


Introduction
Conflicts, crises, social unrest, and disasters can affect the ability of a healthcare system to provide for the needs of its citizens.Reference Nelson, Simic and Beste1 A protracted crisis inevitably affects the skills of the health workforce. Most, if not all health workers surviving severe crises need intense and sustained education, training, and skills upgrading. The participation and input of the health workforce in health system recovery and reform planning is of upmost importance.Reference Ssengooba, Rahman and Hongor2 Disasters can be a vehicle for major development programs, and the political impact of damage and disruption can be a catalyst for wide-ranging social and health system changes.Reference Macrae3,Reference Stephenson and DuFrane4 Planning for sustained rehabilitation activities in health care must immediately be made while delivering emergency medical assistance during disasters.Reference Gardemann5 Planning the rehabilitation of human resources should be started as soon as possible after the precipitating event.Reference Pavignani6 Interest in human resource development should be a long-term priority in order to ensure a sustainable health workforce in a disaster-affected society.7 Worldwide evidence suggests that rehabilitation interventions in the health sector tend to downplay issues regarding human resources.Reference Macrae3 The disruption of the educational system in such societies forces education and training capacities to be stronger than usual.8
The World Health Organization (WHO) has prioritized post-conflict improvement and strengthening of primary health care worldwide.8 The Declaration of Alma-Ata in 1978 defined primary health care as: “essential health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and the country can afford to maintain at every stage of their development in the spirit of self-determination”. These principles made primary health care one of the WHO's core activities in post-war Kosovo.9 The strengthening of primary healthcare services and human resources has its rationale in improving the general health of populations. Many countries significantly improved their health indicators due to expanded primary healthcare networks. For example, from 1975 to 2006, Oman, Portugal, Chile, Malaysia, and Thailand were designated as the best-performing countries by regions for reducing under-five year mortality rate by at least 80%. These results were made possible by sustained political commitment and economic growth with associated investments in the health sector.10
Health Needs and Services in Kosovo
Kosovo's health services needed improvement even before the 1999 war. In 1995, the infant mortality rate in Kosovo was 23.6/1,000 live births, which was one of the highest infant mortality rates in Europe.11 In comparison, the 1995 infant mortality rate in Hungary was 10.7/1,000 live births, and in Germany was 5.3/1,000 live births.11 During the Kosovo war from March–June 1999, the crude mortality rate in Kosovo increased two or three times from the pre-conflict level to 0.72/1,000. Mortality rates peaked in April 1999 at 3.25/1,000 a month, due to the intensification of military operations.Reference Spiegel and Salama12 An emergency is defined by a crude mortality rate >1/10,000.13
Primary healthcare centers were characteristic of the former Yugoslav health system.Reference Albreht, Delnoij and Klazinga14 Before the war, primary health care in Kosovo was provided through Polyclinics or Health Houses and health posts called ambulantas.15,15 According to the WHO, the primary healthcare system in Kosovo was based on 26 municipal Health Houses, providing primary health care and specialist services, and 308 small health centers (ambulantas) with basic primary healthcare services provided by a generalist physician and a nurse. During the Kosovo crisis in 1999, there was minimal damage to health facilities, although many were looted of equipment. Importantly, many of the buildings and much of the equipment already had deteriorated due to a lack of maintenance and repair.15 The Kosovo health system after the war inherited: (1) damaged health infrastructure; (2) a health system oriented solely to curative health services; and (3) physician-centered health services.Reference Cami17 According to the WHO, most of the physicians in Kosovo lacked access to up-to-date medical information for an extended period of time pre-war, and were in need of continuing medical education and training.9 For nearly a decade, the physicians practicing in Serbia (including Kosovo) had been unable to access foreign medical literature, conferences, courses, and other forms of continuing professional education.Reference Nelson, Simic and Beste1 As part of the effort to rehabilitate primary health services in post-war Kosovo, the US-based, international, non-governmental organization (INGO), International Medical Corps (IMC), delivered an introductory education and training program on primary healthcare issues to Kosovar primary healthcare physicians. The hypothesis was that training would improve their ability to practice evidence-based and modern, primary health care. This paper describes and evaluates the effectiveness of the IMC's program provided to Kosovar primary healthcare doctors, and explains how it helped set the stage for recovery and further strengthening of primary healthcare services in Kosovo.
Methods
Setting and Participants
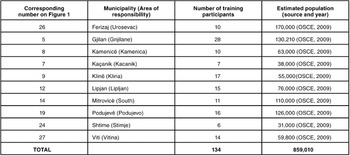
The IMC program for primary healthcare physicians was conducted in 1999 and 2000 in 10 Kosovo municipalities with an estimated population of 859,010 people.18 The IMC was appointed by the United Nations High Commissioner for Refugees (UNCHR) as the Health Coordinator in the areas designated as IMC's Areas of Responsibility (AOR; Table 1, Figure 1). The population of these areas mainly consisted of Albanians, although 10% belonged to other ethnicities, mostly Serbian. Most of the population was young, with 60% <25 years of age.Reference Buowa and Vuori19 The economy of Kosovo primarily depended on agriculture, and all AORs were somehow affected by the 1999 war. An initial assessment using focus groups with primary healthcare physicians and in-depth interviews with Health House Directors concluded that education and training of primary healthcare workers was considered to be one of the major health sector priorities in all of the targeted municipalities. Eight general practitioners were chosen in involved municipalities as local trainers from a pool of candidates recommended by Health House Directors. One public health specialist was selected as a trainer because of the importance of integration of public health methods within primary care.10 One medical technician was included on the team to represent mid-level primary healthcare workers and to provide their perspectives on primary healthcare issues. Panels of Health House representatives and IMC local/expatriate staff interviewed the candidates. One local trainer for each municipality was selected by the IMC, and confirmed by Health House personnel. Local trainers were seconded to the IMC, and would resume their usual PHC duties after the training period.

Figure 1. Map of Kosovo and its municipalities
A purposive sample of 134 program participants was selected from targeted municipalities (Table 1, Figure 1). The main inclusion criterion for their selection was that they were primary care physicians responsible for the implementation of primary healthcare services in their respective municipalities. The other important criterion for their inclusion was a keen interest in the education and training provided by the program and the commitment to continue to work in primary health care after participation. Personal characteristics and prerequisite qualifications were considered. The mean age of training participants was 38.1 ± 5.55 years, and the average time they had worked in medical practice prior to participation was 12.3 ± 5.26 years. A total of 42% of the training participants were women.
Table 1 Kosovo municipalities with their estimated population and the breakdown of training participants (OSCE = Organization for Security and Co-operation)
Intervention
Objective
The objective of the training intervention was to refresh and update the knowledge and skills of the primary healthcare physicians on common, primary healthcare issues. The learning objectives for each of the five training modules were designed by the international trainers after close and regular discussions with the local trainers and administrative supervising authorities (Table 2).
Table 2 Titles, learning objectives, and content of modules (PTSD = post-traumatic stress disorder)
Design
The intervention consisted of a comprehensive, multifaceted, educational program for four hours per week for six months. Thirty-two training sessions and an average of 128 hours were provided in each municipality. The three main intervention stages included: (1) curriculum development; (2) training of trainers; and (3) the intervention.
The curriculum was developed in English by the international staff with assistance from the local trainers. The curriculum was translated into written Albanian by the IMC local translators. The local trainers were trained by international staff, predominantly in spoken English. The written English and Albanian curricula were used to assist with the training of trainers for each module. The local translators assisted in the training of trainers using spoken Albanian as needed to clarify the curriculum. The modules were taught to the Health House primary care providers by the local trainers, in spoken Albanian, and occasionally Serbian. International staff assisted with the Health House training with use of simultaneous interpretation by local interpreters. Written evaluations were conducted in English; verbal assistance was provided in Albanian or Serbian, as needed. Verbal evaluations occurred in Albanian, Serbian, and English. Interpretation to English, as necessary, was accomplished by the local interpreters before analysis of the evaluations.
Local trainers participated in a one-month initial training course followed by one day of focused training before each new weekly topic. The trainers taught each module, including one practical training session per module for hands-on techniques in primary care. Training staff included three international and 10 local trainers. The main training center was established in Prishtina, the capital, and the municipalities were covered through weekly outreach activities. The training sessions were provided in the main Health Houses of the 10 targeted municipalities, and were delivered by international and local trainers. Active adult learning methods and participatory approaches were preferred to formal lecturing, although all methods were used. Discussion groups, case studies, problem-solving approaches, role plays, and hands-on were the preferred training methods.
Evaluation
Kirkpatrick's model of evaluation was used to assess the effectiveness of the intervention.Reference Kirkpatrick20 The evaluation was a continuous process, and focused on three levels of Kirkpatrick's model: (1) trainees' reactions, satisfaction, and perceived relevance to their work; (2) trainees' learning and changes in knowledge, skills, and attitudes; and (3) changes in actual behavior on the job.
Trainees' reactions were evaluated by open-ended questions during weekly training sessions, eliciting participants' appraisals about the training and its relevance to practice. Simultaneously, monthly focus groups with trainers and trainees provided valuable feedback in regard to the satisfaction of participants with the quality of lectures, performance of trainers, and perceived relevance of training to their work. The size of focus groups varied, with a minimum of five to a maximum of 25 people in each group. At least one-third of focus group participants were women. All data were complemented by participant observation to validate the initial needs assessment and guide the development of the training.
The group discussions during weekly training sessions and monthly focus groups were conducted by the local trainers in the field. International trainers rotated through the various training sites to assist with education, training, and evaluation sessions. Local interpreters accompanied the expatriate staff for verbal interpretation as needed. Local trainers were assigned to the same municipalities for the duration of the courses and developed good rapport with their trainees. Information gathered during the evaluation sessions was recorded by the local trainers and presented at the weekly trainers' meetings. The local and international trainers discussed concerns of trainees in an iterative fashion, in order to modify curricular design and presentation.
In order to evaluate Level 2, baseline knowledge was gathered by group discussions in the pre-training assessment period. These discussions helped to establish primary healthcare knowledge, skills, and attitudes toward primary health care. Post-course knowledge tests were designed in the field in close collaboration between international and local trainers. As preparation for the final test, 20-item, written, multiple-choice tests were used to evaluate knowledge of participants at the end of each module. A final, 20-item, multiple-choice test covering content of the all modules completed the process. The face validity of the tests was determined by local trainers, as a representative sample of the training participants in the population of interest. The content validity of tests was determined by the international staff, and it was satisfactory. The tests were in English because the majority of training participants were able to understand questions in English. The assistance of local trainers was given as necessary for translation from English into the local language (generally Albanian or Serbian). The evolution of knowledge, skills, and attitudes of participants toward primary health care were discussed at the weekly trainer meetings. Monthly interviews were conducted with randomly selected local trainers. The interview and focus group guide included quality of the training, suggestions for future topics, attitudes toward primary health care, and areas for improvement. All collected information served as guidance in the development of future modules.
Effects on actual practice (Level 3) were observed and evaluated through occasional supportive supervisions in the field conducted by international trainers.
Results
Level 1: Trainees' Reactions, Satisfaction, and Perceived Relevance to their Work
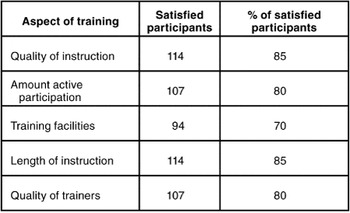
Loss of self-confidence was observed by both local trainers and training participants at the beginning of the course. Often, they were unwilling to demonstrate any lack of knowledge, particularly in front of their colleagues. However, with the moral and professional support of international trainers, the self-confidence of the local trainers and training participants increased; they asked questions and requested assistance. In all interview and focus groups, the majority of local trainers and the participants expressed satisfaction with various aspects of the course. No satisfaction ratings were <70% (Table 3). All of the trainees agreed that the training was relevant to their work in the primary care setting.
Table 3 Satisfaction of participants with different aspects of the training (n = 134)
Level 2: Trainees' Learning and Changes in Knowledge, Skills, and Attitudes
A pre-course assessment through group discussions with local trainers and trainees identified major gaps in knowledge and attitudes on primary healthcare issues. The majority of participants lacked problem-solving skills and possessed only basic theoretical knowledge of most common health problems. Most of them were skeptical about the role and efficacy of primary health care. All of the local trainers and a majority of the participants were highly motivated, and showed interest in sustaining their training efforts. Course attendance showed a steadily increasing trend from the beginning to end of the training period (Figure 2).
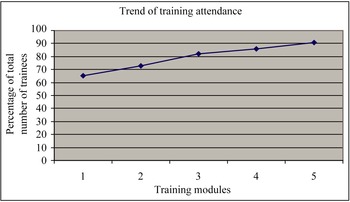
Figure 2. Trend of training attendance by training (1 = approach to patient; 2 = maternal child health; 3 = mental health; 4 = public health; 5 = common illnesses)
The mean of the scores on the final knowledge test was 14.6 ± 2.91 (73.0%) correct answers. The distribution of the test scores is in Figure 3. The likelihood of properly managing common health problems in primary care improved after completion of the course. Most of the trainees gradually changed their negative attitudes toward primary health care. The majority of trainers and training participants thought they should continue with their medical education after the training, either inside or outside the country.
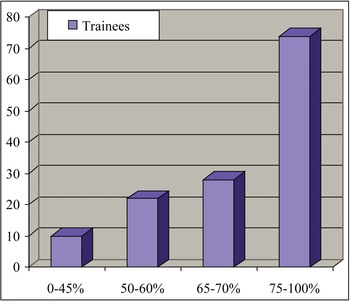
Figure 3. Distribution of training participants by test score (n = 134)
Level 3: Change in Actual Behavior on the Job
Most of the trainees were eager to implement their newly acquired knowledge and skills in primary healthcare settings. Supervisors in the field confirmed increased self-confidence of the majority of the participants. Supervisors' observations suggested an overall “good” level of team leadership and interactions with local health authorities, but persistent difficulties in changing actual behavior on the job. A gap between declared mastery and practice was observed in patient encounters.
Discussion
This descriptive study adds to the limited evidence base on strategies for education and training of primary healthcare workers as a part of post-disaster health sector improvements in resource-poor settings. Although reports and information on such interventions are available,21–Reference Pavignani and Colombo26PubMed and Ovid searches did not provide any case study or evaluation of primary healthcare physician training in post-conflict settings.
The rationale for selecting a comprehensive, six-month intervention in Kosovo was that Kosavar primary healthcare physicians lacked access to up-to-date medical education for an extended period of time pre-war. Physical, political, and socio-economic characteristics of the setting, along with attitudes and priorities of health workers exert a strong influence on the policy and structures of the health sector.Reference Macrae3,Reference Pavignani6 Kosovo's society had a strong interest in better educated physicians; physicians themselves were highly motivated to attend comprehensive education and training. The strong motivation of trainees in Kosovo and their interest in sustaining education and training efforts also was found in a study by Morikawa. Providing morale and collegial support at the field level encourages healthcare providers to learn in difficult environments during a disaster.Reference Morikawa16
Participation rates in the courses provided in Kosovo ranged between 65 and 91%, but the steady increase in attendance rates demonstrated that the participants' believed in the values of the training. Factors such as societal optimism and greater political stability may have influenced the attendance. In post-disaster settings, there may be an increased feeling of optimism and expectation of change due to an influx of human and material resources and heightened interest by the international community.7 Another post-disaster training project described higher participation rates (91–100%), but those courses were more focused and of shorter duration.Reference Driessche, Sabue and Dufour27 Improvement of self-confidence and self-esteem of practitioners have been noted after other training efforts.
The satisfaction of participants with different aspects of the course ranged between 70–85%. For comparison, 85% of the trainees assessed the benefits achieved as “excellent” or “very good” in a Saudi Arabian course directed at improving primary healthcare knowledge.Reference Abdel-Naser, Muzelil and Aladin29 In Alexandria, satisfaction with a course to improve educational knowledge and the skills of physicians ranged from 55.3% to 91.1%.Reference Seif El Din, Faten, Randa and Hoda30 All participants in Kosovo thought participation in the course was relevant to their work. Relevance of training to work also was found in other similar projects.Reference Dormael Van, Dugas and Kone28,Reference Omar, Gerein and Tarin31
Serious deficiencies in practical skills and clinical judgment of local trainers and course participants were observed, especially at the start of the course. Because of these observations, the course later focused more on problem-solving skills and development of a collegial atmosphere for case discussions.
The mean percentage of correct answers on the final knowledge test in Kosovo was 72.95%, compared to 84.9% in the above-mentioned trainings in Saudi Arabia and Alexandria, respectively. The courses provided in Saudi Arabia and Alexandria were not conducted in a difficult post-conflict environment. According to Walshe and Freeman, quality improvement interventions have highly variable results, which depend heavily on the context in which they are used and the way in which they are implemented.Reference Walshe and Freeman32 Proper management of common problems in primary health care also increased post-course in a study by Perez et al.Reference Pérez-Cuevas, Reyes and Guiscafre33
Supervisors in the field confirmed that it was more difficult to implement newly acquired skills than to understand them. Ridde et al reported that implementing the skills learned at the class sessions into the work environment was not an easy task for health professionals.Reference Ridde, Fournier and Banza34 Omar et al stated that the use of new knowledge and skills in practice is lower when respondents are not assisted with its. The factors that influence the transfer of education and training into practice include learner characteristics, the design and delivery of the course, and factors in the work environment, especially lack of involvement by senior management.Reference Omar, Gerein and Tarin31 The course provided in Kosovo raised awareness about the importance of primary health care, and changed the participants attitudes about the role of primary care practitioners. Dormael et al reported similar results in their case study of educating and training of primary healthcare workers.Reference Dormael Van, Dugas and Kone28
Limitations
The major limitation of this study was the non-probability sampling of the participants. However, the course was delivered to primary healthcare physicians in several municipalities spread around Kosovo, and the results from the intervention likely are generalizable to their colleagues throughout Kosovo. Unfortunately, the results of the intervention could not be compared with the cohort of primary healthcare doctors who did not participate in the intervention. Other limitations included time constraints and pressure for the INGO to initiate the intervention as soon as was possible. Therefore, participants were not administered a pre-test to evaluate their knowledge of primary healthcare issues before participation in the course. The evaluation of the program was not designed in advance, and the evaluations were iterative, but not formally designed as such. A shortage of educational resources prevented the provision of a proper implementation of hands-on training and supervision in the field. Although the IMC made an effort to deliver training to Serbian doctors, inter-ethnic tensions precluded the inclusion of certain ethnicities in the program. According to the University of New South Wales, the Albanian Kosovars assumed local control after the 1999 war.7 Consequently, ethnic Serbs developed their own health system and coordinated it with that in Serbia. This study is 10 years old, but does not include complete follow-up information on the participants.
Strengths
To the knowledge of the authors, this is the most comprehensive description of the educational and training of primary healthcare staff in post-war Kosovo. The intervention incorporated immediate emergency health relief as well as the long-term objective of health system rehabilitation in a resource-poor, developing country, post-disaster. The program was culturally sensitive and was proved acceptable to the local community.
Training attendance, as indicated by the high level of engagement of primary healthcare professionals over the six-month period, increased progressively from the beginning to the end of the program; this progression indicates that the program was well-adjusted to the local circumstances and demands. Participants in the course boosted the motivation of primary healthcare workers to continue upgrading their medical knowledge and skills. The course was in accordance with the primary healthcare strategy for Kosovo, as defined by the WHO.Reference Buowa and Vuori19 It served as an introductory course to the transition from general practice to family medicine and facilitated the establishment of a Family Medicine specialization in Kosovo.Reference Hedley and Maxuni35 The IMC's curriculum on primary healthcare issues titled, Introduction to Family Medicine, was provided to the WHO in Kosovo for use in their more comprehensive, two-year, Family Medicine program. During 1999/2000, the Training Centre in Prishtina served as the main training center for primary health care for almost one-third of Kosovo. One of the IMC's local trainers became the first chair of the Association of Family Physicians in Kosovo.
Primary health care and family medicine have continued to evolve in Kosovo. A Department of Family Medicine was added at the Kosovo University, and there is continuing education and training of family medical physicians through its residency program. Several of the IMC trainers from this study's intervention now are educators in family medicine. One of the trainers leads the Department of Primary Care in the Ministry of Health. The WHO continues to assist with family medicine training; the field director at the WHO also was employed by the IMC. Other IMC trainers completed the Family Medicine residency, and continue their work in the delivery of primary care services.36 A follow-up study would be required to elucidate further details on the evolution of primary care and Family Medicine in Kosovo.
Suggestions for Future Research
Further studies of various courses for the education and training of primary healthcare workers in other disaster or post-disaster settings are recommended. Comparative trials and follow-up would generate more credible evidence on the effectiveness and sustainability of the interventions. Also important for future research on course development, is the design of program evaluation simultaneously with overall program design, according to formal program evaluation methods available from multiple sources, including USAID.Reference LaFond and Brown37 It is important to assess sustainable changes in the practices of primary healthcare workers and the participation of course graduates in continuing medical education. Future research should quantify specific outcomes and inputs of education/training interventions in post-disaster settings, e.g., quality of trainers, mode of delivery, and educational techniques. These processes may be hampered by the focus of most international agencies on short-term technical programs rather than broadly defined and comprehensive health interventions.Reference Cueto38 Targeted training interventions on specific health problems also could improve the quality of primary health care,Reference Pérez-Cuevas, Reyes and Guiscafre33 and may be the preferred choice for disaster or post-disaster settings. There is much need to assess and refine the design of training interventions in disaster settings.
Conclusions
This retrospective, descriptive study has demonstrated the feasibility of a comprehensive education and training intervention of primary healthcare workers in one resource-poor, developing country, post-conflict. Participation in the course by primary healthcare doctors in Kosovo was a successful quality-improvement intervention. Participation in the course improved theoretical knowledge and the skills of primary healthcare doctors on primary care issues, and it boosted their motivation to further upgrade their professional knowledge and skills. This intervention has the potential to be reproduced in other post-disaster environments, especially in resource-poor, developing countries with a degraded or neglected health system, e.g., Afghanistan and Iraq. The choices and designs of the interventions depend on the context and population-specific features, but can be guided by prior successes.
Abbreviations:
AOR = Areas of Responsibility
IMC = International Medical Corps
INGO = international non-governmental organization
OSCE = Organization for Security and Co-operation in Europe
WHO = World Health Organization






