in adolescent girls could be so high (e.g., > 60%; Neumark-Sztainer et al., Reference Neumark-Sztainer, Croll, Story, Hannan, French and Perry2002) relative to bulimic symptoms (e.g., < 18%; Neumark-Sztainer et al., Reference Neumark-Sztainer, Croll, Story, Hannan, French and Perry2002) if the restraint pathway is, in fact, valid, by reconceptualizing this process within a developmental psychopathology framework. As we subsequently discuss how the mediating effect varied as a function of thin-ideal internalization, interoceptive deficits, and age in our community sample of adolescent girls, recall that we were also able to replicate the restraint pathway in its unmoderated form. The juxtaposition of results is striking and suggests that an enhanced understanding of bulimic-symptom expression in adolescent girls may be achieved by integrating findings from the literature on quantitative versus qualitative differences, process-oriented models, and developmental theory.
Overall, we found that the restraint pathway applied only to college girls who reported high interoceptive deficits, irrespective of the degree to which they endorsed the thin ideal, but that this effect was significantly stronger for high, versus low, internalizers. For middle school and high school girls, regardless of their reported levels of thin-ideal internalization and interoceptive deficits, we found no evidence supporting the restraint pathway. In all analyses, BMI and depressive symptoms were controlled, indicating that the observed relations were just as likely to occur in adolescent girls who were of normal weight as in those who were underweight or overweight, whether depressed or not depressed. Although we anticipated finding age differences between college girls and the two younger cohorts in our moderated mediation model, we expected them to manifest as “stronger versus weaker”—not “significant versus nonsignificant.” These results are best interpreted in a path-by-path manner, as below.
Body dissatisfaction x Thin-ideal internalization to dieting
Turning first to the link between body dissatisfaction and dieting as moderated by thin-ideal internalization, we found evidence of a synergistic effect. Specifically, the co-occurrence of high body dissatisfaction and high thin-ideal internalization incurred a greater deleterious impact on dietary restraint than did high body dissatisfaction or high thin-ideal internalization, alone. Considered within our moderated mediation model, this effect persisted for college girls (who reported high interoceptive deficits), such that high internalizers expressed significantly greater levels of bulimic symptomatology than low internalizers. Although the same cannot be said for girls in middle school and high school, evidence of this interaction is still relevant from a “one-to-many” perspective (Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996). High-frequency dieting opens early- and mid-adolescent girls up to other risks besides bulimia (e.g., weight cycling, substance use; French, Story, Downes, Resnick, & Blum, Reference French, Story, Downes, Resnick and Blum1995), so refining the specificity of its prediction is beneficial to the broader adolescent health literature. Within the eating disorders literature, more particularly, our study was the first to test thin-ideal internalization as a moderator, rather than an antecedent, of body dissatisfaction. High body dissatisfaction, itself, was still positively associated with dieting (and bulimia, for college girls with high interoceptive deficits), but the risk posed by this variable was exponentially increased when combined with high thin-ideal internalization. This finding lends support to the theory that body-dissatisfied internalizers experience more dissonance (Festinger, Reference Festinger1957) than body-dissatisfied noninternalizers and body-satisfied internalizers, and they are thereby more restrictive of their eating to restore psychological consistency (i.e., dieting is the ticket to attaining the thin ideal and, consequently, body satisfaction). Future studies should continue to evaluate the collective influence of these variables for an improved understanding of their synergy and its impact.
Dieting x Interoceptive deficits x Age to bulimic symptoms
Next, we turn to the link between dieting and bulimia as moderated by interoceptive deficits and age. For college girls, we found evidence of a buffering effect, as high dietary restraint was not related to bulimic pathology for those who reported low interoceptive deficits. Importantly, this interaction was maintained in our moderated mediation model, and it dictated whether or not the mediating effect of body dissatisfaction on bulimia through dieting was significant. Even in the case of high body dissatisfaction, high thin-ideal internalization, and high-frequency dieting, college girls who reported an ability to perceive and interpret visceral sensations related to hunger, satiety, and emotions appeared protected from bulimic-symptom expression. This finding, in a novel way, corroborates prior research that has differentiated individuals at various stages of severity on the disordered eating continuum based on interoceptive functioning (e.g., asymptomatic dieters versus subclinical bulimics; Lowe et al., Reference Lowe, Gleaves, DiSimone-Weiss, Furgueson, Gayda, Kolsky and McKinney1996). It uniquely extends such work, as well, by situating the dieting by interoceptive deficits interaction within late adolescence. Disturbances in interoception, coupled with the normative challenges of emergent adulthood, may render college girls who are in the throes of restrictive eating likely to respond to virtually any arousal state with food intake, portending risk for the binge–purge cycle. Among college girls, then, bulimia may reflect a failed attempt to regulate internal body cues.
In contrast to our findings for college girls, we did not find an interaction between dieting and interoceptive deficits for middle school or high school girls. We note, though, that the positive main effect of interoceptive deficits on bulimia estimated for the full sample (β = .40***) was visually evident for both of the younger cohorts in the interaction plots. Considering high school girls, for example, the predicted values of bulimic symptoms as a function of low dieting and high dieting, respectively, were 3.65 and 5.26 for low interoceptive deficits and 8.92 and 10.09 for high interoceptive deficits. These values did not markedly change between low and high levels of dieting in either condition of interoceptive deficits, so the simple slopes were not significant. Nevertheless, the predicted values of bulimia are indeed higher when estimated for high, versus low, interoceptive deficits. A similar pattern was obtained for middle school girls. Thus, interoceptive deficits may still be relevant to explaining which early- and mid-adolescent girls are prone to bulimic episodes—perhaps just not as a moderator of dieting, or as part of the restraint pathway.
Our findings suggest that dieting is an especially salient predictor of bulimic symptoms among college girls. We found no evidence of a relation between dieting and bulimia for the two younger age groups, and note that much of the data supporting this link have been derived from mixed-age samples (e.g., Shepherd & Ricciardelli, Reference Shepherd and Ricciardelli1998; Stice, Reference Stice2001; Stice, Zimba, Margolis, & Flick, Reference Stice, Ziemba, Margolis and Flick1996). In the current study, when we grouped all ages together, we, too, found an association between dieting and bulimic symptoms. Relative to the few studies that have involved same-age middle- or high school samples, though, our null result is less surprising. For instance, in early-adolescent girls, a significant dieting–bulimia relation was observed by Blodgett Salafia and Gondoli (Reference Blodgett Salafia and Gondoli2010), but not by Wertheim and colleagues (Reference Wertheim, Koerner and Paxton2001). Likewise, in mid-adolescent girls, a significant dieting–bulimia relation was observed by Stice, Shaw, and Nemeroff (Reference Stice, Shaw and Nemeroff1998), but not by van Strien and colleagues (Reference van Strien, Engels, van Leeuwe and Snoek2005). Broadly, then, the association between dieting and bulimic behavior among younger adolescent girls seems to be more consistently supported in mixed-age, versus same-age, samples. Whether this is attributable to coincidence, a methodological issue (e.g., sampling error, imprecise measurement of constructs, not enough variance), or age differences in patterns of risk (that are masked by aggregated data) is unclear.
If age differences truly exist, it is interesting to think about why late-adolescent girls, compared with early- and mid-adolescent girls, might be more susceptible to the harmful effects of high-frequency dieting. A major challenge in delineating cross-sectional age differences is that they may at least partially reflect differences in length of exposure to experiential influences. That is, by virtue of being older, college girls may have longer dieting histories than middle- and high school girls, and this chronic restriction may be a more potent predictor of bulimia. Furthermore, relative to older adolescents, there is some evidence that eating behaviors among middle school girls are less entrenched (e.g., 7th graders; Wertheim et al., Reference Wertheim, Koerner and Paxton2001), suggesting that high dietary restraint, for some, may be a transitory experiment, and thus would not be expected to have an immediate or lasting detrimental effect. As regards dieting in high school versus college, context appears to be crucial. Research has shown, for example, that dietary restraint in girls does not significantly change over this transition (Vohs, Heatherton, & Herrin, Reference Vohs, Heatherton and Herrin2001), but that the college milieu may exacerbate its damaging effects and promote bulimic pathology (Striegel-Moore, Silberstein, & Rodin, Reference Striegel-Moore, Silberstein and Rodin1986). Together, these substantive considerations may help to explain why the dieting–bulimia link (and the restraint pathway, by extension) was applicable to college girls, but not middle- and high school girls in the current study.
Limitations and future directions
There are limitations to the present research that may provide direction for future studies. First, the data are both correlational, which precludes causal interpretation, and cross-sectional, which precluded the temporal ordering of body dissatisfaction, dieting, and bulimia. Mediational processes develop over time, and the abilities to control for prior assessments of the mediator and outcome and to test alternative directions of effects provide a better indication of the underlying causal mechanism than showing that the variables of interest may covary, as in cross-sectional research (Judd & Kenny, Reference Judd and Kenny1981). Additionally, patterns of change and continuity throughout development can only be assessed by collecting data from individuals on multiple occasions over time. Even if age groups do not differ in key sampling characteristics, comparing how risk variables interrelate among individuals of different ages cross-sectionally says nothing about the nature and course of developmental risk processes—only that the age groups may differ. Furthermore, with the exception of objective BMI measurements, we collected self-report data from a single source. Our results could therefore be strengthened through the future use of multiple methods and informants. We caution against overinterpreting our findings and advise that they be used as impetus for designing more methodologically rigorous replication studies.
Also, we acknowledge that the current sample is somewhat restricted with respect to race/ethnicity and socioeconomic status (SES). It is important not to readily generalize the results of this study to other racial/ethnic groups, as body dissatisfaction and eating disturbances are most prevalent in White, versus non-White, adolescent girls and women from Western countries (Wildes, Emery, & Simons, Reference Wildes, Emery and Simons2001). Moreover, although we sampled from a wide spectrum of income classes and there is no definitive association between SES and disordered eating (Gard & Freeman, Reference Gard and Freeman1996), the concentration of participants from upper-SES families in our sample was high. Future studies that include a more diverse range of racial/ethnic and socioeconomic groups will expand our knowledge base to a broader segment of the population.
Practical implications
The identification of thin-ideal internalization and interoceptive deficits as moderators of the restraint pathway has implications for the prevention and treatment of bulimia in adolescent girls, particularly during late adolescence. Among college girls, body dissatisfaction interacted with thin-ideal internalization to predict high-frequency dieting, which, in turn, interacted with interoceptive deficits to predict bulimic symptoms, indicating that altering levels of thin-ideal internalization or interoceptive deficits should alter the likelihood of bulimic-symptom expression. Although this provides flexibility in where to focus preventive and therapeutic efforts, our results suggest that modifying interoceptive deficits may be more effective than modifying thin-ideal internalization. Indeed, low thin-ideal internalization does not appear to prevent—but could lessen the severity of—bulimic symptoms, whereas low interoceptive deficits seems to serve a protective role. This distinction is useful given the current dearth of interoceptive awareness training programs (Boswell, Anderson, & Anderson, Reference Boswell, Anderson and Anderson2015) relative to the surplus of media literacy- and dissonance-based initiatives directed at reducing thin-ideal internalization (Yager & O'Dea, Reference Yager and O'Dea2008).
Our findings are especially relevant to the university context, which is considered a significant environmental risk factor for disordered eating (Compas, Wagner, Slavin, & Vannatta, Reference Compas, Wagner, Slavin and Vannatta1986). College girls who feel at risk for weight gain (and are thus likely to diet) could be targeted for prevention programs focused on emotional awareness, appetite monitoring, and peer social support for psychologically healthy eating habits. Such programs could also be universally implemented in residence halls, or perhaps introduced during middle school or high school in an effort to mitigate pre-existing risk.
Conclusions
To our knowledge, the present study is the third investigation in the eating disorders literature focused on age-related patterns of risk and the only investigation involving the full adolescent age spectrum. Our results emphasize the timeliness of moving away from questions of when or how and toward answering the when of the how to better understand the myriad ways bulimic symptoms might emerge in girls during early, middle, and late adolescence. Disparate findings for college girls versus middle- and high school girls call for continued study into the role of developmental context in the etiology of bulimia. Much work remains to be done in this area, but this study serves as an initial building block for researchers and clinicians alike.
Financial Support
This research was supported by the University of Notre Dame Graduate School and the University of Notre Dame Institute for Scholarship in the Liberal Arts.






