


Introduction
For almost three decades, spreader grafts have been employed by rhinologists and plastic surgeons to address the dorsal aesthetic line and prevent mid-nasal vault collapse during nasal surgery.Reference Sheen1 Originally, spreader graft placement was described for endonasal septal procedures. Currently, it is widely used in open rhinoplasties. However, alternative methods have been developed for endonasal placement, mainly to eliminate the disadvantages of open procedures and to decrease operation times.Reference Manavbasi and Agaoglu2
After a dorsal hump reduction, the upper lateral cartilages must be reinforced to prevent their collapse towards the nasal septum and to prevent internal nasal valve angle compromise.Reference Teichgraeber and Wainwright3 The major advantage of an open septal procedure is the optimal visualisation of the surgical field and the satisfactory fixation of the spreader grafts. A narrow internal nasal valve angle may also need to be widened without any hump reduction during classical (closed) septoplasty procedures. In contrast to the open approach, it is hard to manage a narrow internal nasal valve angle during classical endonasal septoplasty.
In this study, we present a novel method for spreader graft placement without dorsum resection, in patients who have a deviated septum with a narrow internal nasal valve angle.
Materials and methods
All procedures were conducted under general anaesthesia at Eskişehir Osmangazi University. A Killian incision was used for the septoplasty, and all spreader grafts were harvested from excised deviated septal cartilages.
Surgical technique
This technique has been developed for patients who have a narrow nasal valve angle. We believe that this technique is also useful for patients who have a deviated nasal septum with a narrow internal nasal valve angle, who have been diagnosed via endoscopic examination and a modified Cottle test.
The procedure begins with the Killian incision and bilateral mucoperichondrial elevation. After the creation of mucosal flaps, the spreader grafts are harvested from the excised deviated septal cartilage. The septal correction continues with excision of the bony septum. Mucoperichondrial flap elevation continues superiorly towards the upper lateral cartilage. The mucoperichondrium is elevated and protected up to the upper lateral and septal cartilage connection. Then, the harvested spreader grafts are sutured at each edge with 5-0 absorbable sutures, as shown in Figure 1.
Fig. 1 Spreader graft (lateral view).
After preparation of the grafts, the upper lateral and septal cartilage connection is incised from the septal cartilage with a scalpel, to create a space in which to insert the spreader graft (Figure 2). The nasal dorsum skin is lifted by being picking up with the fingers, to protect the nasal dorsal skin from incision. The spreader grafts are placed between the incised upper lateral cartilages and the septum. Needles are passed from the skin and pulled superiorly, and the graft is placed between the upper lateral cartilages and the septum. In this technique, because the nasal dorsum is not being elevated, upward movement of the graft is not expected.
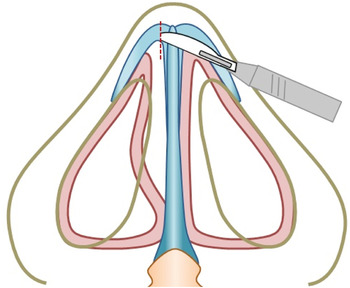
Fig. 2 Septal cartilage incision (inferior view).
At this position, it is not possible to attach the grafts by suture to the septum and upper lateral cartilages; the transseptal sutures inserted immediately below the spreader graft are the primary means for securing the grafts in place (Figures 3 and 4). The important step in this method is to pull the sutures superiorly while creating the transseptal sutures so as to achieve optimal graft attachment.

Fig. 3 Graft placement (lateral view).

Fig. 4 Graft placement (inferior view).
After attachment, the graft sutures are cut. The remaining steps are similar to those in a classical septoplasty.
Discussion
The internal nasal valve angle was first described by Zuckerkandl at the end of the nineteenth century, and was later named the ‘internal nasal valve angle’ by Mink at the beginning of the twentieth century.Reference Grigoryants and Baroni4 The internal nasal valve mainly consists of four anatomical units. It is formed medially by the nasal septal cartilage, laterally by the inferior turbinate, inferiorly by the bony pyriform aperture and superiorly by the caudal border of the upper lateral cartilage.Reference Miman, Deliktas, Ozturan, Toplu and Akarçay5
Maintaining the internal nasal valve angle within a normal range is important for proper physiological intranasal airflow. In the case of an over-resection of the dorsal septal cartilage or upper lateral cartilage during a septal nasal procedure, the nasal valve angle may become narrow. This may result in a restriction of the airstream, which decreases the local pressure. Consequently, a nasal vault collapse may occur during nasal inspiration.Reference Sheen1, Reference Wittkopf, Wittkopf and Ries6
Patients with either a narrow internal nasal valve angle or a resected nasal dorsum require reconstruction of the internal nasal valve to widen the internal nasal valve angle. Unfortunately, it is difficult to approach this area with open technique septoplasty in a patient with a narrow internal nasal valve angle without opening the nasal dorsum. However, nasal surgeons have modified their techniques to minimise the invasiveness of the interventions.
Our novel technique aims to address this objective. The advantage of our technique is the opportunity it provides to harvest autologous material for use as a spreader graft to correct the deviated septal cartilage. Although Reiffel et al.Reference Reiffel, Cross and Spinelli7 mentioned that foreign materials, such as Medpor®, are as satisfactory as autologous spreader grafts, it is a safer option to use autologous tissue or material if it can be obtained. Open techniques have other disadvantages, such as scar formation and post-operative nasal oedema, among others. It is possible to avoid such hazardous complications using our method.
To date, various types of endonasal spreader graft placement methods have been suggested as alternatives, to avoid the problems associated with open techniques. In these methods, either sutures, tissue adhesives or a submucoperichondrial pocket technique are used to attach the spreader grafts.Reference Yoo and Jen8–Reference Toriumi, Josen, Weinberger and Tardy10 The displacement of the graft is minimised with our suture technique, which is affixed immediately under the spreader grafts. Additionally, there is a reported increased risk of complications from infections when using adhesives compared to a suturing technique.Reference Toriumi, Josen, Weinberger and Tardy10
Although the endonasal placement of spreader grafts seems to be more difficult than placement conducted using an open approach technique, an endonasal procedure has many advantages. Currently, many types of endonasal placement techniques are available. Our technique provides surgeons with the opportunity to shorten the operation time, obtain autologous septal graft material and secure the columellar architecture. Surgeons familiar with the classical (closed) septoplasty procedure can easily apply this technique to widen a narrow internal nasal valve angle.
Our novel technique has been performed successfully in more than 20 patients. However, the lack of an objective assessment of nasal patency and the nasal valve by acoustic rhinometry and/or rhinomanometry is the major limitation of our study. Further reports on this technique that include objective measurements will be presented, and the results will be compared statistically.




