


Introduction
In response to the need for the discipline of Disaster Health to build its science on data that are generalizeable and comparable, a Disaster Logic Model (DLM) and a set of five Frameworks have been developed to structure the information and research of the health aspects of disasters. This model and the Frameworks provide a standardized format for studying and comparing the epidemiology of disasters as well as for evaluating the interventions (responses) provided prior to, during, and following a disaster. The components of each of these Frameworks are deconstructed, defined, and simplified in order to describe the interactions and to identify the underlying evidence. The DLM and Frameworks are conceptual, and, as with all conceptual models, they are dynamic, open to challenge, and will evolve as new evidence is gleaned. Although these disaster Frameworks may be useful for other purposes (eg, operations), they were created specifically for the systematic study of the health aspects associated with a disaster. The details of the DLM and each of the Frameworks and supporting information are provided in the individual papers that follow this Overview. A discussion of research and evaluation as they apply to the study of disasters is included.
Disaster Research
Research is a studious inquiry or examination; an investigation or experimentation aimed at the discovery and interpretation of facts, revisions of accepted theories or laws in the light of new facts, or the practical application of such new or revised theories or laws.Reference Birnbaum, Daily, O’Rourke and Loretti 1 These definitions can be applied to the study of the epidemiology of disasters and to evaluating the interventions (responses) used before, during, and following disasters.
Goals of Disaster Research
The ultimate goals of conducting disaster research are to obtain evidence that can be used to: (1) decrease the risks that a hazard will produce a disaster; (2) decrease the mortality associated with disasters; (3) decrease the associated morbidity; and (4) enhance the recovery of the affected population or the population-at-risk. And decrease the risks that a hazard will produce a disaster. Although, in theory, dead victims should not create a burden for the Medical Care and Public Health Systems, it is important to define the mechanisms and causes of death in order to develop interventions to mitigate the numbers of deaths from future events. Deaths that potentially could have been prevented should be studied. Pain and suffering are inevitable components of disasters, but often their occurrence and severity can be mitigated if methods to minimize these problems, whether related directly or indirectly to the damages caused by the event, are identified.
Recovery is complete only when the pre-event status of the essential functions of the affected community is restored. Recovery of the affected individuals and population often is slow and incomplete. There is little documentation regarding the recovery from the functional damages created by an event. Research is essential to identify ways to enhance the speed and comprehensiveness of recovery from a disaster.
Various stakeholders have different needs for disaster research findings. For example, donors look to research findings to support those interventions demonstrating maximal efficiency and minimum waste. Responders to a disaster look to evidence from research to determine appropriate competencies and interventions. All of the stakeholders require knowledge from epidemiologic studies of a disaster that define what to expect when a hazard becomes manifest as an event and progresses to a disaster. Although there is an abundance of information of health changes in relation to disasters, most of the information exists in the grey literature (not scientifically peer-reviewed) and lacks the structure necessary for comprehensive analyses and comparisons.
Research studies involving the evaluation of the interventions provided before, during, and after an event are scarce, particularly the evaluation of the outcomes and impacts of the interventions provided.Reference Guralnik and Friend 2 Unfortunately, baseline, pre-event inventories often are not available, which complicates the interpretation of the findings. In addition to evaluating the effects (outputs), outcomes, impacts, and costs of specific interventions, it is important to study the processes used in order to determine critical points of success/failure in the process and to avoid future errors. Few such studies currently exist, but they are essential to establishing standards and best practices and to determine accountability.
In order to move out of the current morass in Disaster Health research and develop a standardized format for obtaining information, a DLM and five Frameworks for structuring the research and evaluations of the epidemiology of disasters and interventions used are provided: (1) Conceptual; (2) Temporal; (3) Societal; (4) Relief/Recovery; and (5) Risk-Reduction. The first three of these Frameworks are useful in both epidemiological and interventional research, while the Relief/Recovery and Risk-Reduction Frameworks are exclusive processes used in interventional disaster research. These Frameworks provide the structure necessary for analysis and reporting, and they will facilitate comparisons of various components of a disaster. Each of these Frameworks is described briefly.
The Conceptual Framework
The Conceptual Framework has been derived from the initial framework described in Volume 1 of the Guidelines. 3 (p35) Basically, the Conceptual Framework outlines the progression of the occurrences that lead to a disaster, beginning with a hazard that becomes an event, that causes structural damage and losses of essential functions (functional damage), that, in turn, are synthesized into needs that lead to an emergency or disaster (Figure I-1). Critical to all five Frameworks is the inclusion of standardized definitions of the terms used.

Figure I-1 The Basic Conceptual Framework.
Hazard
A hazard is anything that poses a danger or threat. Hazards contain potential energy that, if altered or released, may cause damage to living beings, and/or infrastructure, and/or the environment. Hazards may be natural, human-made, or a combination of both. 3 (pp56-68) Natural hazards are classified as seismic (or geophysical), meteorological (climatic), biological, nuclear, combined, or other (Table I-1). Human-made (anthropogenic) hazards may be classified as technological, economical, or related to the potential of humans to create conflict or fear (terrorism). Some hazards, such as poorly constructed buildings and existing seismic activity, represent a combination of natural and human-made hazards. Some of the energy of some hazards is used to provide goods and/or services for the benefit of the population (ie, generation of electricity, nuclear isotopes, reservoirs of water, and nuclear power plants). In such circumstances, the release of too much or too little energy may create a damaging event.
Table I-1 Classification of Hazards (Modified from the Guidelines 3 )

Event
An event is the actualization of a hazard; it is the release of too much or too little energy that has the potential to negatively affect living things and/or the environment. 3 (p151) The change in the rate or amount of energy (too much or too little) may upset the normal balance of the community. The release of kinetic energy from the hazard may change from zero to massive (ie, an earthquake), or may be too much (ie, nuclear power plant) or too little (ie, nuclear power plant). Events may be caused by natural or human-made hazards, or by a combination of the two (Table I-1). For example, a severe rainstorm (an event related to a natural hazard) may cause mudslides as a result of deforestation (a human-made hazard).
The use of the term event commonly is confused in disaster reporting; frequently and erroneously, the event is referred to as the disaster. However, an event is not a disaster, and it may or may not cause a disaster. Identifying the event or events that resulted in a disaster is essential in order to make comparisons between events and to discern those commonalities and differences that may exist as well as those events that do not result in a disaster. Events are compared by their respective characteristics and the settings in which they occur. Events may be primary or secondary. Secondary events may be responsible for more damage than the primary event (ie, earthquake causing a tsunami).
The probability (likelihood) that any hazard will become an event may be reduced through human actions to modify the risks associated with that hazard. Risk modification may reduce the probability that a hazard will cause an event or may modify the power of the event to a lower level. While risk modification to reduce the probability of an event related to a hazard is possible for the anthropogenic hazards, few natural hazards are amenable to modifying their likelihood for occurrence. However, the consequences of an event caused by a natural hazard often can be modified by human actions (interventions).
Structural Damage
Structural Damage is the harm or injury an event causes to any structures, both living and manmade, and/or the environment. Structural Damage results in decreases in the quantity and/or quality of the goods and/or services and/or resources available to the community. Goods, services, and resources are the elements required for the provision of functions for the population. Structural damage impairs the value or usefulness of something; it is a negative consequence(s) of the changes in the amount/rate of energy released from the hazard. 3 (pp56–68) The resultant damage is related to the transfer of the kinetic energy of the event into the structure exposed to the energy, and the type of energy contained in the event. The physical collapse of buildings or bridges, or the injuries sustained by victims of an event, are examples of Structural Damage. Some damage to structures may be reparable and some irreparable. Just as not all hazards cause an event, not all events cause structural damage. And as with an event, the occurrence of structural damage does not necessarily result in a disaster.
The likelihood that an event will cause damage depends on the natural vulnerability (ie, the vulnerability determined by nature), as well as the vulnerability of the community and the individual. 3 In order for damage to result from an event, the structure must be exposed to the energy (change in energy) of the event. If an event occurs, but no one is exposed to the energy of the event, no injuries will result. The likelihood that an event will result in structural damage is determined not only by the amount and type of energy released by the event and exposure to the energy released by the event, but, also, by the capacity of the affected community (its environment, living beings, structures, goods and services, and financial system) to absorb some or all of the energy released. This is referred to as the Absorbing Capacity 3 (p35) and may be modified (increased or decreased) by human actions (Figure I-2). For example, constructing buildings with quake-resistant materials increases the Absorbing Capacity for the energy released by an earthquake, while deforestation may decrease the Absorbing Capacity for the energy released by heavy rains.

Figure I-2 Conceptual Framework with Responses, Capacities, and Resilience Added. Responses may supplement levels of function and/or repair or replace damaged structures. Abbreviations: Ex, extraordinary; Or, ordinary.
Structural damage (compromised available supplies of goods, services, and/or resources) also may result from failure to provide sufficient supplies of energy for those community functions that require the use of energy from hazards. Failure to provide sufficient supplies of electricity may cause the failure of pumps to provide water for the cooling of a nuclear reactor which in turn, may cause further losses of electrical power to the community or even a nuclear meltdown.
Functional Damage (Decreases in Levels of Functions)
The damage to some structure or the environment that results from an event may impair the functions (functional integrity) of living or human-made structures (Functional Damage). The resultant functional damage may be a decrease in the level(s) of function(s), or a total loss of function. For example, a broken pipe (Structural Damage) may lead to a reduction or loss of water supply (Functional Damage), causing some of the functions of the organizational structure of the community to be diminished or unavailable. Or, the collapse of a bridge (Structural Damage) may lead to the loss, at least temporarily, of the transportation of people, goods, and services; it alters the functionality of the community (Functional Damage).
Not all Structural Damage caused by an event leads to Functional Damage. For example, if a storm causes a loss of electrical power to a hospital, but a back-up generator provides needed electrical power, no loss/decrease of the hospital’s functions occurs. If no decreases or losses in essential functions occur, no disaster occurs.
The probability (likelihood) that a decrease or loss of function will result from the Structural Damage (compromised available supplies of goods, services, and/or resources) caused by an event is determined by the structures damaged, the extent of the structural damage, and the ability of the affected community (or Systems within the community) to cope with that structural damage and to continue to function despite a change in available resources. This ability to continue to function is termed the Buffering Capacity 3 (p35) of the community (or individual) and can be modified (increased or decreased) by human actions (Figure I-2). For example, the stockpiling of drugs and medical supplies increases the Buffering Capacity for the structural damage caused by an epidemic, while locating back-up generators in the basement of hospitals decreases the Buffering Capacity for the structural damage resulting from flooding. The stockpiling of drugs may allow the health care system to continue to function during an epidemic, while generators placed in the basement of the hospital are likely to be damaged by flooding, and thereby render the hospital only partially functional, or completely non-functional. The functional damage that occurs depends on the ability of the affected community and its components to cope with the structural damage (loss of goods, services, and/or resources) and/or functional damage due to other causes.
Needs
A compromise of the functional status of any Societal System of a community, or its components, generates needs. Needs are the differences between the available goods, services, infrastructure, and other resources and those required to either stop or slow further losses of function, fill the gaps in the essential functions of the community, or to return an essential function to its pre-event level. Identifying the needs requires converting the degradation in level(s) of function (functional deficit) to the goods, services, resources, and infrastructure needed to maintain or restore levels of function. This conversion involves the synthesis of many assessments and requires substantial expertise and experience. Often, the conversion is based, in part, on assumptions. 4 Therefore, it is possible that this conversion may not yield an accurate determination of actual needs. Inaccurate/inappropriate synthesis of the data from assessments (lack of validity) can lead to undesirable consequences for the affected community and its component Systems, for the responders, and/or for the donors.
In some circumstances, needs may be anticipated from the characteristics of the event and the structural damage likely to occur. Anticipated needs are based on the experience(s) of those synthesizing the data from the assessments. The identification of needs is an ongoing process as more information becomes available and is integrated into the current Strategic Plan.
Responses
Responses are interventions/actions undertaken to meet the relief or recovery needs that resulted from an event. As noted above, needs are expressed as the goods and services and resources required to sustain the levels of function (relief) or to contribute to recovery.Reference Birnbaum, O’Rourke and Daily 5 - Reference Birnbaum, O’Rourke and Daily 7 The objective of each response must be related to a specific identified need or set of needs (Figure I-2) and every response (intervention) must have a stated overarching goal to which the response is contributing. Within the context of the defined goal, the most appropriate, and hopefully, the most efficient intervention is selected, providers are identified, and the selected response is implemented according to an Operational Plan. In general, responses are directed either to correcting the functional damage, supplementing levels of function, and/or repairing/replacing the damaged structure.
Responses to needs consist of three categories: (1) ordinary; (2) extra-ordinary; and (3) outside. Ordinary responses comprise of the routine, day-to-day responses to needs that do not require use of reserve goods, services, and other resources; examples include day-to-day interventions by prehospital Emergency Medical Services (if appropriate), emergency department services, elective and routine surgeries, law enforcement, clinic visits, and equipment maintenance. When the needs cannot be met by ordinary responses, extra-ordinary responses are recruited. Extraordinary responses include the use of additional of backup equipment, supplemental supplies and personnel, augmented services, and more, all of which normally are kept in reserve for special circumstances. When the needs cannot be met by ordinary responses and extra-ordinary responses are required, an “emergency” exists for the area directly affected. Both ordinary and extra-ordinary responses use local resources. Extraordinary responses utilize the community’s local response capacity: no resources from outside of the area directly affected are required to meet the defined need(s).
Response Capacities
The response capacity is the ability to respond or intervene to meet needs and prevent further deterioration of function(s) of a community or components of a community impacted by an event. Response Capacity often is referred to as “preparedness.” Such responses require goods, services, and/or other resources that are contained in the local response capacity; the local response capacity is the ability of the systems within the impacted area to meet the needs of the impacted population within that area. Each community has a capability to respond to day-to-day needs of the population without having to mobilize reserve goods and services. Needs that require resources that are in excess of those used for the provision of daily functions are extra-ordinary, and these reserves also are part of the Local Response Capacity.
Outside response capacity consists of the ability of the system(s) outside of the area directly impacted by an event to respond or intervene to help meet the needs of an affected population. Any response capacity from higher in the hierarchical level than the community affected by the event is considered to be part of the Outside Response Capacity. Both Local and Outside Response Capacities can be augmented by human actions. 4 , Reference Birnbaum, O’Rourke, Daily and Loretti 6
Emergency
When the community or any of its component systems requires the use of extraordinary goods, services, and other resources within its Local Response Capacity to meet the needs that result from the changes in functions (Functional Damage) to one or more of its components, the situation is an “Emergency” for that System in the community; in other words, even though extraordinary, the Local Response Capacity is sufficient to meet the needs of the affected community or the part(s) of the community that is(are) compromised (have a functional deficit), and no outside assistance (use of the Outside Response Capacity) is required.Reference Birnbaum, O’Rourke and Daily 7
Disaster
When needs cannot be met through use of resources within the local response capacity, a “disaster” has occurred for that community or element of the community; outside resources/responses are required to help meet the needs. Therefore, a disaster occurs for a community, or a part of a community, any time the needs exceed the Local Response Capacity of the community or components of the community.Reference Birnbaum, O’Rourke and Daily 7 A disaster always requires outside assistance to meet the needs, whether that outside assistance comes from a neighboring community, county, state, province, territory, or country. The affected community’s ability to cope with or manage the functional deficits that resulted from the damages caused by an event will determine whether or not a disaster occurs. The Outside Response Capacity is used to supplement the Local Response Capacity (ie, fill gaps in essential functions).
The probability that Functional Damage from an event will result in a disaster is determined by: (1) the extent of the functional damage; (2) whether or not an essential function is compromised or completely lost; and (3) the capacity of the Local Response System. If the Local Response System is able to manage the Functional Damage (ie, meet the needs), and to eventually restore any loss of an essential function using available local resources, a disaster for that community (or part of the community) does not occur. If a disaster has occurred and outside assistance that was provided is no longer required, a disaster for that system in the community no longer is present, although an emergency still may be present (reserve supplies are required).
The overwhelming change(s) in levels of function(s) that cause a disaster in one community may be manageable by local responses in another community and not result in a disaster. Disasters occur at the local community level.Reference Birnbaum, O’Rourke and Daily 8 The disaster is over for the community (or its component Systems) when the levels of essential functions can be sustained using only the local response capacity.
Resilience and Vulnerability
Resilience is the ability to recover quickly from illness, change, or misfortune; the property of a material that enables it to resume its original shape or position after being bent, stretched, or compressed; elasticity;Reference Birnbaum, O’Rourke and Daily 8 , 9 the ability of a system, community, or society exposed to hazards to resist, absorb, accommodate to, and recover from the effects of a hazard in a timely and efficient manner.Reference Pickett 10 In terms of a disaster or an emergency, resilience is comprised of the Absorbing, Buffering, and Response Capacities of a community to an event (Figure I-2). The resilience of a community may be modified by human actions or by changes in the environment caused by events from natural or anthropogenic hazards. Resilience increases as the Absorbing and/or Buffering and/or Response Capacities is/are increased.
On the other hand, vulnerability is the degree to which people, property, resources, systems, and cultural, economical, environmental, and social activity are susceptible to harm, degradation, or destruction on being exposed to a hostile agent or factor; 11 a capacity leading to a higher risk due to the combined effect of susceptibility and differences in exposure to a given hazard. Vulnerability decreases as the Absorbing, Buffering, and Response Capacities are increased. Capacity-building activities decrease the vulnerability to an event related to a hazard.
The Temporal Framework 12
The elements of the Conceptual Framework can be related longitudinally against time (Figure I-3). Each occurrence has a temporal component with a beginning and an end. The phases of a disaster are plotted in the order of their appearance in time, even though some of them may occur concurrently. For the purposes of studying disasters, and for interpreting, understanding, and comparing the findings of such studies, it is imperative to distinguish each of the phases of a disaster. These phases are identified by their characteristics rather than by an absolute time, and they include the: (1) Pre-event; (2) Event; (3) Structural Damage; (4) Functional Damage; (5) Relief; and (6) Recovery Phases. Responses are interventions designed to meet one or more needs. The Relief Phase includes interventions to fill the gaps in provision of essential or critical functions related to the damages sustained, and/or stopping or mitigating further damage from the precipitating (primary) event or subsequent, secondary events. The Recovery Phase includes those interventions that are not directed towards lifesaving or relief efforts, but, rather, towards restoring the community’s functional systems to their pre-event state. When the needs of a System or the components of the community can be met using only resources from within the community, the disaster for that System is over. However, the emergency persists until the pre-event status has been restored. Capacity-building and risk-reduction interventions that improve the functional status of one or more of the Societal Systems to a level higher than it was before the event are part of development, as they improve the community’s ability to withstand a future event; they do not constitute a temporal phase of a disaster.

Figure I-3 Temporal Framework Depicting the Phases of a Disaster from the Pre-Event State through Recovery. The phases usually overlap, and some run concurrently.
The Societal FrameworkReference Birnbaum, O’Rourke and Daily 7
The structural and functional damages and the disaster that occur during or following an event are relevant only in terms of their impact on a community’s population, constructions, functions, or environment. In order to study and compare the effects of an event on the complex amalgam that constitutes a community, the essential functional systems of a community have been deconstructed into 13 basic systems and their respective components (Figure I-4),Reference Birnbaum, O’Rourke and Daily 7 in much the same way that the human body is organized by functional organ systems for purposes of clinical assessment. The Systems are linked through a 14th System that coordinates and controls the activities of each of the component systems (Coordination and Control). The functional Systems that comprise any community are generic and exist in some form in all societies, and are called the Societal Systems. Each of the Societal Systems provides multiple functions and is comprised of subsystems, units, subunits, and so on. The Societal Systems and/or their component subsystems may be dependent upon one or more functions of other Systems to provide their products. For example, the Medical Care System depends on the Education System for the education and training of health care personnel, and the Logistics and Transportation System for the delivery of patients, staff, and supplies; and all of the Systems are dependent on the Energy Supply System.

Figure I-4 The Societal Framework. A community deconstructed into 13 component functional Systems linked together by a Coordination and Control function.
The organization of the Societal Systems is similar to the organization of the Clusters defined by the United Nations Inter-Agency Standing Committee (Geneva, Switzerland).Reference Birnbaum, O’Rourke and Daily 13 However, for the purposes of analysis and research, it is necessary to assign specific functions into only one Societal System.
A disaster is a manifestation of the needs created in one or more of the Societal Systems that requires assistance from outside to supply the needed goods, services, and resources, or to restore the System affected by the event(s). The magnitude of functional damage to the affected community from an event is dependent, in part, on the number of Societal Systems affected. In general, the more Systems that are damaged and lose function(s), the greater the need for outside assistance, and hence, the greater the scale of the disaster. It must be recognized that the levels of function of a given Societal System may be compromised due to functional damage in a Societal System upon which it is dependent. Recovery is complete for the Societal System being studied when the pre-event levels of essential functions have been restored and can be sustained without outside assistance.
Assessments of functional status transect the Temporal Phases at specified points in time. Assessments of function involve utilizing the indicators of function of each Societal System being studied. Each System has specific indicators that reflect its functionality. The functional status of one or more of the Societal Systems can be assessed at any specified time. In this way, one or more Systems can be studied for each event using the same indicators of function for each assessment. This allows evaluations to be repeated and the findings to be compared between evaluations, between communities, and between disasters.
Types of Research and Evaluations
Disaster research is composed of two basic types: (1) Epidemiological (non-interventional); and (2) Interventional. Epidemiology is the study of the incidence and distribution of diseases and other factors related to health; 14 the science concerned with the study of factors determining and influencing the frequency and distribution of disease, injury, and other health-related events and their causes in a defined human population for the purpose of establishing programs to prevent and control their development and spread; the sum of knowledge gained in such a study.Reference Thompson 15 Thus, epidemiological disaster research focuses on the components of a disaster in order to define the causes of the disaster and the progression from a hazard to a disaster, and to develop methods to mitigate or prevent them.
Interventions are action(s) by humans to prevent, attenuate, create, or enhance change; 3 (p35) to evaluate means to assess or appraise.Reference Pickett 16 In the context of Disaster Health, evaluation is an assessment of the effects, costs, outcomes, impacts, benefits, efficiencies, effectiveness, and efficacy of interventions provided during any phase of a disaster (ie, Relief or Recovery phases, or Pre-event (development)). Disaster interventions consist of actions aimed at relief, recovery, risk reduction, or capacity building. The evaluation of such interventions constitutes interventional disaster research.
Unfortunately, due to the paucity and non-uniform structure of reports of disaster interventions, little is known about the effects, costs, outcomes, impacts, benefits, effectiveness, efficacy, efficiency of, and the processes used by interventions provided before, during, and after disasters. Thus, it has not been possible to identify which interventions resulted in benefit(s) to the community affected or at-risk. However, this knowledge is essential for the codification of standards and best practices.
Epidemiological Disaster Research
Thus far, epidemiological research has been the most common form of disaster research used for the study and understanding of the health aspects of disasters.Reference Guralnik and Friend 17 It consists primarily of case, situational, progress, and final reports and summaries. Unfortunately, most of the reports are widely dispersed in the scientific, peer-reviewed literature,Reference Guralnik and Friend 2 and much has been published in the grey literature (non-peer reviewed, non-scientific literature).Reference Adibhattia, Dudek, Ramsel and Birnbaum 18 Currently, the most accessible repository for disaster epidemiological reports (not specific for health aspects) is maintained by the Center for Research on the Epidemiology of Disasters (CRED) at Louvain University in Brussels.Reference Smith, Wasiak, Sen, Archer and Burkle 19
The three Frameworks that are proposed to be used for the documentation and study of the epidemiology of disasters are the: (1) Conceptual; (2) Temporal; and (3) Societal Frameworks. The study of the outcomes, impacts, and benefits of specific interventions are not included in epidemiological research.
The Conceptual Framework in Epidemiological Research (What Happened, Why, and How?)
The Conceptual Framework 20 provides uniform terminology and a structure for reporting disaster epidemiological information. The use of standard definitions is essential to analyze and synthesize information from such studies, and develop the scientific base of Disaster Health. The Conceptual Framework tracks the progression from the existence of a hazard to the development of a disaster, and should facilitate an understanding of a disaster. The Conceptual Framework should be used in writing and publishing all disaster studies and reports related to the epidemiology of disasters, including case studies, situation, progress, after-action, and final reports and summaries. 20 Using the Conceptual Framework allows the synthesis of information from the same disaster, from similar disasters, and even the integration of information between dissimilar disasters, as well as for comparing events that resulted in a disaster to those similar events that did not.Reference Birnbaum, O’Rourke and Daily 21
The Temporal Framework 12 in Epidemiological Research (When?)
The Temporal Framework provides the structure required for describing the phases of a disaster. The phases are not time-bound (time of onset, duration), are not strictly consecutive (they may overlap), and relate to the properties that characterize each of the phases. When reporting a case study or in reports, summaries, and research, the specific phase of a disaster being discussed is included.
The Societal FrameworkReference Birnbaum, O’Rourke and Daily 7 in Epidemiological Research (Who?)
The Societal Framework is used to define the functional status of a Societal System or component at a particular time during one of the Temporal Phases of a disaster. Use of the Societal Framework facilitates the description of the Systems or components of the affected community or a community-at-risk, and the comparison of disasters/emergencies. Each of the Societal Systems has specific functional responsibilities. As noted, a disaster occurs when an event directly or indirectly causes one or more of the Societal Systems to reduce or cease its operation(s) (decrease in levels of functions), and outside help is required to fill the gaps in level(s) of function(s). Studying and/or reporting the functional damage sustained from an event cannot be done of the community as a whole, but, rather, must be focused on one or two of its essential Systems.
The Conceptual, Temporal, and Societal Frameworks provide the structure for systematically describing and understanding the epidemiology of disasters. The use of these three Frameworks should be required for all reports that describe or influence disaster epidemiology.Reference Birnbaum, O’Rourke and Daily 21 Without the use of such structure, the case studies and reports of the health effects of a disaster will remain elusive, and will continue to prevent the synthesis of available information into meaningful science that can be used for selection and implementation of interventions designed for risk-reduction and for education and training. Detailed descriptions of each of these Frameworks are provided in subsequent papers in this series.Reference Birnbaum, O’Rourke and Daily 7 , 12 , 20
Interventional Disaster Research
Interventional research involves the evaluation of disaster-related interventions whether they are directed at relief, recovery, hazard mitigation, capacity building, or performance. Evaluations are used to determine the value of an intervention and for comparisons. Although the goals and objectives differ, the processes used to evaluate interventions provided before, during, or after a disaster are quite similar. Interventional disaster evaluations incorporate the use of the Conceptual, 20 Temporal, 12 and SocietalReference Birnbaum, O’Rourke and Daily 7 Frameworks, as well as the DLM, 4 and the Relief/RecoveryReference Birnbaum, O’Rourke and Daily 5 and Risk-Reduction Frameworks.Reference Birnbaum, O’Rourke, Daily and Loretti 6
The Disaster Logic Model
A logic model is a graphic representation of a program [project] that depicts the intended relationships between investments and results. A logic model is a framework for describing relationships between investment, activities, and results.Reference Kulling, Birnbaum, Murray and Rockenschaub 22 Since the 1970s, logic models have been used for quality management and planning by private, public, and non-profit organizations in the domestic and international arenas (including by some donors). 23 - 26
Logic models are derivations of production functions as used in engineering. 27 Logic models are used to describe a program and its theory of change: “A theory of change is a description of how and why a set of activities—be they part of a highly focused program or a comprehensive initiative—are expected to lead to early, intermediate, and long-term outcomes over a specified period.” 23 The use of logic models helps to match evaluations to the interventions, define what should be assessed, and to focus on key information, including prioritization and what really must be known and why. Therefore, logic models are useful for planning, implementing, evaluating, comparing, and communicating projects or interventions.
The University of Wisconsin-Extension (UWEx; Wausau, Wisconsin USA) has promulgated a logic model for the design and evaluation of educational programs. 23 - 26 This logic model defines logical relationships between inputs, outputs (activities and participation), outcomes, and impacts over the short-, medium-, and long-term. A logic model provided by the Kellogg Foundation (Battle Creek, Michigan USA) separates the components of the logic model into resources and inputs, activities, outputs, outcomes, and impacts. 26
However, none of the logic models identified is precisely applicable to the evaluation of interventions provided before, during, or following disasters. All disaster-related interventions seek to change the current functional status of a community affected by or at-risk for a catastrophic event. Thus, the outputs or the effects from the transformation process should be a change(s) in the functional status of the community or one or more of its component Systems.
The existing logic models do not require the definition of the goals or objectives of the interventions, nor do they relate the needs, outputs, outcomes, and impacts to the goals and objectives. Therefore, for use in the study of disasters, the logic model has been revised to include relating: (1) the goals and objectives with the needs; (2) the effects of the intervention to the goal and objectives for which the intervention was selected; (3) the outcomes to the objectives of the intervention; and (4) the impacts to the overarching goal of the interventions (value). Separating the outcomes from the impacts is essential for the evaluation of a disaster intervention; it is possible that the objectives of an intervention may be achieved, but the project may not have contributed to attaining the stated goal. This iteration of the logic model is termed the “Disaster Logic Model” and is illustrated in Figure I-5.
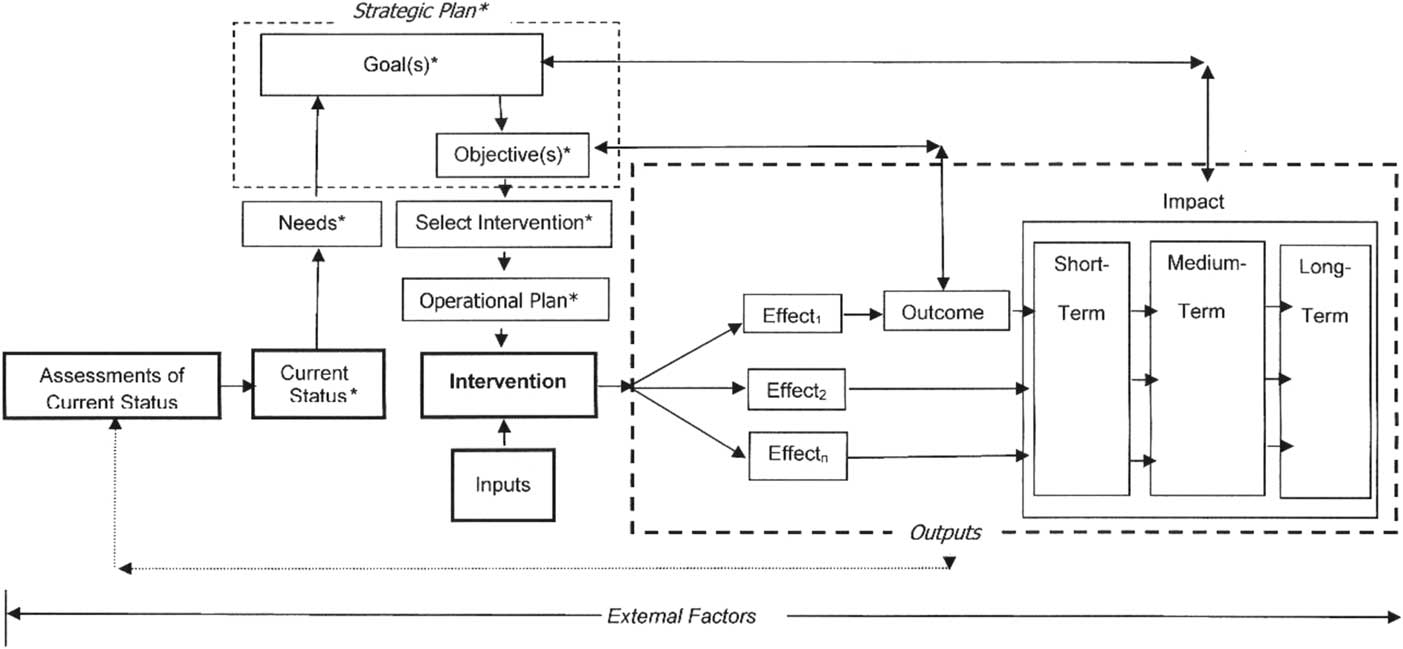
Figure I-5 The Disaster Logic Model Describing the Transformation Process Involved in All Disaster Interventions. The Needs, Goals, Objectives, and Selected Intervention include assumptions. The Intervention is a transformation process that produces a change(s) in the pre-intervention functional status. Inputs include all resources consumed by the transformation process (supplies, equipment, personnel time, opportunity costs, and more). The Outcome(s) relate to the objectives established for the intervention, while the short-, medium-, and long-term Impacts relate to the overarching Goal established in the Strategic Planning Process. Each of the steps in the process may be influenced by factors that are external to the transformation process. The Effects, Outcome(s), and Impact(s) all are based on assessments. *Contain assumptions from synthesis of information from preceding step.
Use of the DLM provides the needed structure for the evaluation of any intervention or project. It can be used to identify the effects (outputs), the outcome(s) (effects related to the objective(s) of the intervention), impacts and benefits (effects of the intervention) on the targeted population or the population-at-risk, and the resources (human, materials, financial, environmental, and opportunity costs) consumed by the transformation process. Cost:benefits, cost:effectiveness, needs:effectiveness, and efficiency in achieving the objectives can be derived and can be compared with those from other interventions provided by the same or different providers.
The Relief/Recovery Framework in Interventional Disaster ResearchReference Birnbaum, O’Rourke and Daily 5
Once an event has occurred and caused damage, human actions (interventions) are undertaken to prevent further losses of function, fill gaps that exist in levels of essential functions (Relief), and/or to restore the levels of essential functions back to their respective pre-event state (Recovery). The need for a specific intervention is determined by synthesizing the data/information obtained from assessments, and a Strategic Plan is developed to meet these needs. Interventions are selected, an Operational Plan is developed, and the intervention is implemented with the intent of satisfying (at least in part) the need(s) for which it is intended. Following implementation, all interventions must be evaluated for their effects, costs, outcomes, benefits/impacts to the affected community, effectiveness, efficacy, efficiency, cost:effectiveness, needs:effectiveness, and cost:benefit.
The Relief/Recovery Framework (Figure I-6) is based on the DLM 4 and provides the structure necessary to systematically evaluate the processes used in providing specific interventions during the Relief or Recovery Phases of a disaster. The Framework consists of a series of production functions (transformations) 27 that set the current status for the next step in the series (Figure I-6). Use of the Relief/Recovery Framework not only facilitates the identification of the effects of a specific intervention, but also its outcomes as related to the objectives of the intervention and its contribution towards achieving the overall goal. The Relief/Recovery Framework allows the dissection of the multiple processes that are involved in identifying the needs and selecting and implementing each intervention. Analyzing these processes facilitates comparisons in order to identify those interventions most successful in achieving the objectives and contributing most to the strategic goal with the greatest efficiency and least number and lowest severity of undesirable effects. This information is necessary to build an evidence-based repository of effective disaster-related interventions.

Figure I-6 The Relief/Recovery Framework. Framework is on the right and the processes used to move between the steps of the Framework are in italics on the left of the Framework. Abbreviations: DLM, Disaster Logic Model; LOF, level of function.
The Relief/Recovery Framework is utilized to evaluate the interventions/responses provided during a disaster and/or to evaluate the underlying processes. It is quite possible that the reason a particular intervention did not have the anticipated positive outcome is related to a failure in process (eg, insufficient funding or inappropriate needs identification) rather than to the specific intervention. Each of the processes of the Relief/Recovery Framework should be identified in reports of every disaster Relief/Recovery intervention.
The structure provided by the Relief/Recovery Framework and the DLM should facilitate the future development of useful interventions, demonstrate the worth of the project to the beneficiaries and sponsors, and build the evidence to support best practices for use for future events and for education and training.
Risk, Risk Reduction, Risk Management, and Capacity Building
The risk, or likelihood, of a disaster is a continuum/cascade of risks from a hazard to an event, to structural damage, to functional damages that create needs, to the local response capacity to meet those needs. Each step in this cascade of risks can be characterized by its probability of occurrence, and the probability of consequences of its occurrence; each risk is dependent upon the preceding occurrence in the progression of a hazard to a disaster (Figure I-7). A consequence of each risk in the cascade is the next occurrence in the Conceptual Framework; for example, the risk that: (1) the hazard will produce an event; (2) the event will produce structural damage; (3) the structural damage will result in functional damage; and (4) the needs created by the functional damage will exceed the local response capacity and result in a disaster for the community or one or more of its Systems. Risk-reduction measures can be directed at any point along this continuum. Interventions may be implemented to: (1) decrease the risk that a hazard will become manifest as an event; (2) decrease the amounts, types, and significance of structural and functional damages that will result from an event; and/or (3) increase the ability to respond to the needs that result from an event. Capacity building increases resilience by augmenting the absorbing, and/or buffering, and/or response capacities of a population-at-risk, and thereby decreases the risk that an event will result in a disaster. These risks holds true for both primary and secondary events.
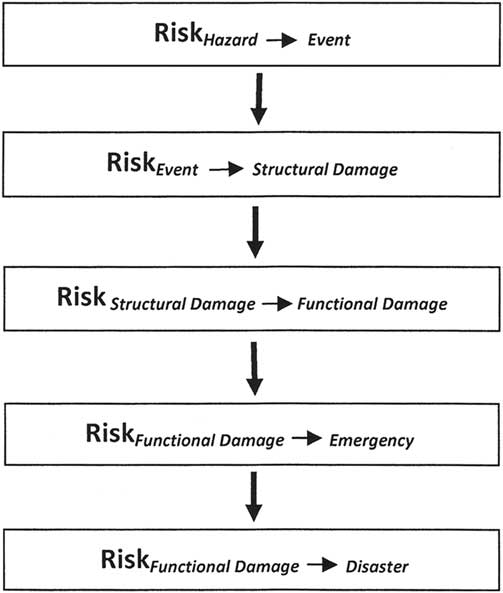
Figure I-7 The Risk Cascade Denoting the Risks for Each Step in the Conceptual Framework.
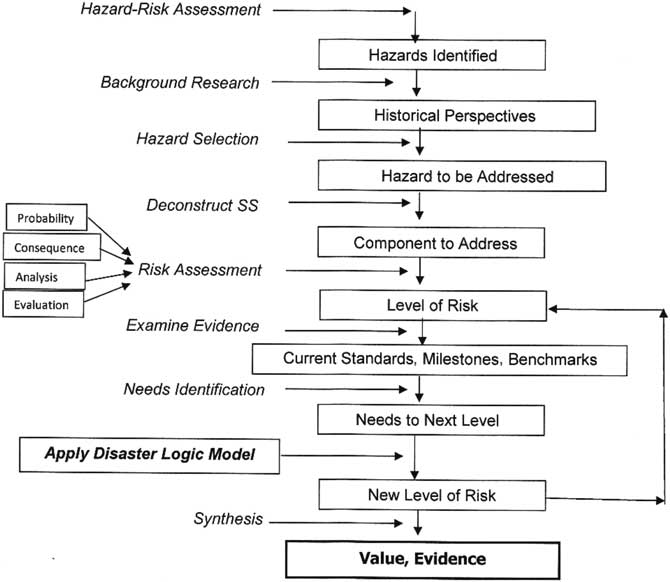
Figure I-8 The Risk-Reduction Framework. Framework is on the right and the processes used to move between the steps of the framework are in italics on the left. The processes/actions applied between the Needs to move on to the next level of Risk are identical to those used in the Relief/Recovery Framework and are based on the Disaster Logic Model. Abbreviation: SS, Societal System.
Most risk-reduction interventions are indirect interventions in that their impact on a disaster cannot be measured directly. For example, it is not possible to measure the impact of most disaster education and training programs on a specific disaster.
The Risk-Reduction Framework in Interventional Disaster ResearchReference Birnbaum, O’Rourke, Daily and Loretti 6
A disaster is a failure of resilience. Implementing measures to mitigate the destructive capabilities of a hazard and/or increase the resilience of a “community” (family, neighborhood, province/state, country, or region)-at-risk requires careful analysis, planning, and execution. The value (outcomes, costs, impacts, and benefits) of risk-reduction interventions is determined by applying the DLM and the Risk-Reduction Framework.
The Risk-Reduction Framework (Figure I-8) details the processes involved in: (1) mitigating the risk that a hazard will produce a destructive event and/or (2) building capacity to augment the resilience of a community to the consequences of an event. Capacity building includes all interventions directed towards increasing the absorbing, buffering, and/or response capacities of a community-at-risk for an event that could result in a disaster. The Risk-Reduction Framework consists of additional steps that precede those outlined in the Relief/Recovery Framework (Figure I-6). These additional elements include: (1) hazard and risk assessment; (2) historical perspectives and predictions of risks; (3) selection of hazard(s) to be addressed; (4) selection of Societal System and components to be addressed; (5) level of risk; (6) identification of current standards, milestones, and benchmarks; and (7) needs to progress to next level of function. These additional steps are required to define the needs for risk-reduction interventions. The ultimate goal of risk-reduction interventions is to develop an improved level of risk and evidence that will guide future interventions.
Evaluations of risk-reduction interventions, including the evaluation of the processes involved with the reduction of risks, allows the comparison of different risk-reduction interventions, as well as the identification of critical points of success and/or failure in the provision of the intervention being evaluated. However, determining the impact of risk-reduction interventions may not be possible until the next event occurs, or by comparing the impacts of similar interventions following similar events in similar or dissimilar settings.
Using the Disaster Research Frameworks
Although the five Frameworks provide a structure for evaluation and reporting of the health aspects related to a disaster, they may be adapted for use in studying other aspects of a disaster. Likewise, they can be used employing various research methodologies as well as in prospective and retrospective analyses.
Summary
Using structured Frameworks with clearly defined terminology facilitates the development of a sound body of evidence regarding the factors that influence the health status of a population affected by an event that led to a disaster. The Conceptual, Temporal, and Societal System Frameworks provide a standardized approach for use in the study of the health aspects related to a disaster. The use of the DLM allows the evaluation of the effects of any disaster-related intervention. Utilizing the Frameworks and the DLM permits comparisons of disasters and disaster-related interventions to be made between different communities, different interventions, and between different disasters.









