



Introduction
Ebola Virus Disease (EVD) is a serious, often fatal disease caused by the Ebolavirus, a virus of the Filoviridae family, capable of infecting multiple species of primates, including humans.Reference Feldmann and Geisbert1,Reference Schou and Hansen2 Due to its epidemiological presentation pattern, impact on public health, resources necessary for its management and control, as well as the need for a response from national and international organizations, the disease is considered a paradigm of international health emergency.3
The first known outbreak of EVD, hereafter Ebola, began in June 1976 in two small villages, Nzara and Maridi, in the southern regions of the current State of South Sudan and ended spontaneously at the end of November.4 Approximately one thousand kilometers away, and almost simultaneously, another outbreak of similar characteristics occurred in the small village of Yambuku, in the north of the former Zaire (now Democratic Republic of the Congo [DRC]).5 The biological samples sent to national and international laboratories allowed to identify a new genus of Filovirus that was called Ebola Virus, in reference to a river near Yambuku, a tributary of the Congo River.Reference Quammen6
Subsequently, Ebola again caused new outbreaks in both countries, and also in Sudan in 1979, and in the DRC in 1977, 1995, 2007, 2008, and 2014. The disease also appeared in Gabon (1994, 1996, and 2001); Ivory Coast (1994); South Africa (1996); Uganda (2000, 2007, 2011, and 2012); and in the Republic of Congo (2001, 2002, 2003, and 2005). During this time, the different sub-types of the genus Ebolavirus were identified,Reference Baron, McCormick and Zubeir7 and an unsuccessful attempt was made to identify the reservoir of the virus. New outbreak control protocols were also implemented and several aspects of epidemiological surveillance and cooperation of the authorities were improved.Reference Le Guenno, Formenty, Wyers, Gounon, Walker and Boesch8-Reference Nkoghe, Kone, Yada and Leroy40
In December 2013, in the small village of Meliandou, in a dense forest region of southern Guinea, the first cases of a new outbreak appeared. It took close to three months before the disease was identified as Ebola, and it had by that time spread through the country, including its capital Conakry and soon after also to the Sierra Leone and Liberia borderlands. When the World Health Organization (WHO; Geneva, Switzerland) declared the International Public Health Emergency,41 nine months after the start of the outbreak, Ebola was affecting numerous districts of both countries, including their capitals Monrovia and Freetown. This was an unprecedented situation.
From the cities of Guinea, Liberia, and Sierra Leone, the disease also risked to spread by land, sea, or air to many other regions of Africa and the world. In a few months, cases appeared in Mali, Nigeria, and Senegal, as well as in Spain, Italy, the United Kingdom, and the United States. Here, the transmission was stopped after a few cases and before any further transmission occurred.
As a consequence of the growing concern, many states and international organizations contributed economic and logistical resources to try to stop the advance of the outbreak. In addition, the intervention protocols were optimized and the number of clinical trials multiplied to find an effective pharmacological treatment. Control of what would be known as “The Great Outbreak of West Africa” was finally achieved in 2016, after almost 29,000 cases and more than 11,300 deaths.42
In 2017, Ebola appeared again in the DRC in the form of an outbreak that was controlled in two months. From April to June 2018, the country was again affected by the disease, and was tested in the field of the new approved rVsV-ZEBOV vaccine against Ebola disease.Reference Walldorf, Cloessner, Hyde, MacNeil and Emergency Ebola43 Just a few days after the official declaration of the end of this last outbreak, the DRC Ministry of Health notified the appearance of a series of new cases of hemorrhagic fever in the east of the country, in the conflict torn area of North Kivu. This was the beginning of the largest outbreak in DRC's history, with a vast geographical spread in North Kivu and also Ituri provinces, and occasional cases in neighboring Uganda, with a total of 1,945 cases and 1,302 deaths reported as of May 28, 2019.44
The objective of this work is to study the evolution and progression of the epidemiological presentation profile of Ebola disease outbreaks since its discovery in 1976 to the present, as well as to explore and discuss the potential reasons for this evolution from different perspectives (demographic, socioeconomic, or political changes in the affected countries).
Methods
Retrospective observational study of the 38 outbreaks of Ebola disease that occurred from 1976 through 2019, excluding laboratory accidents, was done. For the latest outbreak in DRC, the study includes information up until June 2019. The different organizations involved in response and surveillance have been used as sources of information, such as the United Nations agencies and programs (ie, WHO; United Nations Children's Fund [UNICEF; New York USA]; and United Nations High Commissioner for Refugees [UNHCR; Geneva, Switzerland]); Ministries of Health; US Centers for Disease Control and Prevention (CDC; Atlanta, Georgia USA); ReliefWeb (New York USA); emergency nongovernmental organizations such as Doctors Without Borders (Médecines Sans Frontières; Paris, France) and the International Red Cross (Geneva, Switzerland); as well as publications indexed in PubMed (National Center for Biotechnology Information, National Institutes of Health; Bethesda, Maryland USA), EmBase (Elsevier; Amsterdam, Netherlands), and Clinical Key (Elsevier; Amsterdam, Netherlands). The definition of Ebola case established by the WHO has been used.45 Inclusion criterion included cases that had been officially notified to WHO following the mentioned WHO case definition. Cases or suspicion of cases not formally notified were excluded. For each of the outbreaks, information on the variable year of the outbreak, date of beginning and end, duration of the outbreak in days, number of cases, number of deaths, population at risk, geographic extension affected in Km2, and time of notification of the first cases to WHO have been searched and analyzed.
Although different sources of information from field work organizations have been used and therefor the accuracy is variable, this was limited as only confirmed and officially notified cases have been used. A specific study database was developed and the reports were reviewed by two of the researchers to check for accuracy.
Absolute and relative numbers, incidence rates per 10,000 inhabitants, mortality rates per 10,000 inhabitants, as well as case fatality percentages have been used as frequency measures. In the statistical description, parameters of central tendency (mean, median); and dispersion (standard error of the mean, standard error of the median, standard deviation, range, Pearson coefficient of variation [CV]) have been used, as well as parameters of normality of the distributions (Fisher's asymmetry and kurtosis coefficients). Correlation analysis has also been used, and in the trend analysis, regression analysis with simple exponential smoothing has been used to control the data series of the variables with random patterns and to eliminate the effect of the historical irregular elements from the analysis. In all cases, differences with a probability of error of less than .05 have been considered significant.
Results
Table 1 shows the outbreaks and cases for each affected country in the 38 outbreaks of Ebola from 1976 through 2019. Although the DRC was the country in which more outbreaks have occurred, the greatest impact had been in Sierra Leone, which had suffered the highest absolute frequency of cases. A single outbreak in Sierra Leone, which occurred between 2013 and 2016, produced more cases (14,124; 43% of all cases in the historical series) than the 10 outbreaks of the DRC. A summary of the parameters of central tendency, dispersion, and normality characteristics (asymmetry and kurtosis) of the frequency distributions of the studied variables can be seen in Table 2.
Table 1. Number of Ebola Outbreaks and Cases per Affected Country, 1976-2019

Table 2. Epidemiological Parameters of the Ebola Outbreaks (n = 38), 1976-2019

Abbreviation: WHO, World Health Organization.
The average number of cases per outbreak in the 38 outbreaks was 861.3 (SD = 2860.7; CV = 3.3) with large differences between the different outbreaks. There were also significant differences in the average population exposed to risk in the different outbreaks (mean = 1,531,994.4; SD = 2,837,996.2; CV = 1.8) and in the average incidence rates (mean = 87.4; SD = 403.7; CV = 4.6). The average number of deaths per outbreak was very heterogeneous in the 38 outbreaks (mean = 359; SD = 1053.2; CV = 2.9), and so was the mortality rate (mean = 51.7; SD = 226.5; CV = 4.4). However, the case fatality of the outbreaks was more homogeneous (mean = 54.4%; SD = 28.6; CV = 0.5). The average duration of the outbreaks was heterogeneous (mean = 139.4 days; SD = 209.3; CV = 1.5), as well as the geographical extent of the outbreaks (average km2 = 31,892.7; SD = 63,290; CV = 2) and the average time to notify WHO (mean = 36.9 days; SD = 33.5; CV = 0.9).
The amount of population exposed to risk was directly and significantly correlated with the geographical extent of the outbreaks (P = .004), with their duration (P = .001), and with the number of deaths produced (P = .001). The duration and geographic extent of the outbreaks were also directly correlated (P = .001). The total cases were directly related to the population at risk (P = .001), with the extension (P = .04), and with the duration of the outbreaks (P = .001), as well as the incidence and mortality rates (P = .001). The number of deaths was directly correlated with the total number of cases (P = .0001), with the geographical extension (P = .006), and with the duration of the outbreak (P = .0001), but not with the incidence rate or with that of mortality.
Regarding temporal trends, although there was an increase in the number of cases per outbreak during the period studied, this increase was not significant. However, the population at risk increased significantly (P = .024; regression line: - 172.222.076 + 86.672 x Year) from 1976 to the present, as shown in Figure 1. Even though there have been small increases in the number of cases and the number of people who have died due to the disease, the incidence and mortality rates of outbreaks have reduced, although not significantly.

Figure 1. Trend in the Population Exposed to Risk to Ebola, 1976-2019.
The geographical extent of Ebola outbreaks has grown significantly (P = .004; area (Km2) = - 5,290,270.9 + 2,659.7 x Year), as shown in Figure 2, as well as its duration from 1976 to the present has also done, though not significantly. Figure 3 shows that the reporting time of the first cases of Ebola outbreaks to WHO has been significantly reduced (P = .017; days until notice = 2,507.6 - 1.2 x Year) and the case fatality of successive outbreaks in a significant way (P = .028; case fatality (%) = 1,743.5 - 0.84 x Year) that has gone from 88% to 62% in the period studied, as shown in Figure 4.
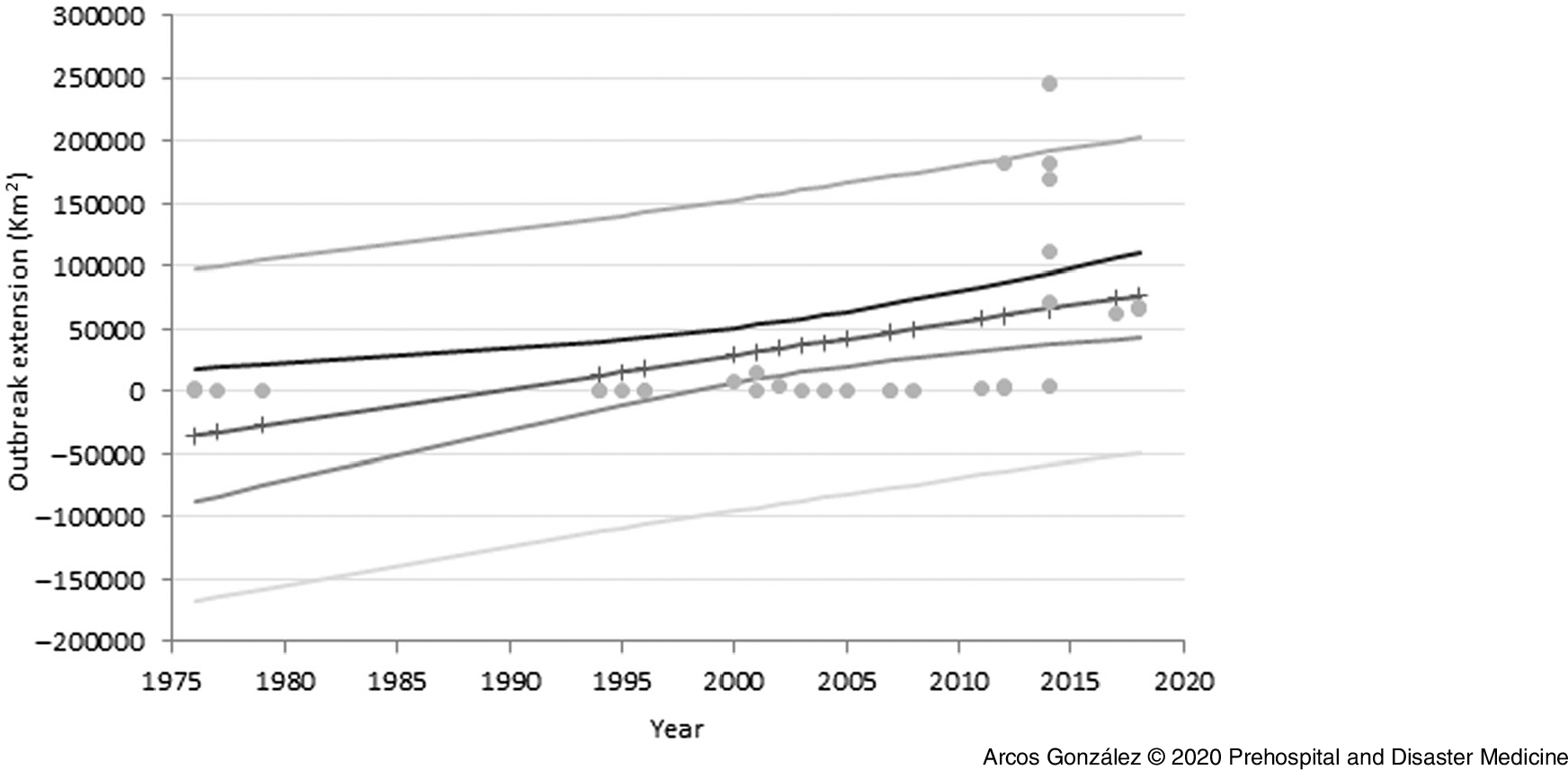
Figure 2. Trend in Geographical Extension of Ebola Outbreaks, 1976-2019.

Figure 3. Trend in Reporting Time of the First Cases of Ebola Outbreaks to WHO, 1976-2019.

Figure 4. Trend in the Case Fatality (%) of Ebola Outbreaks, 1976-2019.
There have been significant differences (P = .04) between the outbreaks produced by the Sudan and Zaire strains of the virus, both in terms of duration and case fatality ratio (Sudan strain 74.5 days on average and 62.7% of case fatality ratio versus Zaire strain with 150 days on average and 55.4% case fatality ratio).
Discussion
This study has found a change in the evolution of the epidemiological characteristics of the outbreaks of Ebola disease in the last 40 years. While recognizing the heterogeneity of the results, the trends point to an increase in the geographical spread, the duration, and the number of cases per outbreak, despite advances in outbreak surveillance and control. While the treatment protocols have been improved and experimental treatment is starting to show promising results, the case fatality in the most recent outbreaks seems to remain at the same level as in earlier outbreaks. Below are suggested explanations to the results.
It is a known phenomenon that regions subject to accelerated demographic, political, and socioeconomic changes undergo changes in the risk-profile of epidemic phenomena.Reference Farmer46,Reference O’Sullivan and Bourgoin47 This process has also occurred in parts of central and western Africa in the last decades.Reference Mertule48 The mainland region of the continent has the highest urban growth rates in the world (by 2050, more than one-half of the Central African population will live in cities), and the significant decline in crude mortality in Africa in the last 30 years has made it a region with unprecedented demographic potential.Reference Munster, Bausch and de Wit49
Urban growth and infrastructure construction show the economic development of the continent, while there is an important exploitation of natural resources, especially raw materials of high strategic and economic value such as tantalum, rubber, gold, or diamonds. The struggle for the control of the exploitation and trade of these goods, together with the corruption and political instability of countries such as the DRC, South Sudan, the Republic of the Congo, Rwanda, or Uganda has in recent decades led to an increase in intra- and international tensions and violence by local guerrillas and other armed groups.Reference Stearns50 This situation of insecurity and violence has generated enormous migrant flows with hundreds of thousands of displaced people who have had to abandon their households.51
On the other hand, deforestation and exploitation of virgin areas have caused human contact with ecosystems in which there are multiple species of animals that can act as reservoirs of pathogenic agents of communicable diseases,Reference Bauch, Birkenbach, Pattanayak and Sills52 as is the case of the Ebola virus. The situation is therefore complex and its economic development unstoppable. It seems reasonable to think that, in this context, the epidemiological profile of Ebola disease presentation also is undergoing changes.
First, the improvement of the infrastructure and communication routes of the countries implies an increase in the movement of people and also facilitates their access to large population centers in short periods of time. This could explain the progressive increase in the number of people at risk in the successive Ebola outbreaks since 1976, as well as their geographical extension. Until 2013, Ebola outbreaks have generally remained confined in small villages of difficult access, surrounded by dense tropical forests, with little population and a reduced risk of extension to large urban centers. However, from the great outbreak of West Africa from 2013 to 2016, the trend has changed. And, although the first cases continue to appear mostly in small villages or rural nuclei, their extension to populations of greater magnitude, including cities of more than one million inhabitants, is increasingly more likely, with the difficulties that this entails in terms of epidemiological containment.
Despite the significant increase in geographic extension and the population at risk, the outbreaks total number of cases and deaths have only suffered a slight upward trend. This could be explained by the important advances made in the management of outbreaks, which would partly offset a growing ease of spreading the virus.
Since 1976, the political interest, the economic and logistic resources available, and the cooperation and coordination of national and international health agencies have improved markedly. Increased awareness of State Authorities has been achieved, and rapid diagnostic methods and close contact monitoring have been optimized. A vaccine has been developed and put into practice, and several clinical trials have been carried out in order to find an effective pharmacological treatment.Reference Damon, Rollin, Choi, Arthur and Redfield53,Reference Jefferies, Rashid, Hill-Cawthorne and Kayser54 Various aspects of epidemiological surveillance in outbreaks have also been optimized, reducing the limited period of time between the appearance of the first cases and the notification of them to WHO. There has been a progressive reduction in the case fatality of Ebola outbreaks. Among the possible reasons for this reduction could be the adaptation of the virus to the human host.
However, despite all the progress made in these four decades, there are a number of factors that make it difficult to epidemiologically address Ebola outbreaks in those parts of Africa with extreme poverty, weakness of national health systems, lack of access to health services, war conflicts, struggle for control of trade in raw materials, and violence that promotes migration movements, in addition to other religious or cultural factors such as the tradition of cleaning and manipulating of deceased (which favors transmission of the virus). All of these circumstances make the control and management of Ebola outbreaks much more complex than those occurring outside the continent to date.
Limitations
This study covers a long period of time, a very large geographical area, and information collected comes from heterogeneous sources, which can constitute a limitation in terms of information bias. The most recent outbreak in eastern DRC is still on-going at the time of writing this article, hence the total number of infected and the geographical spread is not yet known.
Conclusions
There has been a change in the epidemiological profile of the Ebola outbreaks during the period from 1976 through 2019. This change in this epidemiological profile has mainly consisted of a significant increase in the geographical extent of the outbreaks and the population at risk, as well as a significant decrease in the outbreaks case fatality rate. There have been also very significant advances in the detection and management capacity of outbreaks, and the notification time to the WHO has been significantly reduced. However, there is sufficient evidence of the persistence of a series of social, economic, cultural, and political obstacles that continue to greatly hinder a more efficient epidemiological approach to Ebola disease, mainly in Central Africa.
Conflicts of interest
none






