


Introduction
Due to rates in developed countries demonstrating that people change residences more frequently in childhood than in adulthood (Jelleyman & Spencer, Reference Jelleyman and Spencer2008), the ramifications of childhood relocation has gained increasing research attention. A growing body of literature suggests that children who have changed residences are at higher risk for adverse outcomes, including suicidal behavior (Qin et al. Reference Qin, Mortensen and Pedersen2009), psychiatric disorders (Adam, Reference Adam2004; Jelleyman & Spencer, Reference Jelleyman and Spencer2008), substance use (Dewit, Reference Dewit1998; Brown et al. Reference Brown, Benzeval, Gayle, Macintyre, O'Reilly and Leyland2012), criminal convictions (Gasper et al. Reference Gasper, DeLuca and Estacion2010), and academic difficulties (Chen, Reference Chen2013; Hutchings et al. Reference Hutchings, Evans, Barnes, Demmler, Heaven, Hyatt, James-Ellison, Lyons, Maddocks, Paranjothy, Rodgers and Dunstan2013). Several hypotheses exist as to why relocation is associated with adverse outcomes. Relocation may result in the severing of social ties and a disruption in familiar surroundings (Durkheim, Reference Durkheim1951; Wray et al. Reference Wray, Colen and Pescosolido2011), which could, for example, increase one's risk for subsequent suicidal behavior (Stack, Reference Stack2000). Or, relocations may be a marker of confounding pre-existing parental psychiatric disorders, parental unemployment, disorganized family life, or low family income (Pribesh & Downey, Reference Pribesh and Downey1999; Leventhal & Brooks-Gunn, Reference Leventhal and Brooks-Gunn2003; Dong et al. Reference Dong, Anda, Felitti, Williamson, Dube, Brown and Giles2005; Fomby & Cherlin, Reference Fomby and Cherlin2007; Dupere et al. Reference Dupere, Leventhal and Lacourse2008; Jelleyman & Spencer, Reference Jelleyman and Spencer2008). Despite the frequently assumed causal relation (Haynie et al. Reference Haynie, South and Bose2006; Jelleyman & Spencer, Reference Jelleyman and Spencer2008), drawing causal inferences between relocations and adverse outcomes remains problematic (Scanlon & Devine, Reference Scanlon and Devine2001; Adam, Reference Adam2004). Previous studies examining the effect of childhood relocation are limited primarily by: (1) small sample sizes that limit the statistical power and generalizability (Jelleyman & Spencer, Reference Jelleyman and Spencer2008; Nock et al. Reference Nock, Borges, Bromet, Cha, Kessler and Lee2008a ), (2) a lack of rigorous control of measured covariates (Jelleyman & Spencer, Reference Jelleyman and Spencer2008), and (3) inferring a causal relation without sufficiently exploring plausible genetic and environmental confounding factors (Rutter, Reference Rutter2007).
Given the importance of rigorously examining plausible alternative explanations when causal claims have been made (Shadish et al. Reference Shadish, Cook and Campbell2002; Rutter, Reference Rutter2007), this paper aims to examine the relation between childhood relocations (i.e. before age 12 years) and a variety of adverse outcomes by including more extensive measured covariates and comparing differentially exposed cousins and siblings using data collected in population-based, longitudinal, Swedish registers. Although previous studies have highlighted the vulnerability of relocations in adolescence (Qin et al. Reference Qin, Mortensen and Pedersen2009; Paksarian et al. Reference Paksarian, Eaton, Mortensen and Pedersen2015), we focused specifically on childhood relocations due to the minimal literature examining this age range. We examined the extent to which relocations are independently associated with suicide attempt, severe mental illness, substance abuse, criminal convictions, and academic achievement. We hypothesized that the population-wide risk for adverse outcomes associated with relocations would be attenuated after accounting for numerous offspring (i.e. sex, birth parity, maternal smoking during pregnancy, mothers’ cohabitation at offspring birth, parental age at childbearing) and parental covariates (i.e. educational attainment, country of origin, suicide attempt, suicide, severe mental illness, substance abuse, criminal history, and ranked, average family income) and controlling for unmeasured environmental and genetic confounds shared by cousins and siblings.
Method
Data
After approval from the Institutional Review Boards at Indiana University and the Regional Ethical Review Board in Stockholm, Sweden, we generated a dataset linking information from ten longitudinal, population-based and healthcare registers using a personal identification number assigned to all Sweden residents at birth. The registers were: (1) the Medical Birth Register, which provides detailed birth information for more than 95% of pregnancies in Sweden beginning 1 January 1973 (Swedish Centre for Epidemiology, 2003), as well as offspring antenatal and perinatal information; (2) the Multi-Generation Register, which can be used to determine biological and adoptive familial relationships for all individuals born after 1932 or have been living in Sweden since 1961 (Statistics Sweden, 2010); (3) the Statistics Sweden Regional Register (SSRS), which records an annual dichotomous change in residence beginning in 1983 (Statistics Sweden, 2013); (4) the Integrated Database for Labor Market Research (LISA), which provides longitudinal market labor information (e.g. income level, marital status, unemployment status, social welfare status, disability status, etc.) on all individuals over the age of 16 beginning in 1990 until the end of 2008, as well as an annual count of residential changes (Statistics Sweden, 2011); (5) the Cause of Death Register, which contains the date and contributing cause(s) of deaths since 1 January 1952 (Statistics Sweden, 2010); (6) the National Patient Register, which includes International Classification of Diseases Eighth, Ninth, and Tenth Revisions (ICD-8, ICD-9, ICD-10) codes (Janssen & Kunst, Reference Janssen and Kunst2004) and dates for hospital inpatient admissions since 1 January 1969 (Jacobsson, Reference Jacobsson2009); (7) the Migration Register, which records dates for immigrations to and emigrations from Sweden since 11 September 1901 (Statistics Sweden, 2010); (8) the National Crime Register, which records all criminal convictions (i.e. for both non-violent and violent offenses), the date, and the sentence since 1 January 1973 for all citizens aged ⩾15 years (Fazel & Grann, Reference Fazel and Grann2006); (9) the Education Register, which includes information since 1970 on the highest level of completed formal education, divided into seven ordinal groups from fewer than 9 years of education to postgraduate education (D'Onofrio et al. Reference D'Onofrio, Singh, Neiderhiser, Iliadou, Lambe, Hultman, Långström and Lichtenstein2010); and (10) the National School Register, which includes a continuous measure of academic performance aggregated across 16 subjects since 1989, and Swedish language tests since 1987 for all students graduating from 9th grade at approximately age 16 years (the Swedish National Agency for Education, 2011). Additional information about the registers can be found elsewhere (e.g. D'Onofrio et al. Reference D'Onofrio, Class, Rickert, Larsson, Långström and Lichtenstein2013a ).
Sample
The population cohort in this study included individuals who were born in Sweden between 1 January 1983 and 31 December 1997. Using this time-frame enabled us to define childhood relocations in terms of residential address changes occurring before the age of 12 and follow individuals on our main outcomes through 2009. Specifically, we wanted to ensure exposure to the risk factor (i.e. childhood relocations) occurred before any measured outcome to more accurately assess the independent association between relocation and later adverse outcomes (Kraemer et al. Reference Kraemer, Kazdin, Offord, Kessler, Jensen and Kupfer1997). In addition, previous research has demonstrated that the validity of suicide attempt and severe mental illness younger than age 12 is unknown (D'Onofrio et al. Reference D'Onofrio, Class, Rickert, Larsson, Långström and Lichtenstein2013a ).
Starting with 1 594 532 observations from the Medical Birth Register, we excluded individuals sequentially starting with stillbirths (n = 3608), offspring with any congenital malformation (n = 63 790), and those with missing or invalid information for sex (n = 65). We then excluded individuals who had no relocation data in SSRS (n = 10 227), as well as one individual born after 1990 who was missing relocation data from LISA. Next, we dropped all recorded cases of suicide attempt (n = 3892) or suicide (n = 2) that occurred before the age of 12. Due to the lack of documented information on predictor and outcomes variables during time spent outside of the country, we also excluded those who migrated before age 12 but subsequently returned to Sweden and had a later recorded suicide attempt (n = 473) or suicide (n = 9). Finally, we excluded individuals for whom the maternal age at childbearing was under 9 years (n = 6), the age of death was less than 0 (n = 1), and the recorded date of suicide did not match the date of death (n = 1). In total, we excluded 5.27% (n = 84 069) of individuals born from 1983 to 1997, leaving a final cohort of 1 510 463 individuals, which included 2.38% (n = 35 940) from multiple births. Table 1 presents a summary of offspring-specific characteristics for the study cohort.
Table 1. Descriptive summary of offspring and parental covariates for cohort with individuals born between 1 January 1983 and 31 December 1997

a Based off 1 510 463 unique offspring born 1983–1997.
b Denotes percentages that are rounded to nearest hundredths and thus may not equal 100.
c Indicates the reference group.
d Based off 882 574 distinct mothers and 882 000 distinct fathers.
e Based on fathers of the mother's first-born child.
f Indicates a covariate with no missing variables, and thus the reference group was ‘No’.
Measures
Relocation predictors
We operationally defined relocations using information recorded in two different registries: (1) SSRS, and (2) LISA. Table 2 presents the distribution of SSRS and LISA relocations. The first (SSRS) began in 1983 and records relocations to and from homogenous, geographic clusters called Small Areas for Market Statistics (SAMS) areas. Statistics Sweden defines SAMS areas as either sub-divisions of municipalities nested within large municipalities or electoral districts nested within small municipalities (Statistics Sweden, 2015). There are ~1000 people in each SAMS area in Sweden with the exception of Stockholm, which averages ~2000 people per area (Sundquist et al. Reference Sundquist, Winkleby, Ahlén and Johansson2004). It should be noted that data in SSRS are collected annually and can account only for a move between two different SAMS areas from one year to the next. Thus, we assumed that the number of SSRS relocations was an underestimate of the actual number of relocations for an individual and used data from a second register, LISA, for our sensitivity analyses. The LISA register contains a count of the total number of moves between different residential addresses within the same year starting in 1990. For each individual in the cohort, we used two different predictor variables indexing childhood relocations by summing each measure from ages 0 to 11 years. Because SSRS has a longer time span, we used the summed SSRS variable in the main analyses and the summed LISA variable for the sensitivity analyses. An ROC analysis using relocations as measured using LISA data as the reference variable indicated that relocations estimated using SSRS data from 1990 to 2008 has both high sensitivity (0.82) and very high specificity (0.99).
Table 2. Grouped frequency distributions of the total number of childhood relocations (ages 0–11) as measured by SSRS- and LISA-based data

SSRS, Statistics Sweden Regional Register; LISA, integrated database for labor market research.
a Denotes a variable in which the percentages are rounded to the nearest hundredths and thus may not equal 100.
b Based off 1 510 463 unique individuals born 1983–1997.
c Based off 836 074 unique individuals born 1990–1997.
d Reference group.
Adverse outcomes
The five main outcomes under study were: (1) suicide attempt, defined as the first uncertain or certain attempt requiring inpatient hospital admission at age ⩾12 years (Tidemalm, Reference Tidemalm, Långström, Lichtenstein and Runeson2008); (2) severe mental illness (i.e. either schizophrenia or bipolar disorder), defined as the first inpatient hospitalization at age ⩾12 years (Lichtenstein et al. Reference Lichtenstein, Yip, Bjork, Pawitan, Cannon, Sullivan and Hultman2009); (3) substance abuse, defined as the first inpatient hospitalization at age ⩾12 years (Tidemalm, Reference Tucker, Marx and Long2008; D'Onofrio et al. Reference D'Onofrio, Rickert, Långström, Donahue, Coyne, Larsson, Ellingson, Van Hulle, Iliadou, Rathouz, Lahey and Lichtenstein2013c ); (4) criminal conviction, defined as the first criminal conviction at age ⩾15 years (Fazel et al. Reference Fazel, Grann, Carlström, Lichtenstein and Långström2009a ); and (5) low grade point average (GPA) in 9th grade, which consisted of a continuous measurement of GPA ranked into quintiles and further dichotomized, with the first quintile considered ‘low GPA’ (Lambe et al. Reference Lambe, Hultman, Torrång, MacCabe and Cnattingius2006). Note that individuals who were born after 31 December 1994 were missing criminal conviction data, as these individuals were not yet 15 years of age at the conclusion of the study. Likewise, individuals born after 1992 were not used in the analyses of low grades, which indexed performance at age 16. Finally, if offspring had not received a diagnosis or conviction within the study period, they contributed person-time at risk until death, emigration, or the end date of follow-up (31 December 2009), whichever came first. Thus, the risk period began at age 12 for all outcomes except criminal convictions, which began at age 15.
Appendix A lists the ICD codes and provides further information about the outcomes. Appendix B shows the tetrachoric correlations among the main outcome variables, while Appendix C lists Kaplan–Meier estimates of survival outcomes, including death by suicide. (See Supplementary online material for Appendices A–M.)
Covariates
Measured offspring-specific covariates were sex, birth parity, maternal smoking during the beginning of pregnancy, maternal cohabitation status with biological father at time of offspring birth, and parental age at childbearing. The parental-specific covariates for this study were highest level of completed formal education, country of birth, suicide attempt, death by suicide, lifetime history of severe mental illness (i.e. either schizophrenia or bipolar disorder), inpatient substance abuse, and criminal convictions. Details of all measured covariates are provided in Table 1. We additionally controlled for the average familial income, measured using percentile ranks that were computed annually to account for inflation and/or transient unmeasured disturbance. For those born before 1990 (i.e. the first year of LISA), calculation of ranked average familial income began in 1990 and ended when the individual reached age 12 years. All offspring in the cohort had at least 3 years of income data available.
Analyses
We first calculated Pearson product-moment and tetrachoric correlations to quantify the bivariate association between number of relocations and the offspring and parental covariates. Next, for each outcome, we fit four regression models (described below) that sequentially adjusted for measured confounders and unmeasured familial confounders. We estimated all models using SAS v. 9.3 (SAS Institute Inc., USA) and Stata v. 13.1 (StataCorp., USA). We used Cox regression to estimate the effect of childhood relocations on the age at the first diagnosis or criminal conviction where age was measured in units of years rounded to the nearest 0.001; to estimate the effect of childhood relocations on low GPA, we used binary logistic regression. Model 1 (i.e. cohort baseline model) estimated the association between the number of childhood relocations and each outcome while accounting for both sex and birth parity. Model 2 (i.e. adjusted model) additionally included all offspring- and parental-specific covariates. We used robust (sandwich) estimation, clustering on the maternal identifier, in both models 1 and 2 to account for the non-independence of observations at the nuclear family level. Model 3 (i.e. fixed-effect, cousin comparison model) compared differentially exposed cousins to account for genetic and environment factors shared by cousins. Before fitting this model, we created a subset of the main cohort by identifying all pairs of offspring who had the same maternal grandmother identifier but different maternal identifiers. Each pair was then assigned a unique numeric identifier code. There were 1 271 618 observations (i.e. 635 809 distinct cousin pairs) from 530 809 distinct offspring in the cousin cohort subset. We obtained fixed-effects estimates by: (1) using the cousin pair identifier as a strata variable during Cox and logistic model estimation, and (2) using robust standard errors to account for repeated data from individuals belonging to more than one cousin pair. Although model 3 does not completely eliminate genetic and environmental confounding, it accounts for 6.25% or 12.5% of genetic contributions from half- and full-cousins, respectively (D'Onofrio et al. Reference D'Onofrio, Lahey, Turkheimer and Lichtenstein2013b ). To account for additional genetic confounding, model 4 (i.e. fixed-effect, sibling comparison model) compared differentially exposed siblings by stratifying on the maternal identifier. Note that the intraclass correlation (ICC) between siblings measured using SSRS-based relocations variable was considerably higher compared to cousins (i.e. 77% v. 18%, respectively). The sample includes 425 833 discordant cousin pairs for relocations and 350 910 discordant sibling pairs.
After fitting the population and covariate-adjusted models for the survival outcomes, we evaluated the proportional-hazards assumption by testing for a non-zero slope in the linear regression of the scaled Schoenfeld residuals on time. If the covariate-specific or global tests indicated that the assumption did not hold, we fit additional models that included parameters representing the interaction between relocations and categorical age (i.e. <19 as the reference, 20–23, and ⩾24 years). We also performed an extensive set of sensitivity analyses to address limitations inherent to our definitions of particular constructs and to our dataset.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Results
Table 3 presents the correlations estimates between the covariates and the relocation data from SSRS and LISA. While all the covariates were associated with the frequency of relocations, the magnitudes of correlation were largest for maternal (r = −0.25) and paternal (r = −0.20) age at childbearing, closely followed by familial average income (r = −0.21), maternal (r = 0.18) and paternal criminality (r = 0.16), and maternal (r = 0.14) and paternal substance abuse (r = 0.12). Thus, frequent relocations are associated with younger parental age at childbearing, lower socioeconomic status, and more parental substance use problems and criminality.
Table 3. Sample bivariate correlations between relocations (measured by SSRS and LISA) and offspring and parental covariates

SSRS, Statistics Sweden Regional Register; LISA, integrated database for labor market research.
All correlation coefficients p < 0.05 for the test H o: ρ = 0. Offspring sex is not included in the table.
Table 4 and Fig. 1 present the results of the Cox regression models predicting suicide attempt, severe mental illness, substance abuse, and criminal convictions from continuous SSRS relocations. For model 1 (i.e. cohort baseline model), the observed hazard ratio (HR) for relocations predicting suicide attempt was 1.19 [95% confidence interval (CI) 1.12–1.18], indicating that each additional annual relocation increases the risk for attempting suicide by 19%. After adjusting for measured covariates in model 2, the magnitude of the association was attenuated (HR 1.08, 95% CI 1.07–1.09), but remained robust. The association was slightly weaker in model 3, which compared differentially exposed cousins (HR 1.07, 95% CI 1.05–1.09). Only in model 4, which compared differentially exposed siblings, was the association fully attenuated (HR 1.00, 95% CI 0.97–1.04). A similar pattern of results was observed for severe mental illness, substance abuse, criminal convictions, and low GPA (i.e. the cohort-wide associations were attenuated when accounting for offspring and parental covariates, and attenuated even further when controlling for genetic and environmental factors shared by cousins and siblings). Appendix D provides the exact HRs and odds ratios (ORs) and 95% CIs that are presented in Fig. 1. Appendix E lists the parameter estimate and standard error for each covariate for the main outcomes in models 2 and 4 (i.e. the adjusted population and sibling comparison model, respectively).
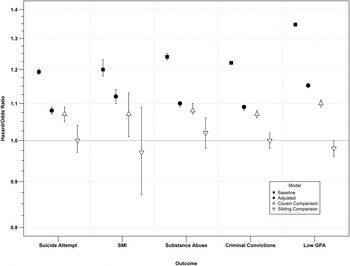
Fig. 1. Point estimates and 95% confidence intervals for the association between childhood relocations and adverse outcomes across models.
Table 4. The association between number of childhood relocations as measured by SSRS and suicide attempt, severe mental illness, inpatient hospitalization for substance abuse, criminal conviction and low GPA

SSRS, Statistics Sweden Regional Register; GPA, grade point average; b, estimated regression coefficients; s.e. standard error.
a Based off cohort size of 1 510 463.
b Based off cohort size of 1 271 618.
c Based off cohort size of 974 008.
d Based off cohort size of 865 983.
We found no evidence that the proportional-hazards assumption was violated for the models predicting suicide attempt and severe mental illness. By contrast, tests rejected the null hypothesis of zero slope for both criminal convictions and inpatient substance abuse, indicating that the log HR function is not constant over time. To address this further, we estimated the baseline and covariate-adjusted models including two additional parameters representing the interaction between relocations and categorical age. Although the interaction terms were statistically significant, the magnitudes of the differences in estimates for criminality and substance abuse were quite small (see Appendix F for details).
We used sensitivity analyses to examine several alternative explanations of our main findings and to address generalizability issues across different measures of the exposure and outcomes. First, we fit the full covariate-adjusted model 2 to a subset of the data that excluded individuals who were missing a maternal grandmother identifier (n = 153 515, see Appendix G) to determine whether or not those with missing maternal grandmothers systemically differed from those without missing maternal grandmothers. Results were analogous to model 2 on the full sample (see Appendix D). Second, we fit models 1–3 predicting (1) death by suicide (determined with certainty using ICD codes) to compare with previous literature regarding the effect of relocations and death by suicide specifically (Qin et al. Reference Qin, Mortensen and Pedersen2009), and (2) four continuous measures of academic performance (i.e. GPA, achievement in Swedish, mathematics, and English tests) to examine the validity of our derived dichotomous outcome indexing low GPA. The results (see Appendix H) of the models predicting suicide, GPA, and achievement test scores all mirrored the pattern of findings in the main analyses. Third, we re-estimated models 1–3 on a subset of the cohort for the main outcomes (see Appendix I) and for death by suicide and academic performance (see Appendix J) using the LISA-based relocations variables to explore the extent to which findings using the more detailed measurement for relocations agreed with the analyses based on SSRS data. Although LISA spanned fewer years, we observed the same pattern of attenuation in risk association with relocations across models as in the main analyses. Fourth, we categorized the continuous, SSRS-based measurement of childhood relocations into three groups representing no moves (reference category), 1–2 moves (dummy coded 0/1), and ⩾3 moves (dummy coded 0/1). We used the re-parameterized models to detect potential nonlinear associations between relocations and the outcome. Results for models 1–3 using categorical relocations (see Appendix K) are consistent with those from the main analysis using a continuous representation of relocations as a predictor – the risks associated with more relocations were attenuated with additional statistical and methodological controls for confounding factors. Fifth, due to the fact that SAMS areas are sub-divisions of municipal districts, we analyzed an annual change in municipality to capture relocations across broadly defined geographical areas (see Appendix L). Results were similar regardless of whether we defined relocation as a change in SAMS area or municipal district. Finally, we analyzed two separate age ranges (i.e. 0–5, 6–11) to explore sensitive periods of childhood relocation (i.e. early and late childhood; see Appendix M) because relatively few studies examined developmental periods in relation to childhood relocations (Anderson et al. Reference Anderson, Leventhal, Newman and Dupéré2014). Offspring who moved between the ages of 6–11 were at an increased risk compared to offspring who moved before age 6, although risk progressively attenuated across the four models, consistent with the results of the main analyses. In sum, the results of each sensitivity analysis were commensurate with those in the main analyses and followed a similar pattern of risk attenuation.
Conclusions
The current study sought to address the limitations of past literature by examining the associations between relocations specifically in childhood and later adverse outcomes using an extensive list of measured covariates and family-based, quasi-experimental designs (D'Onofrio et al. Reference D'Onofrio, Lahey, Turkheimer and Lichtenstein2013b ). We first showed that an increase in the frequency of relocations was associated with numerous other risk factors. Those who relocated in childhood were more likely to have been born to young parents and have parents who abuse substances, have lower incomes, and engage in criminal activity, which supports previous research (Dohrenwend et al. Reference Dohrenwend, Levav, Shrout, Schwartz, Naveh, Link, Skodol and Stueve1992; Karriker-Jaffe, Reference Karriker-Jaffe2013; U.S. Census Bureau, 2013). We then utilized analyses to incorporate both measured covariates and family-based comparisons, including the comparison of differentially exposed cousins and siblings. Overall, the findings suggest that previous studies may have overstated the magnitude of the independent association between relocation and later adverse outcomes. Instead, our findings suggest that the associations are more likely due to: (1) the correlates of relocation (Jelleyman & Spencer, Reference Jelleyman and Spencer2008) and (2) genetic and shared environmental factors associated with suicide attempt, severe mental illness, substance abuse, criminal convictions, and academic achievement (Bondy et al. Reference Bondy, Buettner and Zill2006; Brent & Melhem, Reference Brent and Melhem2008; Lichtenstein et al. Reference Lichtenstein, Yip, Bjork, Pawitan, Cannon, Sullivan and Hultman2009; Kendler et al. Reference Kendler, Sundquist, Ohlsson, Palmer, Maes, Winkleby and Sundquist2012). The risk for adverse outcomes attenuated when controlling for genetic and shared environmental confounds, regardless of the sensitive period in which a child moved. However, future studies should further explore the role of sensitive periods when examining risk factors for a variety of adverse outcomes.
This study was strengthened by the use of multiple approaches and designs to more precisely examine the independent associations between relocation and suicide attempt, psychiatric problems, and low academic achievement. The ICCs between cousins and siblings (i.e. 18% v. 77%, respectively) demonstrate the likelihood that siblings move together within family units, and thus siblings are less likely to be differentially exposed to relocations. Thus, the cousin comparison model strengthens the external validity of the findings (i.e. the siblings may not be representative of the entire population), while the sibling comparison model strengthens the internal validity because the design controls for more genetic and environmental factors (D'Onofrio et al. Reference D'Onofrio, Lahey, Turkheimer and Lichtenstein2013b ). Additionally, the large sample size enabled us to estimate associations for outcomes with low base rates (Saha et al. Reference Saha, Chant, Welham and McGrath2005; Nock et al. Reference Nock, Borges, Bromet, Cha, Kessler and Lee2008a ) and provide a more diverse cross-section of the population (Adam, Reference Adam2004). The inclusion of extensive sensitivity analyses reduced the possibility that our results were influenced by our construct definitions or limitations inherent to the registers. For example, results were unaffected regardless of our definition of relocations. In addition, this study examined relocations before age 12, thus expanding upon previous studies that have highlighted the vulnerability of relocations specifically in adolescence (Qin et al. Reference Qin, Mortensen and Pedersen2009; Paksarian et al. Reference Paksarian, Eaton, Mortensen and Pedersen2015).
Conversely, there are several limitations to this study. First, the register-based measurements of the psychiatric outcomes reflect more ‘severe’ outcomes (e.g. suicide attempt and substance abuse), although we replicated results with a variety of other outcomes that covary with suicide attempt and substance abuse (Fazel et al. Reference Fazel, Långström, Hjern, Grann and Lichtenstein2009b ; Lichtenstein et al. Reference Lichtenstein, Yip, Bjork, Pawitan, Cannon, Sullivan and Hultman2009; Webb et al. Reference Webb, Långström, Runeson, Lichtenstein and Fazel2011). Second, we were unable to explore moderating factors, such as the motive behind relocating (e.g. if relocation is due to a ‘crisis,’ the effect may be more detrimental) (Tucker et al. Reference Tucker, Marx and Long1998), or the population density and neighborhood deprivation of the post-relocation area (Pedersen & Mortensen, Reference Pedersen and Mortensen2001). Despite this, previous research has demonstrated that the association between relocations to more dense or deprived neighborhoods and schizophrenia, for example, is negligible when controlling for unmeasured familial risk factors shared by cousins and siblings (Sariaslan et al. Reference Sariaslan, Larsson, D'Onofrio, Långström, Fazel and Lichtenstein2015). Third, the results are based solely on Swedish data, which may not generalize to other countries or cultures. However, current research suggests that the associations between risk factors and suicidal behavior, for example, are relatively consistent cross-nationally despite socioeconomic, racial, ethnic, and cultural diversity amongst a variety of countries (Nock et al. Reference Nock, Borges, Bromet, Alonso, Angermeyer, Beautrais, Bruffaerts, Chiu, de Girolamo, Gluzman, de Graaf, Gureje, Haro, Huang, Karam, Kessler, Lepine, Levinson, Medina-Mora, Ono, Posada-Villa and Williams2008b ). Fourth, while the main analyses demonstrate a pattern of attenuation with increased control for measured and unmeasured covariates, sibling comparison analyses suggested that offspring who relocate more may actually be at a decreased risk for low grades (see Appendix D) but remains an open research question for future studies. However, previous literature parallels our findings suggesting that students who perform poor in school are exposed to disadvantages that better explain the relation between relocations and poor grades (Pribesh & Downey, Reference Pribesh and Downey1999). Finally, we were unable to measure school mobility. While we analyzed moves amongst municipal districts, and thus captured a greater geographical area possibly indicating school changes, our measure of residential mobility was only an indirect measure of school mobility.
The results suggest that clinicians should not discount relocation as a risk factor for adverse outcomes (as there is still an association in the population model) but rather refocus intervention and prevention programs. Inquiring about relocations may serve as an indicator of exposure to co-occurring risk factors (e.g. parental substance abuse). Importantly, federal programs that aid children who frequently change residences (e.g. in military families or children in foster care) focus on educational transition, such as ensuring a timely high school graduation (Anderson et al. Reference Anderson, Leventhal, Newman and Dupéré2014). We argue that these programs should not only consider educational outcomes, but a wide range of risk factors that are associated with both relocations and other adverse outcomes.
Future studies will need to replicate this study, particularly in other countries. Additionally, because we did not include possible interactions among childhood relocations and adverse outcomes (e.g. the role of socioeconomic status), future research would benefit from these analyses. In sum, this study illustrates the importance of using rigorous research designs to test plausible alternative hypotheses, especially when studying early risk factors (D'Onofrio et al. Reference D'Onofrio, Lahey, Turkheimer and Lichtenstein2013b ); studies that are unable to apply such designs may overestimate the magnitude of causal influences (Academy of Medical Sciences Group, 2007).
Supplementary material
For supplementary material accompanying this paper visit http://dx.doi.org/10.1017/S0033291715002469.
Acknowledgements
This study was supported by the National Institute of Child Health and Development (B.M.D., HD061817); Indiana Clinical Translational Institute Project Development Teams (B.M.D.); the Swedish Council for Working Life and Social Research and the Swedish Research Council through the Swedish Initiative for Research on Microdata in the Social and Medical Sciences (C.A., 340-2013-5867).
Declaration of Interest
None.







