



The ages of about 10 to 14 years (early adolescence) can be an especially important time for identifying the early predictors of weight-related concerns and the onset of disordered eating (DE). This period of increased weight and appearance concern has been linked to changes in pubertal maturation and appearance (Stice, Reference Stice and Hayward2003; Wertheim, Paxton, & Blaney, Reference Wertheim, Paxton, Blaney and Thompson2004), as well as adolescents’ developing awareness that conforming to societal standards of attractiveness often brings higher social status with peers and in society at large (Borch, Hyde, & Cillessen, Reference Borch, Hyde and Cillessen2011). Although young adolescents can have a range of different concerns about their appearance, for many the main concern is about their weight, which can lead to maladaptive dieting and eating behaviors, such as purging of food and skipping meals (Fildes, Robbins, Cave, Perrens, & Wearring, Reference Fildes, Robbins, Cave, Perrens and Wearring2014; Slater & Tiggemann, Reference Slater and Tiggemann2010; Tylka & Sabik, Reference Tylka and Sabik2010). Our primary purpose in the present five-wave, 2.5-year longitudinal study was to identify early social and physical risk factors for growth in early adolescents’ DE behaviors, including purging food and skipping meals as two forms of DE most often motivated by weight concerns and attempts at weight loss or management. We aimed to determine how these risk factors might contribute to the internalization of appearance concerns. We investigated appearance anxiety as (a) an outcome of social and physical risk factors, and (b) a mediator linking early risk factors with DE.
A Biopsychosocial Model and the Tripartite Sociocultural Influence Model
Given the breadth of focus on sociocultural, psychological, and biological risks, a biopsychosocial model has been successfully applied to identify a multitude of risk factors that account for differential development of body dissatisfaction, weight and shape concerns, and DE during adolescence and beyond (Muris, Meesters, van de Blom, & Mayer, Reference Muris, Meesters, van de Blom and Mayer2005; Rodgers, Paxton, & McLean, Reference Rodgers, Paxton and McLean2014). Of most relevance to the present study, this model draws attention to biological risks, such a timing of pubertal development and body size (or body mass index; BMI), which are expected to be influential in the development of DE. By emphasizing the biological, as well as the social and the psychological, a biopsychosocial model adds to another widely supported theoretical model, the tripartite sociocultural influence model (TSIM; Thompson, Heinberg, Altabe, & Tantleff-Dunn, Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999), which details multiple social influences on body dissatisfaction and DE. In particular, the TSIM describes the central interactions with close others and related to consuming media that can trigger the internalization of appearance or body standards, comparisons with others, concerns about the body and appearance, and eventually DE. Peers and the media, and even the family, can provide powerful messages about the importance of appearance and weight management, sometimes serving to perpetuate weight and appearance concerns and behaviors to remedy perceived flaws (Menzel et al., Reference Menzel, Schaefer, Burke, Mayhew, Brannick and Thompson2010). Thus, key risk factors examined in the present study were peer appearance-related teasing, perceived media appearance pressures, and family appearance-related teasing, as well as pubertal development and BMI.
Risk factors for DE behaviors
Peer and family appearance-related teasing
Influences from peers, family, and the media are foundational components of the TSIM (Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999), and together, they represent sociocultural influences emphasized in the biopsychosocial model (Muris et al., Reference Muris, Meesters, van de Blom and Mayer2005). Peer weight- or general appearance-related teasing are quite prevalent among children and adolescents. Research has shown that about 1 in every 4 adolescents perceive that they are teased because of their weight (Libbey, Story, Neumark-Sztainer, & Boutelle, Reference Libbey, Story, Neumark-Sztainer and Boutelle2008), and a similar proportion report that they are teased by peers about their appearance more generally (Zimmer-Gembeck, Webb, Farrell, & Waters, Reference Zimmer-Gembeck, Webb, Farrell and Waters2018). Moreover, in multiple longitudinal studies, such peer teasing has been associated with concurrent and later elevations in DE, such as restrictive eating and bulimic behaviors (Fairweather-Schmidt & Wade, Reference Fairweather-Schmidt and Wade2017; Shroff & Thompson, Reference Shroff and Thompson2006), and appearance anxiety (Lavell, Webb, Zimmer-Gembeck, & Farrell, Reference Lavell, Webb, Zimmer-Gembeck and Farrell2018; Webb et al., Reference Webb, Zimmer-Gembeck, Mastro, Farrell, Waters and Lavell2015).
The effect of appearance-related teasing on DE is not limited to peers. Parental direct messages, such as teasing about appearance, have also been associated with appearance evaluative concerns and appearance anxiety, especially in younger adolescents (Phares, Steinberg, & Thompson, Reference Phares, Steinberg and Thompson2004; Webb et al., Reference Webb, Zimmer-Gembeck, Farrell, Waters, Nesdale and Downey2017). Moreover, in one study, weight-related teasing by parents was associated with adolescent girls’ restrictive eating behaviors even after controlling for BMI (Keery, Boutelle, van den Berg, & Thompson, Reference Keery, Boutelle, van den Berg and Thompson2005), and in a second study, weight-related teasing by parents, weight talk, and mothers’ dieting were all associated with a range of DE behaviors in girls (Neumark-Sztainer et al., Reference Neumark-Sztainer, Bauer, Friend, Hannan, Story and Berge2010). Overall, 57 studies of the associations of teasing (about weight or appearance by peers, parents, siblings, or others) and body dissatisfaction or DE were located in one meta-analysis (Menzel et al., Reference Menzel, Schaefer, Burke, Mayhew, Brannick and Thompson2010). After abstracting Pearson's correlations as effect sizes, 20 effect sizes were summarized for dietary restraint and 22 effect sizes were summarized for bulimic behaviors. The effect size for the association between weight teasing and dietary restraint was .35 (a medium effect; 17 studies) and the effect size for the association between weight teasing and bulimic behaviors was .36 (a medium effect; 18 studies). The effect size for the association between more general appearance teasing and DE could not be calculated as too few (only 2) studies were found. In this meta-analysis, teasing source (e.g., peers vs. family) could not be differentiated, suggesting that more research is needed that examines the influence on DE of peer teasing separate from family teasing.
Media appearance-related pressures
Media has long been known to have an important negative influence on adolescents’ body attitudes and appearance-related concerns (Thompson & Stice, Reference Thompson and Stice2001), and greater consumption of media has been found to be associated with reports of elevations in DE among young adolescents (Holland & Tiggemann, Reference Holland and Tiggemann2016; Latzer, Spivak-Lavi, & Katz, Reference Latzer, Spivak-Lavi and Katz2015; Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999; Tiggemann, Reference Tiggemann, Cash and Smolak2011). For example, in a systematic review of 20 studies that examined associations between social networking and body dissatisfaction or DE (Holland & Tiggemann, Reference Holland and Tiggemann2016), significant cross-sectional and longitudinal associations were described for adolescents and young adults (5 of 20 with a longitudinal component; 8 of 20 included only adolescents; 6 of 20 examined gender differences). Moreover, although multiple theories, including the TSIM (Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999), more specifically focus on the messages that sexualize and idealize the appearance of girls and women as a way to explain the effects of media, only 1 study found a gender difference in the impact of media. Such findings have led some to conclude that mass media is the most influential and pervasive cause of body and appearance dissatisfaction and, in turn, DE (e.g., Holland & Tiggemann, Reference Holland and Tiggemann2016; Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999; Tiggemann, Reference Tiggemann, Cash and Smolak2011). Research on media and DE has most often focused specifically on media consumption (i.e., level of use), but other research has measured perceived pressure from the media, defined as perceived feelings that the media promotes the importance of an ideal appearance and weight. Perceived pressure from the media has been described as both directly and indirectly associated with DE, and may be more relevant as a risk factor than use level (Stice & Whitenton, Reference Stice and Whitenton2002).
Pubertal maturation and BMI
Alongside the examination of sociocultural risk factors, pubertal development and BMI were considered as physical/biological risks for DE in the current study. Early adolescence is a time when pubertal maturation is prominently on view for others, can be quite varied in onset and presentation, and is often accompanied by weight gain. Just has been found for BMI (Brixval, Rayce, Rasmussen, Holstein, & Due, Reference Brixval, Rayce, Rasmussen, Holstein and Due2012; Fairburn, Welsh, Doll, Davies, & O'Connor, Reference Fairburn, Welsh, Doll, Davies and O'Connor1997; Gardner, Brown, & Boice, Reference Gardner, Brown and Boice2012; Helfert & Warschburger, Reference Helfert and Warschburger2013; Levinson et al., Reference Levinson, Rodebaugh, White, Menatti, Weeks, Iacovino and Warren2013; Wiklund et al., Reference Wiklund, Kuja-Halkola, Thornton, Balter, Welch and Bulik2018), earlier (i.e., more advanced relative to peers) pubertal maturation has been associated with DE (e.g., Graber, Brooks-Gunn, Paikoff, & Warren, Reference Graber, Brooks-Gunn, Paikoff and Warren1994; Haynos, Watts, Loth, Pearson, & Neumark-Stzainer, Reference Haynos, Watts, Loth, Pearson and Neumark-Stzainer2016; Levinson et al., Reference Levinson, Rodebaugh, White, Menatti, Weeks, Iacovino and Warren2013; for reviews see Ricciardelli & Yager, Reference Ricciardelli and Yager2016; Striegel-Moore & Cachelin, Reference Striegel-Moore, Cachelin, Johnson, Roberts and Worell1999; Wiklund et al., Reference Wiklund, Kuja-Halkola, Thornton, Balter, Welch and Bulik2018), appearance dissatisfaction and poorer body image (Rousseau, Rodgers, & Eggermont, Reference Rousseau, Rodgers and Eggermont2017; Rosseau, Trekels, & Eggermont, Reference Rousseau, Trekels and Eggermont2018), appearance anxiety (Webb, Zimmer-Gembeck, & Mastro, Reference Webb, Zimmer-Gembeck and Mastro2016; Zimmer-Gembeck et al., Reference Zimmer-Gembeck, Webb, Farrell and Waters2018), and peer teasing or criticism about appearance (Rosseau et al., Reference Rousseau, Trekels and Eggermont2018; Zimmer-Gembeck et al., Reference Zimmer-Gembeck, Webb, Farrell and Waters2018).
In the present study, we expected that adolescents, both boys and girls, with a higher BMI and more advanced pubertal maturation, would to be at greater risk for DE and appearance anxiety. Regarding pubertal maturation, previous longitudinal research findings suggest that it is more advanced physical signs of puberty that are associated with relative increases in appearance dissatisfaction (Rosseau et al., Reference Rousseau, Trekels and Eggermont2018) and appearance anxiety (Zimmer-Gembeck et al., Reference Zimmer-Gembeck, Webb, Farrell and Waters2018) for both boys and girls. Theories specifying the risks that may be associated with earlier pubertal maturation have concentrated on the changes in appearance, combined with biological and hormonal changes, which distinguish young people, making them more sensitive to social and emotional stressors than their later maturing peers (Somerville, Reference Sommerville2013). Moreover, in addition to the novel experience of early physical and social change relative to peers, earlier maturation is thought to disrupt the acquisition of adaptive skills and the gradual acceptance of development, resulting in risks for maladjustment (Petersen & Taylor, Reference Petersen, Taylor and Adelson1980). In particular, because of the relative novelty of early maturation in the peer group, there is little time for modeling of and experience with positive adaptation to physical development and accompanying social changes. This reduced time for transition can result in skill deficits for coping with the distress that can be associated with changing bodies and social relationships. In response, young people may be more attuned to their appearance and may try to modify or change it, resulting in associations of early maturation with emotional and appearance- or body-related responses, such as appearance anxiety symptoms and symptoms of DE.
Past research has specifically focused on pubertal timing relative to peers as a risk for DE, given that early puberty may be a greater risk for girls because it entails an increase in the fat-to-muscle ratio. This increase moves many girls away from the idealized image of the attractive thin female. In contrast, later maturation may be a risk for boys as puberty moves many boys closer to the idealized image of the attractive, muscular male. Research suggests gender differences in the impact of pubertal maturation; for example, in one study, earlier maturing girls and later maturing boys were more at risk for bulimic symptoms (e.g., McNicholas, Dooley, McNamara, & Lennon, Reference McNicholas, Dooley, McNamara and Lennon2012). Overall, however, the gendered pattern here is not completely clear. In a review, Klump (Reference Klump2013) concluded that the findings regarding pubertal maturation were relatively unequivocal for girls, with earlier pubertal timing and more advanced pubertal maturation (pubertal status) associated with more DE. In contrast, the findings were less clear for boys, with associations of pubertal status or timing with DE much weaker or mixed.
Appearance anxiety and DE
Internalization of appearance or body standards, comparisons with others, and concerns about the body and appearance are components of the TSIM that are mediating mechanisms expected to account for why peer, family, and media appearance-related pressures result in DE. To capture a component that reflects some aspects of these mediating mechanisms, we focused here on appearance anxiety. Appearance anxiety is defined as excessive concerns about appearance, preoccupation with perceived body and appearance flaws, and behaviors to check, change, or hide appearance (Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Gregertsen, Miyamoto and Farrell2018; Sharpe et al., Reference Sharpe, Griffiths, Choo, Eisenberg, Mitchison, Wall and Neumark-Sztainer2018; Veale, Reference Veale2004). Such appearance concerns can be a common experience during adolescence, but appearance anxiety differs from measures of body dissatisfaction and low body esteem, in that appearance anxiety taps symptoms representative of body dysmorphia, which include significant distress alongside behaviors that indicate a preoccupation with appearance such as repetitive grooming and checking of appearance (Greenberg et al., Reference Greenberg, Markowitz, Petronko, Taylor, Wilhelm and Wilson2010; Lavell et al., Reference Lavell, Webb, Zimmer-Gembeck and Farrell2018; Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Gregertsen, Miyamoto and Farrell2018; Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2014; Zimmer-Gembeck et al., Reference Zimmer-Gembeck, Webb, Farrell and Waters2018). Despite these differences between body dissatisfaction and appearance anxiety, just as has been found for body dissatisfaction and low body esteem (Brosof & Levinson, Reference Brosof and Levinson2017; Graber et al., Reference Graber, Brooks-Gunn, Paikoff and Warren1994; Haynos et al., Reference Haynos, Watts, Loth, Pearson and Neumark-Stzainer2016; Ricciardelli & Yaeger, Reference Ricciardelli and Yager2016; Smolak & Levine, Reference Smolak, Levine, Smolak and Levine2015; Striegel-Moore & Cachelin, Reference Striegel-Moore, Cachelin, Johnson, Roberts and Worell1999), appearance anxiety has also been associated with DE. In one study from the first wave of data used in the current study (Mastro, Zimmer-Gembeck, Webb, Farrell, & Waters, Reference Mastro, Zimmer-Gembeck, Webb, Farrell and Waters2016), young adolescents (N = 387, age 10 to 13 years) who reported more appearance anxiety were found to also report more purging of food, as well as poorer social functioning and perceptions of social competence. Another previous study using additional waves from this same data set has shown that, on average, appearance anxiety is quite elevated among girls and relatively common among boys even as early as the ages of 10 to 13 years (Zimmer-Gembeck et al., Reference Zimmer-Gembeck, Webb, Farrell and Waters2018). Just as concerning, dissatisfaction with appearance and other appearance concerns have been associated with concurrent and increasing DE among adolescents and young adults in other research (Hinrichsen, Waller, & Van Gerko, Reference Hinrichsen, Waller and Van Gerko2004; Levinson & Rodebaugh, Reference Levinson and Rodebaugh2012; Sharpe et al., Reference Sharpe, Griffiths, Choo, Eisenberg, Mitchison, Wall and Neumark-Sztainer2018; Turel et al., Reference Turel, Jameson, Gitimu, Rowlands, Mincher and Pohle-Krauza2018).
The focus upon appearance anxiety specifically is made more important by the evidence that it is a unique construct potentially more strongly associated with DE than the broader vulnerability of social anxiety. For example, in two studies we located, social anxiety itself was associated with DE (Ostrovsky, Swencionis, Wylie-Rosett, & Isasi, Reference Ostrovsky, Swencionis, Wylie-Rosett and Isasi2013; Sawaoka, Barnes, Blomquist, Masheb, & Grilo, Reference Sawaoka, Barnes, Blomquist, Masheb and Grilo2002), and eating and anxiety disorders have been described as highly comorbid conditions (Levinson et al., Reference Levinson, Rodebaugh, White, Menatti, Weeks, Iacovino and Warren2013). Yet, the common vulnerability of anxiety specifically related to appearance might explain this association and could be even more relevant to identifying those at risk of DE onset and progression. Testing this notion in US undergraduate students, Levinson and Rodebaugh (Reference Levinson and Rodebaugh2012) found, using a 16-item measure of fear of negative evaluation because of appearance (Hart et al., Reference Hart, Flora, Palyo, Fresco, Hollie and Heimberg2008), that a unique (concurrent) association of appearance anxiety with DE remained even after accounting for general social anxiety. Similarly, in a study of undergraduate women and men, Levinson et al. (Reference Levinson, Rodebaugh, White, Menatti, Weeks, Iacovino and Warren2013; Study 1, replicated in Study 2 with undergraduate women) found a strong correlation between social appearance concern and eating disorder symptoms (measured with the Eating Disorder Inventory–2; Garner, Olmstead, & Polivy, Reference Garner, Olmstead and Polivy1983). These later results (Levinson et al., Reference Levinson, Rodebaugh, White, Menatti, Weeks, Iacovino and Warren2013) emerged even after accounting for the associations of social anxiety, high standards, fear of negative evaluation, maladaptive perfectionism, BMI and gender with eating disorder symptoms.
Although this emerging evidence supports concurrent and unique associations between appearance anxiety and DE, we could locate only one longitudinal study reporting associations of appearance anxiety with DE, relying on a sample of undergraduate students and focusing only on binge eating, rather than weight-management related DE behaviors (Brosof & Levinson, Reference Brosof and Levinson2017). In this longitudinal study, young women reported on their appearance anxiety and binge eating three times over 6 months. Concurrent associations ranged from r = .33 to r = .50. In addition, appearance anxiety was associated with an increase in binge eating at the next wave, but the reverse association was not supported. We could locate no previous study of appearance anxiety as a correlate of purging and skipping meals among young adolescents, as well as a mediator linking early social and physical risk factors with DE.
Participant gender
As noted often in research on appearance and body image, DE, and pubertal maturation, gender must also be considered. It is widely reported that, from before adolescence and throughout most of the life span, women (and girls) are more susceptible to appearance pressures and report more body concerns, greater body dissatisfaction, and more appearance anxiety symptoms than men (and boys; Frisén, Lunde, & Berg, Reference Frisén, Lunde and Berg2015; Ricciardelli & Yager, Reference Ricciardelli and Yager2016; Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Gregertsen, Miyamoto and Farrell2018). In addition, the prevalence of many forms of DE is higher in young adult women than men (Striegel-Moore et al., Reference Striegel-Moore, Rosselli, Perrin, DeBar, Wilson, May and Kraemer2009), multiple forms of DE and rates of clinical eating disorders are much higher in adolescents girls than boys (Kinasz, Accurso, Kass, & Le Grange, Reference Kinasz, Accurso, Kass and Le Grange2016; Ricciardelli & Yager, Reference Ricciardelli and Yager2016), and women and men also seem to differ in age of onset and in their clinical presentation of eating disorders (Kinasz et al., Reference Kinasz, Accurso, Kass and Le Grange2016; Ricciardelli, Reference Ricciardelli and Wade2016). These gender differences are believed to be an outcome of many genetic, biological, and social factors, but one social influence that has been a prominent focus of research is the mounting actual or perceived sociocultural pressure to conform to appearance ideals for young women in order to enhance social acceptance and success in life (Bucchianeri, Arikian, Hannan, Eisenberg, & Neumark-Sztainer, Reference Bucchianeri, Arikian, Hannan, Eisenberg and Neumark-Sztainer2013; Piran, Reference Piran2010). However, it should be noted that this gender effect has been questioned in recent years (e.g., McCabe & Ricciardelli, Reference McCabe and Ricciardelli2004; Turel et al., Reference Turel, Jameson, Gitimu, Rowlands, Mincher and Pohle-Krauza2018). Nevertheless, gender differences remain important to examine in all analyses undertaken with the aim of identifying risk factors for appearance anxiety and DE. Thus, in the present study, we examined gender as a moderator by testing two-group (boy, girl) latent growth curve and path models. Moreover, we selected measures that have been used effectively in the past with both girls and boys.
The Current Study
In sum, the general purpose of the present five-wave, 2.5-year longitudinal study was to identify early risk factors of DE, including social risks of teasing about appearance (by peers and family members) and media pressure, as well the influences of BMI and more advanced pubertal maturation, among young adolescents. Bulimic symptoms and skipping meals were the two DE behaviors examined here. Three other behaviors were also assessed: binge eating food; using laxatives, diet pills, or diuretics; and using pills or power with the aim of reducing fat or building muscle mass. However, we did not examine these in this study given that it was rare for participants to report using laxatives (4 reported using once a month or less and 3 reported using more frequently, 1.9% overall), or using pills for fat reduction or building muscle (9 reported using once a month or less and 9 reported using more frequently, 4.8% overall). In addition, although more common (20.1% reported binge eating once a month or more at the first wave), binge eating was outside the domain of our focus on behaviors that we expected would be motivated by appearance anxiety and attempts to conform to appearance ideals.
Novel to this study is the focus on appearance anxiety as an influence on DE and as a mediator explaining why both sociocultural and physical/biological risk factors are associated with the development of DE. Moreover, we focused on whether models fit or differed for boys compared to girls. We had three general hypotheses. First, it was hypothesized that elevated initial levels and steeper growth in DE (modeled from Time 3 to Time 5; T3 to T5) would be predicted by all risk factors measured in Time 1 (T1) and Time 2 (T2), including appearance-related teasing, media pressure, higher BMI, and more advanced pubertal maturation. Second, the associations of each risk factor with initial levels and growth of DE was expected to be fully mediated by T3 appearance anxiety. Third, given evidence that it may be early maturing girls who are most at risk and girls often have a greater focus on weight loss or maintenance than boys, we expected that pubertal maturation and BMI would be more strongly associated with appearance anxiety and, in turn, DE (purging of food and skipping meals) in girls relative to boys. We did not expect any other gender differences in model paths to emerge.
Method
Participants
The participants were 383 boys (45%) and girls (55%) who participated in a five-wave, 2.5-year longitudinal study. At study entry, students were in Grades 5 to 7 and ranged from age 10 to 13 years (M = 12.0, SD = 0.90). Each wave was separated by 6 months, and by Wave 5, students were in Grades 7 to 9 and ranged from age 12 to 15 years (M = 15.7, SD = 0.93). Thus, given that all participants were in the adolescent stage of development by Wave 5, we use the term “adolescent” in the remaining sections. Most students endorsed White (79%) or Asian (15%) race/ethnicity. The remaining students endorsed a range of other sociocultural backgrounds. Students attended one of three participating schools in an urban area of Australia. A total of 395 students attempted participation, but 2 did not report any demographic information at any wave and 10 failed to provide information on DE for at least one wave. These 12 students were excluded from all analyses. Students reported their gender at each wave, and 8 students reported a different gender at only one (and not more than one) of the five waves. Because gender reported at T1 was always the gender reported at three (of the four) other waves and gender reported at the last wave was always the same as gender reported at the first wave, T1 reported gender was used in this study.
Measures
This study covered the early adolescent period and involved multiple reporters, with adolescents reporting their DE, appearance anxiety, experiences of teasing, and perceived appearance-related media pressures; height and weight (to calculate BMI) were measured by research staff, and pubertal maturation was reported by parents.
DE
At T3, T4, and T5, adolescents reported their purging of food (i.e., “Made yourself sick (vomited) to control your weight or shape”) and skipping meals (“Skipped a meal to control your weight or shape”) using two items drawn from the EAT-26 (Garner, Olmsted, Bohr, & Garfinkel., Reference Garner, Olmsted, Bohr and Garfinkel1982). These three waves were used for growth curve estimation so that risk factors and the mediator of appearance anxiety occurred prior to the first considered assessment of DE. T3 purging food and skipping meals were significantly correlated with the report of whether (no/yes) participants had been told they had an eating disorder, r = .19 and .21, respectively, both p < .01. T3 skipping meals (but not purging food) was significantly correlated with the report of whether (no/yes) participants had been told by a doctor to lose weight, r = .17, p < .01.
T3 appearance anxiety
At T3, the 10-item Appearance Anxiety Inventory (Veale et al., Reference Veale, Eshkevari, Kanakam, Ellison, Costa and Werner2014) was used to assess repetitive thoughts and behaviors associated with appearance concerns and worries. An example item is “I check my appearance (e.g., in mirrors, with photos).” Responses ranged from 1 (never) to 5 (always or almost always). The total score was formed by summing all items. Cronbach's α was excellent at .91 (.89 for boys and .92 for girls).Footnote 1
T1/T2 appearance teasing
At T1 and T2, four items derived from the weight teasing subscale of the Perceptions of Teasing Scale (Thompson, Cattarin, Fowler, & Fisher, Reference Thompson, Cattarin, Fowler and Fisher1995) were used to assess the frequency of perceived appearance teasing by peers (three items, same-gender and other-gender) and parents (1 item) and the associated distress. Items were revised to focus on appearance in general, rather than only weight (“… make fun of or tease you about your weight or looks”). Regarding family, participants reported how often family member(s) “… tease you about your weight or looks.” Frequency responses ranged from 1 (never) to 5 (very often). Distress ratings ranged from 1 (not at all upset) to 5 (very upset). The product of frequency and distress ratings was computed and items for peer teasing were averaged. Cronbach's α was good, .84 and .78 for peer teasing at T1 and at T2, respectively (.82 and .81 for boys; .85 and .76 for girls at T1 and at T2, respectively).
T1/T2 media appearance pressure
At T1 and T2, two items were used to assess perceived media appearance pressure (Webb, Zimmer-Gembeck, & Donovan, Reference Webb, Zimmer-Gembeck and Donovan2014). An example item is “I've felt pressure to look good from the media (e.g., TV, magazines).” Response options ranged from 1 (none) to 5 (a lot). Averaging items formed a total score, with a higher score indicating more pressure. Cronbach's α were good, at .87 and .76 at T1 and at T2, respectively (.88 and .69 for boys; .86 and .78 for girls at T1 and at T2, respectively).
T1 parent-reported pubertal maturation
At T1 and as part of the consent process, parents (n = 304, 79%) completed the Pubertal Development Scale (Petersen, Crockett, Richards, & Boxer, Reference Petersen, Crockett, Richards and Boxer1988) to rate their offspring's pubertal maturation across five characteristics, including height, body hair, skin change, breast growth (girls only)/voice change (boys only), menstruation (girls only), and facial hair (boys only). Response options for all items (except menstruation) ranged from 1 (not yet started or none) to 4 (seems complete/fully mature). Menstruation was reported as no (1) or yes (4). Items were averaged to create total scores for pubertal maturation, with higher scores indicating earlier maturation relative to others at the Wave 1 assessment. The Cronbach's α were acceptable at .76 for boys and .78 for girls.
T1 BMI
Trained research assistants measured participant height and weight. BMI was calculated as kg/meters2.
Procedure
Study approval was obtained from the Griffith University Human Research Ethics Committee (approval number 2013/13 titled “Appearance-Based Rejection Sensitivity From Childhood to Adolescence: Victimisation, Mental Health Consequences, and Rejection Resilience”) before principals were contacted for approval to conduct the study and students were given parental consent forms to take home and return to the school. To encourage the return of consent forms (regardless of parental consent to participate), a classroom-based celebration was held for the class within each grade, at each school, that returned the most consent forms. About one-half (58%) of the students returned consent forms to the school, with 9% of these parents declining to participate. The return and consent rate may have been adversely affected by the requirement that parents had to complete a short questionnaire to return along with the consent form. A small gift (e.g., novelty pen or sticker) was given to participating students after each survey was completed. Students were able to decline participation on the day of the survey; no student declined.
Overview of analyses
With regard to missing waves of assessment, 33 students failed to complete one wave (8.6%), 20 students missed two waves (5.2%), 10 students missed three waves (2.6%), and 11 students missed four waves (2.9%). In addition, 81 students were missing parent report of pubertal maturation. Missing data were estimated using multiple imputation with estimates made based on all measures included in this study (20 imputed data sets). Pooled means (Ms), standard deviations (SDs), and correlations across the 20 datasets are reported. Because a planned missingness design was used so that 50% of students completed information about family teasing and media pressure at T1 and the other 50% completed the items at T2, family appearance teasing and media pressure were merged to create single complete sets of T1/T2 scores for these two risk factors. In addition, to create a parallel measure for peer appearance teasing, T1 and T2 reports were averaged to produce composite T1/T2 peer appearance teasing scores. The merged scores were calculated prior to multiple imputation.
For the primary analyses, models of DE were fit using MPlus v.8.3 with robust maximum likelihood estimation to estimate initial levels and linear growth for boys and girls, and to examine the effects of all risk factors and the mediational role of appearance anxiety in DE. We began by estimating a two-group (boy, girl) growth model of DE, which we call a gender-conditional growth model. Given the findings from these gender-conditional models, we then made decisions about how best to test the predictors of DE for boys and for girls and fit additional models. In these models, we initially controlled for age at the first assessment. Yet, age was not significant in any model, so it was not included in the model results reported here.
Model fit was assessed with the χ2 test statistic and associated level of significance and the comparative fit index (CFI; Bentler & Bonett, Reference Bentler and Bonett1980). The CFI is more acceptable as the values approach 1 and values over .95 are considered indication of very good model fit (Hu & Bentler, Reference Hu and Bentler1999). In addition, the root mean square error of approximation (RMSEA; Browne & Cudeck, Reference Browne, Cudeck, Bollen and Long1993) provided an estimate of error due to approximate fit of the models, with RMSEA values below .05 considered good, values between .05 and .08 considered fair, and values between .08 and .10 considered mediocre fit (Kaplan, Reference Kaplan2000). Critical ratios were used to determine significance of model paths (t-test values above an absolute value of 1.96).
Results
Gender differences and correlations between measures
Means, standard deviations, and results of t tests comparing girls and boys on all measures are reported in Table 1. Skipping meals was higher in girls than in boys at each wave (T3 to T5), and girls reported more T3 appearance anxiety, peer and family teasing about appearance, and media pressure than boys. Girls, relative to boys, were reported by their parents to be more physically mature at T1, but average BMI did not differ. Finally, purging did not differ between boys and girls at any wave, and it should be noted that there was a very low average level of purging in boys at all times of measurement (just over the minimum possible level of 1). More specifically, 25 adolescents (7%; 9 boys and 16 girls) reported purging of food more than 2–3 times/month at some time. For skipping meals, 94 (24%; 23 boys and 71 girls) adolescents reported skipping meals at least 2–3 times/month at some time.
Table 1. Correlations between disordered eating and other study measures (N = 383)
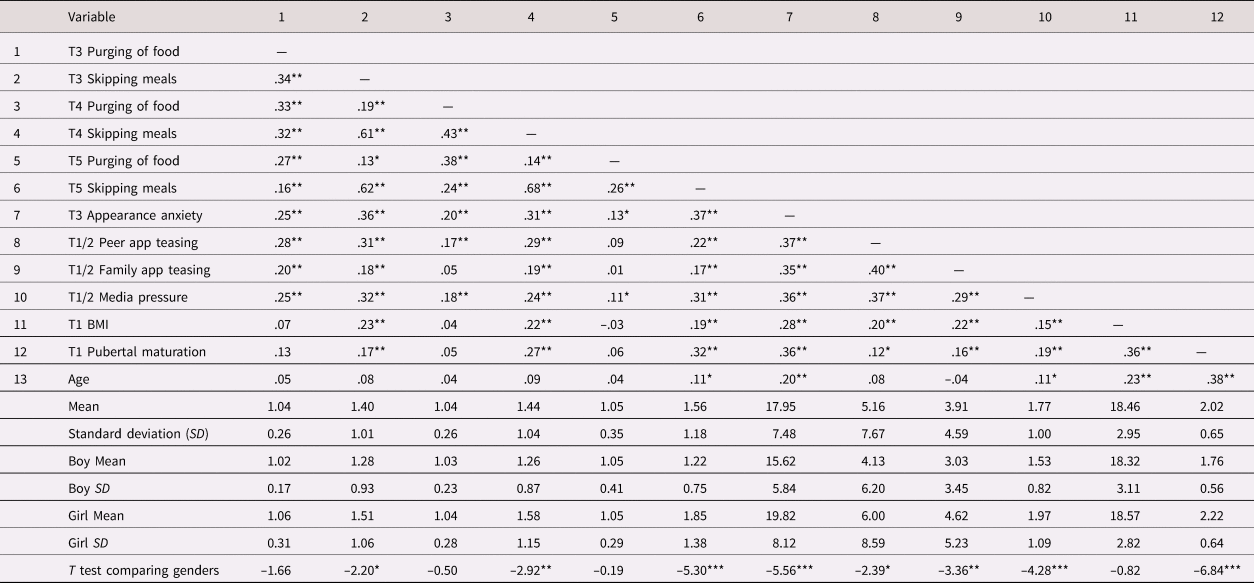
Note: T3, Time 3. T4, Time 4. T5, Time5. T1/2, merged across Time 1 and Time 2. App, appearance. BMI, body mass index. *p < .05. **p < .01.
As shown in Table 1, there were consistent associations of T3 appearance anxiety with DE across T3 to T5, and there were generally consistent correlations of T1/T2 peer teasing, family teasing, and media pressure with more elevated DE across T3 to T5 and with T3 appearance anxiety. T1 BMI and T1 pubertal maturation were positively associated with skipping meals but not purging, and age was only associated (positively) with one assessment of DE: T5 skipping meals.
Gender-conditional linear growth in DE
There were gender differences in the average linear growth models of purging and skipping meals. As shown in Table 2, boys’ initial levels of purging and skipping meals were significantly greater than 0, both p < .001, but there was no significant linear change in either form of DE, p = .340 and .248, respectively. In addition, the variance of the estimated initial levels was significant for skipping meals, p < .001, but not for purging, p = .071, and the variance in the slope was not significant in either model, p = .802 and .237, respectively. Thus, on average, boys reported some purging of food and skipping meals initially, but these reports did not significantly change over time and this lack of significant change did not vary across boys. The results for girls were somewhat different. Girls’ initial levels of purging and skipping meals were greater than 0, both p < .001, but different from boys, there was significant linear growth in skipping meals, on average, p < .01 (but no significant linear growth in purging, p = .937). Of note, also different from boys, there was variability in girls’ linear change over time for both purging and skipping meals, as well as in initial levels of both forms of DE, all p < .05.
Table 2. Results of two-group (boy/girl) unconditional growth curve models of purging of food and skipping meals (N = 383)

Note: Purging χ2 (4) = 5.94, p = .204, CFI = .99, RMSEA = .036, 90% CI [.000, .091], p = .588. Skip meals χ2 (4) = 6.21, p = .184, CFI = .99, RMSEA = .038, 90% CI [.000, .093], p < .564. *p < .05. **p < .01. ***p < .001.
Longitudinal predictive models of DE
Given the differences found between boys and girls in the gender-conditional growth curve models, gender-specific predictive models of purging and skipping meals were fit. In particular, because of the lack of linear growth, as well as the lack of variability in growth, of purging and skipping meals in boys, we reduced the data by averaging T3, T4, and T5 reports of DE to produce average level composite scores for each. Path models were then fit to test whether early risk factors were predictive of boys’ average level of purging and average level of skipping meals, while also examining T3 appearance anxiety as a mediator linking risk factors to DE.Footnote 2 In girls, given a significant average increase in skipping meals, as well as individual variability among slopes for both purging and skipping meals, latent growth models were fit to estimate individual girls’ initial levels and slopes of purging and skipping meals, while also testing the impact of risk factors and appearance anxiety as a mediator on growth patterns of girls’ purging and skipping meals.
Boys
Results of the path model predicting boys’ purging and skipping meals had an excellent fit to the data: χ2(6) = 4.66, p = .588, CFI = 1.00, RMSEA = .000, 90% confidence interval (CI) [.000, .086], p = .789. However, no risk factor nor appearance anxiety was significantly associated with purging, unstandardized estimates ranging from –.01 to .01, all p > .07. Thus, we removed purging from the model and fit a predictive model of the average level of skipping meals only. This model also had an excellent fit to the data: χ2 (5) = 1.55, p = .908, CFI = 1.00, RMSEA = .000, 90% CI [.000, .043], p = .961. As shown in Figure 1, only pubertal maturation was significantly associated with the mediator of appearance anxiety, while BMI was the one early risk factor directly associated with boys’ higher level of skipping meals. In addition, boys’ appearance anxiety was directly associated with skipping meals, and when indirect effects were tested, pubertal maturation had a significant positive indirect effect on boys’ skipping meals via appearance anxiety, with an unstandardized effect size of .11 (p = .024).

Figure 1. Results of a path model predicting boys’ average levels of skipping meals from T1/T2 risk factors and T3 appearance anxiety (n = 171). Average level represents average of disordered eating across Waves T3, T4, and T5. Unstandardized significant direct effects are shown here followed by standardized effects in parentheses; unstandardized indirect effects are reported in the text. All significant (p < .05) covariances between T1/T2 risk factors were freed but are not shown here. Model fit: χ2 (5) = 1.55, p = .908, CFI = 1.00, RMSEA = .000, 90% CI [.000, .043], p = .961. *p < .05. ***p < .001.
Girls
Figure 2 shows the significant path estimates from the conditional latent-variable linear growth curve model of girls’ purging and skipping meals. As can be seen, the fit of this model was good, χ2(23) = 38.44, p = .023, CFI = 0.96, RMSEA = .056, 90% CI [.021, .087], p = .341, and all T1/T2 risk factors were positively and significantly associated with the mediator of T3 appearance anxiety. In addition, of the five risk factors, it was media pressure that was directly associated with a higher initial level of purging, whereas three of the five risk factors (peer teasing, media pressure, and pubertal maturation) were all associated with a higher initial level of skipping meals. Regarding predictors of growth in DE, pubertal maturation had a direct positive effect on the estimated linear slope of skipping meals. Finally, regarding appearance anxiety as a direct correlate, girls’ anxiety was only associated with a higher initial level of skipping meals, and there were no significant indirect effects of early risk factors on DE via appearance anxiety. It should also be noted that there was no significant predictor of linear change in girls’ purging.

Figure 2. Results of a conditional latent-variable growth model predicting girls’ disordered eating from T1/T2 risk factors and T3 appearance anxiety (n = 212). Unstandardized significant direct effects are shown here followed by standardized effects in parentheses; no indirect effects were significant. All significant (p < .05) covariances between T1/T2 risk factors and between disordered eating measures were freed but are not shown here. Model fit: χ2 (23) = 38.44, p < .023, CFI = .96, RMSEA = .056, 90% CI [.021, .087], p = .341. *p < .05. **p < .01. ***p < .001.
Discussion
The aim of this study was to investigate appearance anxiety as a predictor of DE in young adolescents while also testing whether appearance anxiety served as a mediator accounting for why sociocultural and physical/biological risk factors impact on DE (Fairweather-Schmidt & Wade, Reference Fairweather-Schmidt and Wade2017; Menzel et al., Reference Menzel, Schaefer, Burke, Mayhew, Brannick and Thompson2010; Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999). Thus, in this five-wave longitudinal study, we considered early social and physical risk factors, measuring them in Grades 5, 6, and 7 students (ages 10 to 13 years) at the first two waves (T1 and T2), a mediator of appearance anxiety measured at T3 (Grades 6, 7, and 8), and modeled patterns of DE from T3 to T5 ending when participants were in Grades 7, 8, and 9 (ages 12 to 15 years). We focused on forms of DE expected to be associated with weight concerns or weight management, including purging food after meals and skipping meals. The early risk factors investigated were those that are described in the biopsychosocial model (Muris et al., Reference Muris, Meesters, van de Blom and Mayer2005; Rodgers et al., Reference Rodgers, Paxton and McLean2014) and the sociocultural risk factors were also identified from the TSIM (Thompson et al., Reference Thompson, Heinberg, Altabe and Tantleff-Dunn1999) and relevant to the development of social-evaluative concerns about appearance and weight (Menzel et al., Reference Menzel, Schaefer, Burke, Mayhew, Brannick and Thompson2010). These included physical/biological factors of BMI and pubertal maturation, which are known to be influential in DE, as well as appearance anxiety and sociocultural risks of peer teasing about appearance, parent teasing about appearance, and perceived media appearance-related pressure (Wiklund et al., Reference Wiklund, Kuja-Halkola, Thornton, Balter, Welch and Bulik2018; Zimmer-Gembeck et al., Reference Zimmer-Gembeck, Webb, Farrell and Waters2018).
In general, multiple early risks for DE were identified, especially for girls. In particular, the findings revealed more advanced pubertal maturation to be a common risk factor for DE in both boys and girls, a range of social risk factors only relevant for girls’ purging and skipping meals (especially media pressure to conform to societal standards), and higher BMI as primarily relevant to boys’ DE. Also common to both boys and girls was the finding that appearance anxiety is associated with more skipping meals, but not purging. Finally, regarding the proposed mediator of appearance anxiety, the impact of sociocultural and physical/biological risk factors on DE is generally direct and not mediated via appearance anxiety, except for boys whereby appearance anxiety mediated the association between physical maturation and skipping meals. Thus, overall, it appears that physical not social risk factors predict boys’ DE, but girls are influenced by social circumstances and their physical status. In addition, although there is some positive association between appearance anxiety and skipping meals in both boys and girls, appearance anxiety and DE appear to be relatively divergent outcomes of the early risk factors measured here.
Major study findings
More specifically, there are five major findings of this study to address. The first finding relates to gender differences and patterns of DE in boys and girls. Consistent with some past research (e.g., Neumark-Sztainer, Wall, Larson, Eisenberg, & Loth, Reference Neumark-Sztainer, Wall, Larson, Eisenberg and Loth2011; for a review see Ricciardelli & Yager, Reference Ricciardelli and Yager2016), girls are at higher risk for DE than boys, especially those related to weight management; our first general finding confirms this for skipping meals. We also found good fitting models for both boys and girls, but the parameter estimates for temporal patterns of purging food and skipping meals indicated no significant change over time, or even interindividual differences in change over time, among boys. In contrast, change in DE and more variability in patterns of DE were found among girls. Specifically, for girls, variability was evident in initial levels of purging and skipping meals, and despite the average stability of girls’ reports of their purging of food, in addition to the average increase in skipping meals over time, girls varied in these temporal patterns. Thus, our findings of generally low levels and little change in boys’ DE, especially purging, is consistent with past modeling of trajectories that has found general stability in the middle adolescent years (Davis, Guller, & Smith, Reference Davis, Guller and Smith2016), but we did find that there is some increase and significant variability in growth of girls’ reports of both purging and skipping meals during early to middle adolescence.
Given the low and generally stable level of boy's DE over time, but the variability in girls’ patterns, we tested different models for each gender. This involved modeling predictors of average level of DE for boys, but modeling predictors of initial levels and growth in DE for girls. This modeling approach led to a second key study finding regarding the risk factors and their associations with appearance anxiety. Specifically, it was pubertal maturation that was the predictor in common across the models for boys and girls. The other four risk factors of peer appearance teasing, family appearance teasing, media pressure, and BMI were associated with greater anxiety in girls, but these were not associated with boys’ appearance anxiety. Thus, associations cut across all measured risk factors for girls, supporting theories that have described and clarified the continuing dominant role of social interactions and messages about appearance concerns, particularly coming from the media, in adolescent girls (Harper & Tiggemann, Reference Harper and Tiggemann2008; Ricciardelli, McCabe, Williams, & Thompson, Reference Ricciardelli, McCabe, Williams and Thompson2007; Rosenblum & Lewis, Reference Rosenblum and Lewis1999; Webb & Zimmer-Gembeck, Reference Webb and Zimmer-Gembeck2014).
Extending on the above, the third key study finding is more specifically about the risk factors for DE, with, again, different findings for boys and girls. Social risk factors, specifically peer teasing and media pressure, were direct predictors of girls’ initially higher level of DE, as was pubertal maturation. Given there were no indirect effects of peer teasing, media pressure, or physical maturation on girls’ DE via appearance anxiety, this seems to suggest that girls may purge food and skip meals not because they are more anxious or concerned about their appearance relative to other girls, but for other reasons. One possibility not tested here is that teasing and media pressure, and even looking more physically mature, directly relate to purging and skipping meals, because they assist girls to feel that they can conform to peer group or societal ideals of thinness, which helps them to be more accepted by peers (Holland & Tiggemann, Reference Holland and Tiggemann2016; Rosseau et al., Reference Rousseau, Rodgers and Eggermont2017, Reference Rousseau, Trekels and Eggermont2018; Webb & Zimmer-Gembeck, Reference Webb and Zimmer-Gembeck2014). In one previous longitudinal study, positive associations were reported between being liked by peers and popularity with peers in early adolescence and greater eating pathology in early adulthood, even after controlling for poor body image and self-perceived physical appearance (e.g., Smink et al., Reference Smink, van Hoeken, Dijkstra, Deen, Oldehinkel and Hoek2018). Girls also are very aware that achieving societal standards of beauty can bring greater social status (Borch et al., Reference Borch, Hyde and Cillessen2011). Taken together, all of these findings suggest that girls’ DE may be a direct outcome of peer and media pressure to conform. In addition, DE in girls seems to be a direct outcome of physical maturation, which moves girls away from the appearance ideals they witness in media (Rosseau et al., Reference Rousseau, Trekels and Eggermont2018). All of these associations do not necessary involve appearance anxiety to have their impact on DE. Although appearance anxiety may also emerge as a concern about conforming and meeting societal ideals, it primarily involves engaging in repeatedly checking appearance and camouflaging appearance (Roberts et al., Reference Roberts, Zimmer-Gembeck, Lavell, Gregertsen, Miyamoto and Farrell2018; Sharpe et al., Reference Sharpe, Griffiths, Choo, Eisenberg, Mitchison, Wall and Neumark-Sztainer2018; Veale, Reference Veale2004). In other words, appearance anxiety may be one set of beliefs and responses that follow from a range of social and personal appearance pressures, not only those about weight or body shape, whereas DE may be a somewhat separate way of responding to pressures to conform to weight and body shape ideals more specifically.
A fourth key finding, which was probably the most surprising, was the finding of few significant correlates of appearance anxiety in boys, but also that the only indirect association of risk factors with DE via appearance anxiety occurred for boys. Boys who were reported by their parents as more physically mature in the earliest years of adolescence report more appearance anxiety relative to other boys, and this anxiety, in turn, is related to a higher level of DE (specifically, skipping meals). Thus, appearance anxiety is useful to consider as a mediator explaining when boys may skip meals, but we suspect that there are additional risk factors, not measured here, that also account for boys’ appearance anxiety and DE. For example, it may also be late maturation that puts boys at greater risk for DE (McNicholas et al., Reference McNicholas, Dooley, McNamara and Lennon2012), which (given the age of the sample at T1) we could not examine in the present study. It is also possible that the current risk factors might become stronger correlates of boys’ appearance anxiety and DE as the boys get older, moving into later adolescence and early adulthood. There is some evidence that social risk factors are more strongly associated with DE among middle to late adolescent boys relative to younger boys (e.g., Jackson & Chen, Reference Jackson and Chen2011), and eating disorders are known to onset in males later than in females (Ricciardelli, Reference Ricciardelli and Wade2016).
Finally, a fifth finding is the direct effects of risk factors on boys’ DE. For boys, it was only a physical factor (BMI) that was directly related to skipping meals, and we found no direct effects on purging. Clearly boys with a higher BMI are engaging in skipping meals, probably to manage weight, despite our finding that BMI did not directly relate to boys’ appearance anxiety. However, boys seem to rarely purge food, and it remains unclear from this study what might predict this behavior when it does occur.
Limitations, future directions, and conclusion
There are three limitations of this study, with associated future research directions, to raise here. First, the low level and low variability in purging and skipping meals in boys (and a focus on early to middle adolescents) may have been partly to blame for the more limited findings for boys relative to girls. There was also no significant interindividual variability in boys’ growth in purging or skipping meals, which limited our planned focus on growth curves of DE in boys. Although the focus on appearance anxiety as a mediator is novel in this study and a needed direction for understanding its role in DE for both boys and girls, future research might consider including additional DE behaviors to expand this model to include those that might be more common in boys, such as binging on food, emotional eating (Thompson et al., Reference Thompson, Kelly, Schvery, Brady, Courville, Tanofsky-Kraff and Shomaker2017), or “muscularity-oriented” DE (Murray, Accurso, Griffiths, & Nagata, Reference Murray, Accurso, Griffiths and Nagata2018). Moreover, there are alternative models that might be important to test in future research, such as considering (1a) associations between multiple forms of appearance concerns and DE simultaneously as they onset and change over time during adolescence, (b) how DE might have implications for later levels of appearance anxiety and peer and family relationships, and (c) other meditators that measure body dissatisfaction and esteem in addition to focusing on appearance anxiety symptoms.
Second, because consent forms were not returned by about 40% of the potential participants, the generalizability of the results may be compromised. Third, BMI and physical development were measured only at the first wave of data collection, and physical development was reported by parents and not by the adolescents themselves. There is some evidence that associations between pubertal maturation, peer teasing, and appearance beliefs may be slightly stronger if puberty was reported by adolescents themselves (Rosseau et al., Reference Rousseau, Trekels and Eggermont2018). Yet, we did expect that we captured pubertal development at an ideal time for measuring early maturation via parent observation, as participants were aged 10–12 years, a time of life when pubertal maturation may be under way for the very earliest maturers and parents may interact frequently with their children. However, not all parents may have been accurate observers of their offspring's development and relying on parents’ reports only at T1 limited our focus to a measure of pubertal maturation that could identify adolescents who looked most mature, but it was too early to identify those who would mature later than most of their peers. Early maturation for girls and later maturation for boys have been found to be risk factors for eating disorder symptoms (McNicholas et al., Reference McNicholas, Dooley, McNamara and Lennon2012). For BMI, it would have been useful to have assessments later as weight can change quite substantially during and after puberty, and later BMI measures might have been more strongly associated with appearance anxiety and DE than was found here.
Conclusion
This multireporter, five-wave longitudinal study was novel in that we examined patterns of DE related to weight management (purging and skipping meals) for boys separate from girls, identifying relatively more advanced pubertal maturation (reported by parents) as a risk factor that was common across boys and girls, with other social risk factors (peer teasing, media pressure, and family teasing) and BMI also influential for appearance anxiety in girls and BMI influential for skipping meals in boys. However, we found very little evidence that appearance anxiety is a mediator linking these risk factors to DE, with support for mediation only found for boys’ pubertal maturation. To build upon these findings, researchers should consider longitudinal research that begins in early adolescence and extends into later adolescence and young adulthood when increasing levels of DE may begin to emerge (Ricciardelli, Reference Ricciardelli and Wade2016; Ricciardelli & Yager, Reference Ricciardelli and Yager2016). It will also be important to expand on this study to examine other predictors and forms of DE while also collecting data throughout adolescence and into young adulthood (especially those relevant to boys such as muscularity-oriented DE; Murray et al., Reference Murray, Accurso, Griffiths and Nagata2018) or mediators (especially those relevant to girls such as internalization of the thin or the fit ideal; Uhlmann, Donovan, Zimmer-Gembeck, Bell, & Ramme, Reference Uhlmann, Donovan, Zimmer-Gembeck, Bell and Ramme2018).
Acknowledgments
We thank Professor Drew Nesdale and Professor Geraldine Downey for advice during the early stages of the larger project on appearance-based rejection sensitivity, from which these data were drawn. We also thank the students and the schools for their continued involvement, and acknowledge the important contributions from research assistants who were critical to the collection of quality data, including Shawna Campbell, Sarah Clear, and Tanya Hawes.
Financial support
This research was funded by Australian Research Council Discovery Grants DP130101868 and DP170102547.




