



Conduct problems refer to a broad range of “acting out” behaviors, which vary considerably in terms of severity (e.g., temper tantrums vs. physical violence) and type (e.g., covert vs. overt; Kimonis, Frick, & McMahon, Reference Kimonis, Frick, McMahon, Mash and Barkley2014). As a result, youth who display conduct problems are highly heterogeneous with respect to their etiologies, clinical presentations, and prognoses, making subtyping an empirical and clinical necessity. One commonly used approach for subtyping youth with conduct problems is based on age of onset. This approach is rooted in Moffitt's (Reference Moffitt1993) developmental taxonomy theory, which proposes that there is a distinction between youth whose conduct problems emerge in childhood versus adolescence. Since its publication, considerable evidence has been found for the distinction between early-onset-persistent (EOP) and adolescence-onset (AO) conduct problems (Moffitt, Reference Moffitt2018). This research has highlighted the risk incurred by developing conduct problems in childhood (i.e., the continuation of antisocial behavior later into development). In addition to being formally incorporated into diagnostic criteria for conduct disorder (i.e., childhood- vs. adolescent-onset specifiers; American Psychiatric Association [APA], 2013), this distinction has inspired large-scale prevention and early intervention efforts to prevent the onset and development of conduct problems in childhood (e.g., Conduct Problems Prevention Research Group [CPPRG], 2019; Shaw, Dishion, Supplee, Gardener, & Arnds, Reference Shaw, Dishion, Supplee, Gardener and Arnds2006).
Even though early-onset conduct problems are an established risk factor for antisocial behavior in adolescence and adulthood (Jennings & Reingle, Reference Jennings and Reingle2012; Moffitt, Reference Moffitt2018; Moffitt et al., Reference Moffitt, Arseneault, Jaffee, Kim-Cohen, Koenen, Odgers and Viding2008), accumulating evidence suggests that not all “early starters” show persistent antisocial behavior. Indeed, a second pathway of early-starting conduct problems has been reported, often referred to as childhood-limited (CL), but also declining or desisting (see Fairchild, van Goozen, Calder, & Goodyer, Reference Fairchild, van Goozen, Calder and Goodyer2013; Moffitt et al., Reference Moffitt, Arseneault, Jaffee, Kim-Cohen, Koenen, Odgers and Viding2008). This pathway, characterized by childhood-onset conduct problems that steadily decline prior to adolescence, has been identified by multiple independent research groups in North American (e.g., Aguilar, Sroufe, Egeland, & Carlson, Reference Aguilar, Sroufe, Egeland and Carlson2000; Cote, Vaillancourt, LeBlanc, Nagin, & Tremblay, Reference Cote, Vaillancourt, LeBlanc, Nagin and Tremblay2006; Nagin & Tremblay, Reference Nagin and Tremblay1999; Shaw et al., Reference Shaw, Galan, Lemery-Chalfant, Dishion, Elam, Wilson and Gardner2019), European (e.g., Barker & Maughan, Reference Barker and Maughan2009; Reef, Diamontopoulou, van Meurs, Verhulst, & van der Ende, Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2010; Sentse, Kretschmer, de Haan, & Prinzie, Reference Sentse, Kretschmer, de Haan and Prinzie2017), New Zealand (e.g., Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008), and Australian (e.g., Bor, McGee, Hayatbakhsh, Dean, & Najman, Reference Bor, McGee, Hayatbakhsh, Dean and Najman2010) samples. With population-based studies showing that 50–70% of early starting children desist from acting antisocially before adolescence, it has been suggested that desistence is the most common outcome of childhood-onset conduct problems (Fairchild et al., Reference Fairchild, van Goozen, Calder and Goodyer2013).
From a developmental psychopathology perspective, these findings beg the question of what predicts early-onset conduct problem persistence versus decline. To date, only a small number of researchers have used formal statistical tests to directly compare characteristics of children who follow these different trajectories. So far, there is preliminary evidence that certain family and child characteristics may increase the likelihood that childhood conduct problems will persist (vs. decline). With respect to family factors, persistence has been linked to lower family income (Cote et al., Reference Cote, Vaillancourt, LeBlanc, Nagin and Tremblay2006; Maughan, Pickles, Rowe, Costello, & Angold, Reference Maughan, Pickles, Rowe, Costello and Angold2000; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007); higher levels of family stress (Kjeldsen, Janson, Stoolmiller, Torgersen, & Mathiesen, Reference Kjeldsen, Janson, Stoolmiller, Torgersen and Mathiesen2014); lower maternal education (Cote et al., Reference Cote, Vaillancourt, LeBlanc, Nagin and Tremblay2006; Nagin & Tremblay, Reference Nagin and Tremblay2001); lower maternal age (Kjeldsen et al., Reference Kjeldsen, Janson, Stoolmiller, Torgersen and Mathiesen2014; Nagin & Tremblay, Reference Nagin and Tremblay2001); maternal anxiety during pregnancy (Barker & Maughan, Reference Barker and Maughan2009); family histories of externalizing disorders (Odgers, Milne, et al., Reference Odgers, Milne, Caspi, Crump, Poulton and Moffitt2007); parental criminality (Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007); and exposure to domestic abuse (Barker & Maughan, Reference Barker and Maughan2009), and negative parenting practices (e.g., harsh parenting, poor supervision, maternal rejection; Barker & Maughan, Reference Barker and Maughan2009; Maughan et al., Reference Maughan, Pickles, Rowe, Costello and Angold2000; Shaw, Gilliom, Ingoldsby, & Nagin, Reference Shaw, Gilliom, Ingoldsby and Nagin2003). In terms of child characteristics, there is some evidence that children on the persisting pathway are significantly more likely to: be male (Cote et al., Reference Cote, Vaillancourt, LeBlanc, Nagin and Tremblay2006), have ADHD (Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007), and display more severe childhood conduct problems (Pitzer, Esser, Schmidt, & Laucht, Reference Pitzer, Esser, Schmidt and Laucht2009) and distinct temperamental characteristics like fearlessness (Shaw et al., Reference Shaw, Gilliom, Ingoldsby and Nagin2003) and a high activity level (Barker & Maughan, Reference Barker and Maughan2009).
Despite these promising findings, most of the identified predictors have not been replicated – and in some cases, inconsistent findings have emerged (e.g., regarding maternal depression; Kjeldsen et al., Reference Kjeldsen, Janson, Stoolmiller, Torgersen and Mathiesen2014; Shaw et al., Reference Shaw, Gilliom, Ingoldsby and Nagin2003). On a practical level, this means that there is currently no systematic, evidence-based way to reliably distinguish between children whose conduct problems are likely to persist versus decline for the purposes of diagnosis and treatment planning (Moffitt et al., Reference Moffitt, Arseneault, Jaffee, Kim-Cohen, Koenen, Odgers and Viding2008). Nevertheless, this may only pose a problem if children on the declining (or CL) pathway of conduct problems are not at risk for negative outcomes. That is, if children with persisting and declining conduct problems show similar problems later in development, similar interventions may be indicated for all early starters.
When used to describe conduct problem trajectories, the terms “childhood-limited” and “desisting” imply a certain degree of prognostic optimism. While it may be tempting to assume that these children adapt well because their conduct problems decline before adolescence, one could argue that displaying conduct problems at any point in childhood could potentially disrupt subsequent development. Developmental cascade theory (Masten & Cicchetti, Reference Masten and Cicchetti2010) posits that certain childhood events or experiences (e.g., the onset of psychopathology) have the potential to set a “snowball effect” in motion, whereby different levels of development are affected in complex ways over time. In line with this theory, research shows that early-onset conduct problems increase children's risk for poor adaptation during school years (e.g., academic failure, peer rejection), which further predicts poorer adjustment later in development (e.g., Dodge, Greenberg, Malone, & CPPRG, Reference Dodge, Greenberg and Malone2008; Moilanen, Shaw, & Maxwell, Reference Moilanen, Shaw and Maxwell2010). Furthermore, it is possible that CL individuals’ core psychopathology may not desist, but rather display heterotypic continuity (i.e., manifest differently throughout development; Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996). The concept of heterotypic continuity could explain why CL children's conduct problems decline over the course of childhood: Their clinical presentations may change as they approach the transition to adolescence. In either case, the implication would be that CL children are potentially at elevated risk for poorer outcomes – at least compared to peers who never display conduct problems. Therefore, the long-term adjustment of CL individuals is an empirical question that needs to be formally tested.
To date, only a small number studies have examined the long-term developmental outcomes of children who follow different pathways of childhood-onset conduct problems. Earlier studies primarily used cut-off scores to classify antisocial children/youth, which typically involves manually assigning conduct problem trajectory labels based on the severity of antisocial behavior at different time points (e.g., Aguilar et al., Reference Aguilar, Sroufe, Egeland and Carlson2000; Bor et al., Reference Bor, McGee, Hayatbakhsh, Dean and Najman2010; Hyatbakhsh et al., Reference Hyatbakhsh, McGee, Bor, Najman, Jomrozik and Mamun2008; Jennings, Rocque, Fox, Piquero, & Farrington, Reference Jennings, Rocque, Fox, Piquero and Farrington2016; Moffitt, Caspi, Harrington, & Milne, Reference Moffitt, Caspi, Harrington and Milne2002; Roisman, Aguilar, & Egeland, Reference Roisman, Aguilar and Egeland2004). However, the cut-off approach has been criticized for its overreliance on theoretically derived categorization rules to define different subgroups of youth (Nagin & Odgers, Reference Nagin and Odgers2010).
To address this limitation, more recent studies have used group-based modeling techniques such as latent class growth analysis (LCGA; Nagin, Reference Nagin1999) to examine the long-term outcomes of childhood conduct problem trajectories. To date, a wide range of long-term outcomes of childhood conduct problem trajectories have been examined using this person-centered method, including various indicators of psychopathology, antisocial behavior, physical health, public service utilization, and social functioning (e.g., Fontaine et al., Reference Fontaine, Carbonneau, Barker, Vitaro, Hebert, Cote and Tremblay2008; Heron et al., Reference Heron, Maughan, Dick, Kendler, Lewis, MacLeod and Hickman2013; Kjeldsen et al., Reference Kjeldsen, Janson, Stoolmiller, Torgersen and Mathiesen2014; Kretschmer et al., Reference Kretschmer, Hickman, Doerner, Emond, Lewis, MacLeod and Heron2014; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008; Rivenbark et al., Reference Rivenbark, Odgers, Caspi, Harrington, Hogan, Houts and Moffitt2018; Sentse et al., Reference Sentse, Kretschmer, de Haan and Prinzie2017). That said, much of the evidence is limited to adjustment in adolescence and emerging adulthood (i.e., ages 13 to 21). For example, in the UK-based AVON Longitudinal Study of Parents and Children, Kretschmer et al. (Reference Kretschmer, Hickman, Doerner, Emond, Lewis, MacLeod and Heron2014) examined associations between conduct problem trajectories (modeled from ages 4 to 13) and psychosocial outcomes at 18 years. They found that individuals on the CL pathway (12.1% of the sample) were less likely than their early-onset-persistent counterparts (9.2% of the sample) to report alcohol use, smoking, cannabis use, criminal involvement, and anxiety. Furthermore, after adjusting for potentially confounding factors, there were no significant differences between CL individuals and those on the Low trajectory (70.1%) at age 18. In contrast, in the Flemish Study on Parenting, Personality, and Development, Sentse et al. (Reference Sentse, Kretschmer, de Haan and Prinzie2017) found that, compared to individuals with Low conduct problems from ages 4 to 17 (48% of the sample), those on CL (12% of the sample) and LCP (25% of the sample) pathways were more likely to display aggression, rule-breaking behavior, withdrawn/depression symptoms, and thought problems by the time they were 17–20 years old. Notably, the LCP group also showed more attention problems and social problems than the Low group; however, the LCP and CL groups did not significantly differ on any of the outcomes examined. Although the findings from these two studies suggest that LCP individuals fare the worst by late adolescence, they paint contradictory developmental pictures of individuals who followed the CL pathway. Thus, more research is needed on long-term outcomes of childhood conduct problem trajectories – including studies that extend beyond adolescence and emerging adulthood.
To date, only a few studies have used group-based modeling to examine the predictive validity of childhood conduct problem trajectories beyond the age of 21 (e.g., Bongers, Koot, van der Ende, & Verhulst, Reference Bongers, Koot, van der Ende and Verhulst2008; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008; Reef et al., Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2010, Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2011). In the Dunedin birth cohort, Odgers and colleagues (Odgers, Caspi, et al, Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008) reported that individuals on the LCP pathway (10.5% males, 7.5% females) were faring the worst on most outcomes at age 32. Although CL males (24.3%) displayed more internalizing problems, violence, substance use, health problems, and financial problems than males with Low conduct problems (45.6%), the researchers found that CL females (20.0%) resembled Low females (55.1%) on virtually all mental health, physical health, and economic outcomes at age 32. Notably, in a recent follow-up study using the Dunedin sample, Rivenbark et al. (Reference Rivenbark, Odgers, Caspi, Harrington, Hogan, Houts and Moffitt2018) found that LCP individuals (9.0%) had the greatest service utilization between 26 and approximately 38 years of age. However, compared to individuals with Low conduct problems (50.3%), those on the CL pathway (22.1%) were more likely to receive criminal convictions, make injury claims, and use social welfare benefits in adulthood. CL individuals were also more likely than Low individuals to display high service use across multiple domains (i.e., criminal justice, social welfare, health). These findings suggest that early-onset conduct problems can have long-term costs for society – even when they decrease before adolescence. Results from other longitudinal samples followed into adulthood similarly indicate that CL conduct problems pose a risk for negative outcomes (e.g., the Zuid-Holland population-based sample; Bongers et al., Reference Bongers, Koot, van der Ende and Verhulst2008; Reef et al., Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2010, Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2011).
Overall, there is evidence that individuals who display declining childhood conduct problems are still at elevated risk for later internalizing problems, antisocial behavior, health and financial problems, social difficulties, and higher service use (e.g., Bongers et al., Reference Bongers, Koot, van der Ende and Verhulst2008; Kjeldsen, Nilsen, Gustaven, Shipstein, & Melkevik, Reference Kjeldsen, Nilsen, Gustaven, Shipstein and Melkevik2016; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008; Reef et al., Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2010, Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2011; Rivenbark et al., Reference Rivenbark, Odgers, Caspi, Harrington, Hogan, Houts and Moffitt2018; Sentse et al., Reference Sentse, Kretschmer, de Haan and Prinzie2017). In a meta-analysis, Bevilacqua et al. (Reference Bevilacqua, Hale, Barker and Viner2018) proposed that “full recovery from conduct problems rarely occurs” (p. 11), since CL individuals experience some maladjustment in adulthood relative to typically developing individuals. That said, the exact nature and degree of later maladjustment associated with early-onset-declining conduct problems remains unclear, which is in part related to the paucity of studies looking at outcomes beyond the age of 21. It is therefore imperative to further investigate the long-term developmental outcomes associated with different pathways of childhood conduct problems.
The present study
The aim of this study was to investigate trajectories of childhood conduct problems and their associated long-term developmental outcomes in adulthood (age 25). Employing data from the Fast Track project (CPPRG, 2019), this study proceeded in two general steps. First, a group-based modeling technique (LCGA) was used to examine childhood conduct problem trajectories. Because the Fast Track recruiting procedure selected for a disproportionately high-risk sample of children (described in detail below), it was hypothesized that different trajectories of early-onset conduct problems, including both a persistent and a declining pathway, would emerge. Given that the present sample also included a subset of typically developing children, however, it was hypothesized that a trajectory characterized by stable-low conduct problems would be identified as well. Second, a broad range of distal (i.e., age 25) outcomes were examined, including psychopathology, substance use, risky sexual behavior, antisocial behavior, and adaptive outcomes. In light of previous research (e.g., Bongers et al., Reference Bongers, Koot, van der Ende and Verhulst2008; Kjeldsen et al., Reference Kjeldsen, Nilsen, Gustaven, Shipstein and Melkevik2016; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008; Reef et al., Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2010, Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2011; Sentse et al., Reference Sentse, Kretschmer, de Haan and Prinzie2017), we hypothesized that an early-onset-declining trajectory would be associated with more adverse adult outcomes than a stable-low trajectory; however, no specific predictions were made due to the inconsistency of existing evidence. By examining long-term developmental sequelae of early-onset conduct problems in a disproportionately high-risk sample of diverse children, this study adds to the literature by explicitly investigating heterogeneity among “early starters.” Such investigations are critical to advance the assessment, prevention, and treatment of youth conduct problems.
Method
Participants
The proposed study utilized data from the Fast Track Project, which began with the selection of 55 elementary schools deemed to be high risk based on neighborhood crime and poverty in four geographical locations in the United States: Seattle, Washington (n = 15); Nashville, Tennessee (n = 10); Durham, North Carolina (n = 13); and rural Pennsylvania (n = 17). Schools within these sites were then matched based on size, ethnic composition, and poverty rates, and randomly assigned to either intervention or control conditions. Within these schools, 9,594 kindergarten children (approximately 6 years of age) across three cohorts (1991–1993) participated in a multiple-gating screening procedure (Lochman & CPPRG, Reference Lochman1995). The procedure began with a screening for classroom conduct problems that utilized teacher ratings on items from the Teacher Observation of Classroom Adaptation – Revised (Werthamer-Larsson, Kellam, & Wheeler, Reference Werthamer-Larsson, Kellam and Wheeler1991). Children found to be in the top 40% of their cohort and site were then screened for externalizing behavior problems at home using parent ratings on 24 items drawn from existing behavior checklists (i.e., Child Behavior Checklist, Achenbach, Reference Achenbach1991; Revised Problem Behavior Checklist, Quay & Peterson, Reference Quay and Peterson1987). Next, a “total severity-of-risk” screen score was created by summing standardized scores on the parent and teacher screens, and children with the highest total risk scores were selected for inclusion in the study until desired sample sizes were reached across sites, schools, and groups. Children were not included in the study if they refused to participate or failed to enroll in first grade at 1 of the 55 core schools. Deviations from the selection procedure were also made to ensure that no child would be the only girl in an intervention group.
Ultimately, 891 children participated in the randomized controlled trial, with 445 and 446 children being assigned to the intervention and high-risk control groups, respectively. In addition, a normative comparison sample (n = 387) was selected from children in the first cohort from the control schools (i.e., approximately 100 children from each site), to represent the population-normative range of conduct problems within the schools. Annual assessments of all children took place post-kindergarten through 2 years post-high school, with the entire sample being assessed again at age 25. In the current project, only data from the high-risk control and normative comparison groups were utilized. Since the normative comparison group included some children from the high-risk control group (n = 79), the final sample consisted of 754 children. The final sample was 58% male, 50% White, 46% Black, 1.6% Hispanic, 0.4% Asian, 0.3% Native American, and 1.7% other race.
Measures
At the outset of the Fast Track project, parents reported on child age, child sex (0 = female, 1 = male), child race, and family socioeconomic status (SES). In addition, geographic site was recorded for each participant. Consistent with previous studies (e.g., CPPRG, 2002), a race/urban status composite variable (0 = Urban White, 1 = Urban Black, 2 = Rural White) was created to account for the strong association between race and site in the Fast Track sample (i.e., Black participants were more likely to come from urban sites, while the only rural site was primarily White). For all analyses, this race/urban status variable was dummy coded into dichotomous indicators (0 = no, 1 = yes) of Urban White, Urban Black, and Rural White status.
Childhood conduct problems were measured using parent report on the CBCL (Achenbach, Reference Achenbach1991). The CBCL is widely used to assess child behavior problems and has good reliability and validity (Achenbach, Reference Achenbach1991). This checklist requires parents to rate the applicability of a series of statements (e.g., “Bullies others”) to a target child over the past 6 months using a 0-1-2 response scale (0 = not true; 1 = somewhat or sometimes true; 2 = very true or often true). Reponses are then used to calculate eight syndrome scale scores as well as broadband Externalizing, Internalizing, and Total Problem scores. Parents completed the CBCL in the summer following the children's kindergarten year (M age = 5.89) as well as in the summers following grades 1, 2, 4, 5, and 7. Raw (sum) scores on the CBCL Externalizing broadband scale were used to identify childhood conduct problem trajectories. The Externalizing scale is comprised of 33 items, from the aggression and delinquency narrowband scales of the measure.
The present study examined five areas of psychosocial functioning at age 25: psychopathology, substance use, risky sexual behavior, antisocial behavior, and adaptive outcomes. The same outcome measures were used previously in a follow-up study published by the CPPRG (Dodge et al., Reference Dodge, Bierman, Coie, Greenberg, Lochman and McMahon2015).
Psychopathology was assessed using self- and peer-report on the Adult Self-Report (ASR) and the Adult Behavior Checklist-Friend (ABCL-F) (Achenbach & Rescorla, Reference Achenbach and Rescorla2003). Participants completed the ASR and nominated one peer (e.g., spouse, friend) to complete the ABCL-F. Both of these 132-item instruments have shown good reliability and validity (Achenbach & Rescorla, Reference Achenbach and Rescorla2003). They require respondents to report on the applicability of various statements regarding the participant's symptoms on a 3-point scale (0 = not true; 1 = somewhat or sometime true; 2 = often true). The ASR and ABCL-F provide DSM-oriented scales, which were based on criteria recommended by an international panel of judges to be consistent with DSM-IV criteria. Binary diagnostic indicators (1 = present; 0 = absent) were used for the following clinical problems: adult ADHD, antisocial personality disorder (APD), avoidant personality disorder (AvPD), somatic problems, anxiety problems, and depressive problems. Participants’ symptoms were considered to be in the clinical range if peer- or self-ratings indicated that individuals met criteria for a given disorder.
Substance use was assessed using self- and peer report on the third version of the Tobacco, Alcohol, and Drugs (TAD) Survey (Bureau of Labor Statistics, U.S. Department of Labor, 2002; Elliot, Huizinga, & Ageton, Reference Elliot, Huizinga and Ageton1985) as well as an alcohol and drug interview module that was adapted from the National Institute of Mental Health Diagnostic Interview Schedule (Robins, Helzer, Croughan, & Ratcliff, Reference Robins, Helzer, Croughan and Ratcliff1981). Four binary indicators of self- or peer-reported substance use problems at age 25 were examined: (a) regular binge drinking (i.e., 5+ drinks on one or more occasion in the last month and 5+ drinks on 12 or more occasions in the last year); (b) heavy marijuana use (i.e., 27+ days of use in the past month); (c) serious substance use (i.e., use of crack, cocaine, inhalants, heroin, LSD, phencyclidine, ecstasy, mushrooms, speed, or other pills not prescribed by a physician in the past month); and (d) a diagnostic indicator of alcohol abuse (i.e. created using DSM-IV diagnostic criteria assessed during the alcohol and drug interview module). Consistent with previous work (Dodge et al., Reference Dodge, Bierman, Coie, Greenberg, Lochman and McMahon2015), a binary measure of any self- or peer-reported problematic substance use was also used, scored 1 if any of the four substance use problems were met and 0 otherwise.
Risky sexual behavior was assessed using self-report on the 37-item Overview of Sexual Experiences (Capaldi, Reference Capaldi2002), a self-report questionnaire developed to assess various characteristics of participants’ sexual experiences over their lifetime and in the past 12 months (e.g., number of sexual partners, contraction of sexually transmitted diseases, contraceptive use). Lifetime number of sexual partners was assessed on a 0 to 7 scale (0 = 0; 1 = 1–2; 2 = 3–5; 3 = 6–10; 4 = 11–15; 5 = 16–20; 6 = 21–50; 7 = 50 or more). In addition, a variable for risky sexual behavior in the past 12 months was previously created for the Fast Track project by multiplying the number of partners in the past year with the sum of two scales: new-partner condom non-use and regular partner condom-non-use (Dodge et al., Reference Dodge, Bierman, Coie, Greenberg, Lochman and McMahon2015). Participants rated their new partner condom non-use from 0 (no new partner) to 5 (never use), and they rated their regular partner condom non-use from 1 (never non-use) to 5 (never use).
Adult antisocial behavior was assessed using measures of criminality and relationship violence. Criminality was assessed using information on convictions and diversions from local court records as well as a national database. Severity weighted indices of adult substance convictions, violent convictions, and property and public order (PPO) convictions were created in the Dodge et al. (Reference Dodge, Bierman, Coie, Greenberg, Lochman and McMahon2015) study by multiplying frequencies by severity across all lifetime adult convictions. Severity levels for substance crimes range from 1 to 2 (1 = possession; 2 = manufacturing and possession with intent to sell). For violent crimes, severity levels range from 1 to 3 (1 = DUI and carrying a concealed weapon; 2 = robbery and first-degree burglary; and 3 = aggravated/armed robbery, murder, rape, kidnapping, sex offenses, and first-degree assault). Severity of PPO crimes ranges from 1 to 3 (e.g., 1 = public consumption/open container, loitering, curfew violation; 2 = obstructing justice, disorderly conduct, unauthorized use of a vehicle, theft under $1,000; 3 = criminal assistance, evading arrest, extortion, theft over $1,000).
Romantic partner violence was assessed using the General Violence Questionnaire (Holtsworth-Monroe, Rehman, & Herron, Reference Holtsworth-Monroe, Rehman and Herron2000). Participants and their self-nominated peers reported on the number of times that participants had engaged in the following violent acts toward any romantic partner in the past year: threatened with a knife or gun; pushed, shoved, grabbed, slapped, or threw something; punched, hit, kicked, bit, or slammed against a wall, beat up or choked, strangled, burned, or scalded on purpose; or used a knife or gun. Items were rated on a scale of 0–3 (with 3 indicating 3 or more times) and item scores were summed for each reporter. The present study used the self- and peer-reported average.
Adaptive outcomes included education, employment, and well-being. Binary indicators (1 = yes; 0 = no) of educational attainment and current employment at age 25 were used to assess whether participants (a) had graduated high school or received a General Equivalency Diploma (GED) and (b) were currently employed full time or enrolled in post-secondary, respectively. These items were created from the Education Information and Employment History measures from the National Longitudinal Survey (Howe & Frazis, Reference Howe and Frazis1992). General well-being was assessed using self- and peer-report measures of happiness, personal strength, and general health. Happiness and personal strength were both assessed using select items from the ASR and the ABCL-F (Achenbach & Rescorla, Reference Achenbach and Rescorla2003). Participants and their self-nominated peers both also completed the 36-item Short-Form Health Survey (Ware & Sherbourne, Reference Ware and Sherbourne1992), which included four items assessing overall health status, presence of chronic conditions, magnitude of bodily pain, and presence of physical health issues that impacted work. A general well-being score was created by averaging scores across the standardized general health index, personal strength, and happiness scores, separately for self- and peer report (Dodge et al., Reference Dodge, Bierman, Coie, Greenberg, Lochman and McMahon2015). The self- and peer-reported average well-being score was used in the present analyses.
Analysis Plan
Statistical analyses proceeded in four steps. First, SPSS 19.0 (IBM Corp., 2010) was used to conduct descriptive analyses. Second, Mplus version 7.31 (Muthén & Muthén, Reference Muthén and Muthén1998–2012) was used to conduct LCGA to identify unique latent trajectories of childhood conduct problems from kindergarten to grade 7. A series of models were examined in a stepwise fashion (i.e., adding a class with each model) and a single model was selected by comparing fit indices, including (a) information criteria [i.e., the Akaike information criteria (AIC), the Bayesian information criteria (BIC), and the sample size-adjusted BIC (aBIC)], with lower values reflecting better model fit; and (b) likelihood ratio tests [i.e., Lo-Mendell-Rubin adjusted likelihood ratio test (LMR-LRT: Lo, Mendell, & Rubin, Reference Lo, Mendell and Rubin2001), and the Vuong-Lo-Mendell-Rubin likelihood ratio text (VLMR-LRT; Lo et al., Reference Lo, Mendell and Rubin2001)]. These tests are statistical comparisons of fit between a given model with k classes and a model with one fewer classes (i.e., k−1), with significant p values indicating improved model fit with the k-class model. Linear and quadratic slopes were included. To avoid a local minimum, multiple random starting values were used, and each class model was run 500 times. Entropy was also examined as an indicator of class separation, with a value closer to 1.00 being preferred. In addition to statistical indices of model fit, class size (i.e., prevalence) and the interpretability of identified classes were also considered to ensure that the models made substantive sense in light of developmental theory and previous findings.
Next, the three-step approach (Asparouhov & Muthén, Reference Asparouhov and Muthén2014) was used to examine predictors of trajectory group membership. In the three-step approach, latent trajectory groups are first identified in the manner described above. Individuals are then assigned to their most likely group based on posterior probabilities obtained through model estimation. A nominal variable is created to represent each participant's most likely group membership. In the third step, predictors are included into the model and regressed on this nominal group membership variable, taking misclassification into account. In the present study, child age, sex, family SES, initial screen scores, and race/urban status were examined as possible predictors of trajectory group membership. For analyses involving the dummy coded race/urban status variable (described above), the Urban Black group served as the reference class. Predictors were controlled for in subsequent outcome analyses if they were found to have significant associations with trajectory group membership. In the last step, associations between class membership and age 25 outcomes were examined in SPSS, using either analyses of covariance (ANCOVAs) for continuous outcomes or binary logistic regression for dichotomous outcomes. Given the number of adult variables examined, a Bonferroni correction was applied to omnibus F and χ 2 tests (alpha = 0.0025).
Missing data and attrition analyses
Missing data on childhood conduct problems increased over time, ranging from nearly 0% (n = 7) in kindergarten to 18% (n = 136) in grade 7. In the LCGA, missing data were accommodated using full information maximum likelihood estimation (FIML), which assumes data are missing at random (Rubin & Little, Reference Rubin and Little2002). Thus, the full sample (n = 754) was used to identify childhood conduct problem trajectories. To test the associations between latent class membership and predictors/distal outcomes, however, only participants with available data were included in the analyses. Full information was available on predictors for 717 participants (95% of the sample). On age 25 outcomes, rates of missingness ranged from 7% (adult drug convictions and educational attainment, both n's = 698) to 28% (romantic partner violence, n = 544).
Participants with and without missing data on conduct problems at each of the six time points and on adult outcomes at age 25 were compared on baseline demographic variables and kindergarten CBCL Externalizing scores. To remain consistent with the main outcome analyses, a Bonferroni-corrected alpha of 0.0025 was applied to attrition analyses involving age 25 outcomes. Notably, participants with and without missing data on conduct problems did not differ on sex, initial screen scores, or kindergarten CBCL Externalizing scores. No significant differences regarding baseline demographics were revealed between participants with and without missing data on conduct problems either in grades 2 or 7. Modest differences in demographic variables were revealed at kindergarten and grades 1, 4, and 5: Those with missing data on conduct problems in kindergarten tended to be a bit older, t(752) = 2.00, p = .045; those with missing data on conduct problems in grade 1 had slightly higher family SES, t(752) = 2.05, p = .04; those with missing data on conduct problems in grade 4 were more likely to be Urban White or Rural White and less likely to be Urban Black, χ 2(2) = 7.98, p = .02; and those with missing data on conduct problems in grade 5 were more likely to be Urban White and less likely to be Urban Black, χ 2(2) = 9.48, p = .01. Hence, in general, there was no evidence of differential attrition on conduct problems with respect to initial levels of conduct problems or risk. At age 25, missingness on adult outcomes was related to child sex (i.e., being male) and, to a lesser extent, race/urban status (i.e., greater likelihood of being Urban Black and lower likelihood of being Urban White or Rural White). Those with missing data on adult drug, violent, and PPO convictions had higher initial screen scores, suggesting potential differential attrition on age 25 criminality outcomes with respect to kindergarten risk for conduct problems.
Results
Descriptive statistics
Tables 1–3 provide descriptive statistics and bivariate correlations between conduct problems, predictors, and age 25 outcomes. Skewness and kurtosis were high for five of the adult outcomes (i.e., risky sexual behavior, drug convictions, violent convictions, PPO convictions, and romantic partner violence), so these variables were log transformed for all subsequent analyses. Conduct problems were significantly correlated across time (rs ranging between 0.54 and 0.77). In terms of potential predictors, conduct problems were modestly correlated with child sex (rs ranging between 0.16 and 0.19) and family SES (rs ranging between −0.14 and −0.19), and moderately correlated with initial screen scores (rs ranging between 0.45 and 0.57), at each time point. Conduct problems also showed small to moderate correlations with most age 25 outcomes (rs ranging between −0.29 and 0.32). Notably, there were very few significant correlations between conduct problems and most substance use outcomes (rs ranging between 0.02 and 0.12 for regular binge drinking, marijuana use, serious substance use, and alcohol abuse). The only exception was the “any substance problem” indicator, which showed modest correlations with conduct problems across time (rs ranging from 0.08 to 0.16).
Table 1. Bivariate correlations between CBCL Externalizing raw scores and predictor variables

Note. EXTK = Kindergarten Externalizing raw scores, EXT1 = Grade 1 Externalizing raw scores, EXT2 = Grade 2 Externalizing raw scores, EXT4 = Grade 4 Externalizing raw scores, EXT5 = Grade 5 Externalizing raw scores, EXT7 = Grade 7 Externalizing raw scores, Age = age at kindergarten, Male = male indicator, SES = family socioeconomic status at kindergarten, ISS = initial screen score, UW = Urban White, RW = Rural White, UB = Urban Black.
* p < .05, ** p < .01.
Table 2. Bivariate correlations between CBCL Externalizing raw scores and age 25 psychopathology and substance use outcomes

Note. EXTK = Kindergarten Externalizing raw scores, EXT1 = Grade 1 Externalizing raw scores, EXT2 = Grade 2 Externalizing raw scores, EXT4 = Grade 4 Externalizing raw scores, EXT5 = Grade 5 Externalizing raw scores, EXT7 = Grade 7 Externalizing raw scores, APD = antisocial personality disorder, ADHD = attention-deficit/hyperactivity disorder, AvPD = avoidant personality disorder, SOM = somatic problems, ANX = anxiety problems, DEP = depression problems, BING = regular binge drinking, MARI = heavy marijuana use, SSU = serious substance use, AA = alcohol abuse, ANY = any substance problem.
* p < .05, ** p < .01.
Table 3. Bivariate correlations between CBCL Externalizing raw scores and age 25 risky sexual behavior, antisocial behavior, and adaptive outcomes

Note. EXTK = Kindergarten Externalizing raw scores, EXT1 = Grade 1 Externalizing raw scores, EXT2 = Grade 2 Externalizing raw scores, EXT4 = Grade 4 Externalizing raw scores, EXT5 = Grade 5 Externalizing raw scores, EXT7 = Grade 7 Externalizing raw scores, LNP = lifetime number of sexual partners, RSB = risky sexual behavior scale, DRUG = lifetime index adult drug convictions, VIOL = lifetime index adult violent convictions, PPO = lifetime index adult property and public order convictions, HS = graduated high school or obtained General Equivalency Diploma, WELL = general well-being score.
1 Log-transformed for correlational analyses.
* p < .05, ** p < .01.
Developmental trajectories of childhood conduct problems
Table 4 provides fit indices of 1- through 7-class models for childhood conduct problems. For the 4-class model, the significant LMR-LRT (p = .00) and VLMR-LRT (p = .00) suggested better model fit over the 3-class model. The lower information criteria in the 4-class solution (AIC = 27161.13, BIC = 27258.26, aBIC = 27191.58) also suggested better model fit than the 3-class solution (AIC = 27445.30, BIC = 27523.94, aBIC = 27469.95). Despite the slightly lower information criteria in the 5-class solution (AIC = 27073.78, BIC = 27189.42, aBIC = 27110.03), the nonsignificant LMR-LRT and VLMR-LRT suggested that including a fifth class did not significantly improve model fit. In light of these statistical indices, as well as parsimony and interpretability, the 4-class solution was selected. Entropy for the final model was high, indicating high classification.
Table 4. Model fit indices

Note. LL = log-likelihood, AIC = Akaike Information Criteria, BIC = Bayesian Information Criteria, aBIC = sample size-adjusted BIC, LMR-LRT = Lo-Mendell-Rubin adjusted likelihood ratio test, VLMR-LRT = Vuong-Lo-Mendell-Rubin likelihood ratio test. Best model bolded.
The estimated developmental trajectories for the 4-class solution are depicted in Figure 1. The majority of children (38.8%) displayed moderately elevated conduct problems in kindergarten (intercept = 16.85, SE = 0.58, p = .00) that decreased through grade 7 (slope = −1.41, SE = 0.24, p = .00), labeled the moderate decreasing (MD) group. The next largest group (35.5%) had low levels of conduct problems in kindergarten (intercept = 7.74, SE = 0.44, p = .00) that decreased through grade 7 (slope = −0.90, SE = 0.16, p = .00), labeled the low decreasing (LD) group. Furthermore, 22% of the sample followed a trajectory characterized by high conduct problems in kindergarten (intercept = 23.21, SE = 0.74, p = .00) that remained stable through grade 7 (slope = 0.07, SE = 0.37, p = .85), labeled the high stable (HS) group. Finally, 3.7% of the sample displayed very high levels of conduct problems in kindergarten (intercept = 30.61, SE = 1.71, p = .00) that increased through grade 7 (slope = 3.80, SE = 1.15, p = .00), labeled the extremely high increasing (EHI) group.

Figure 1. Predicted developmental trajectories of childhood conduct problems. Note. MD = Moderate decreasing; LD = low decreasing; EHI = extremely high increasing; HS = high stable; K = kindergarten.
Prediction of childhood conduct problem trajectories
Child age at study time 1 (i.e., post-kindergarten), child sex, family SES, initial screen scores, and race/urban status were examined as possible predictors of trajectory group membership (see Table 5). Trajectory group membership was not significantly predicted by initial child age, child sex, or race/urban status.
Table 5. Trajectory group membership prediction with multinomial logistic regression (n = 717)

Note. EHI = extremely high increasing; HS = high stable; MD = moderate decreasing; OR = odds ratio; SES = socioeconomic status.
a Low Decreasing as reference group.
b Moderate Decreasing as reference group.
c High Stable as reference group.
d At kindergarten.
e Urban Black as the reference group.
* p < .05, ** p < .01.
Family SES and initial screen scores were significantly associated with trajectory group membership. Children from families of lower SES were significantly more likely to be in the EHI and HS groups, as compared to both the MD group (EHI vs. MD: B = −0.05, SE = 0.02, p = .03; HS vs. MD: B = −0.02, SE = 0.01, p = .03) and the LD group (EHI vs. LD: B = −0.07, SE = 0.03, p = .01; HS vs. LD: B = −0.04, SE = 0.01, p = .00). Children with higher initial screen scores were more likely to be in the MD (B = 0.84, SE = 0.11, p = .00), HS (B = 1.23, SE = 0.14, p = .00) and EHI (B = 2.14, SE = 0.26, p = .00) groups than the LD group. Among the three groups with elevated conduct problems, children with higher screen scores were significantly more likely to be in the EHI group than the HS (B = 0.91, SE = 0.24, p = .00) and MD (B = 1.30, SE = 0.24, p = .00) groups, and significantly more likely to be in the HS group than the MD group (B = 0.39, SE = 0.11, p = .00). Given these findings, family SES and initial screen scores were included as covariates in all subsequent outcome analyses, to increase confidence that any group differences observed on adult outcomes were due to conduct problem trajectory membership (vs. group differences on these baseline characteristics).
Prediction of age 25 outcomes by childhood conduct problem trajectories
Probability/mean differences in age 25 outcomes by trajectory group membership, controlling for family SES and initial screen scores, are presented in Table 6.
Table 6. Probability/mean differences in age 25 outcomes by trajectory group membership controlling for SES and initial screen scores
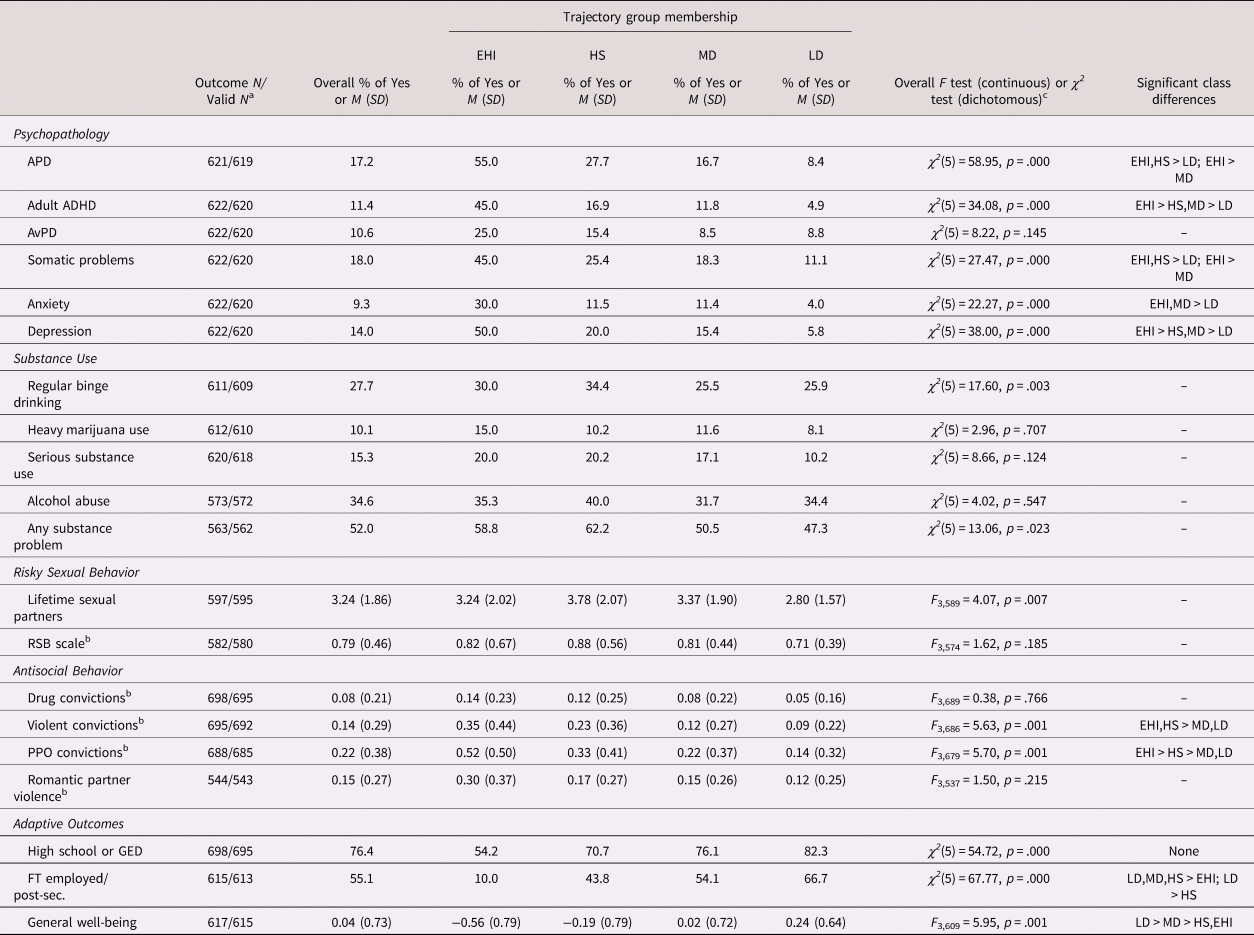
Note. EHI = extremely high increasing; HS = high stable; MD = moderate decreasing; LD = low decreasing; APD = antisocial personality disorder; ADHD = attention-deficit hyperactivity disorder; AvPD = avoidant personality disorder; RSB = risky sexual behavior; PPO = property and public order; GED = General Equivalency Diploma; FT = full-time.
a A maximum of 3 participants were excluded from each set of outcome analyses, depending on patterns of missingness on one covariate (initial screen score) and age 25 outcomes.
b Log-transformed.
c Bonferroni-corrected α = .0025 used for omnibus tests.
There were significant differences between conduct problem trajectory groups on all but one psychopathology outcome at age 25 (i.e., avoidant personality problems). The EHI group was significantly more likely to have symptoms of APD, ADHD, somatic problems, and depression by age 25 than the LD and MD groups. The EHI group also displayed significantly more problems with anxiety than the LD group, as well as more problems with adult ADHD and depression than the HS group. Those in the HS and MD groups did not significantly differ on any of the age 25 psychopathology outcomes, and both groups displayed significantly more problems with ADHD and depression at age 25 than the LD group. However, the MD and HS groups differed in several ways in their pairwise comparisons with the LD group. Specifically, compared to the LD group, the HS group was significantly more likely to exhibit APD and somatic problems at age 25, whereas the MD group was significantly more likely to display anxiety problems.
No significant differences were observed between trajectory groups on any of the age 25 substances use (i.e., regular binge drinking, heavy marijuana use, serious substance use, alcohol abuse, any substance problem) or risky sexual behavior (i.e., lifetime number of sexual partners, 12-month risky sexual behavior scale) outcomes.
In terms of adult antisocial behavior, individuals in the EHI and HS groups had significantly more index adult violent and PPO convictions by age 25 than those in the MD and LD groups. There was no significant difference between the EHI and HS groups on adult violent convictions, but membership in the EHI group was associated with significantly more adult PPO convictions by age 25 than membership in the HS group. Trajectory group membership did not significantly predict adult drug convictions or romantic partner violence.
Regarding adaptive outcomes, at age 25, individuals in the EHI group were significantly less likely than those in all other groups to be employed full-time or enrolled in post-secondary education at age 25 (i.e., only 10.0% of the EHI group). Those in the LD group were significantly more likely than those in the HS group to be employed full-time or in post-secondary education (LD: 66.7% vs. HS: 43.8%), but the MD group did not significantly differ from the LD or the HS groups on this outcome (MD: 54.1%). Overall, individuals in the LD group displayed the greatest well-being at age 25, but those in the MD group also exhibited significantly higher general well-being scores than those in the EHI and HS groups. Although the omnibus test for high school/GED completion was significant, family SES was the only significant predictor in the model. In other words, controlling for SES, trajectory group membership did not predict high school-level education attainment.
Discussion
Moffitt's (Reference Moffitt1993) developmental taxonomy has led to great advances in our understanding of the developmental course of antisocial behavior throughout the lifespan. The original distinction Moffitt made between EOP and AO conduct problems has been supported by decades of research (Jennings & Reingle, Reference Jennings and Reingle2012; Moffitt, Reference Moffitt, Cullen, Wright and Blevins2008, Reference Moffitt2018), and is now regularly utilized in clinical practice (APA, 2013). More recently, however, empirical attention has been directed towards a previously unrecognized subgroup of children, whose early-onset conduct problems steadily decline before adolescence. Given the current lack of consensus in the research literature on this CL pathway (Moffitt, Reference Moffitt2018), the present study examined the long-term outcomes of different childhood conduct problem trajectories in a disproportionately high-risk sample.
Childhood conduct problem trajectories
Consistent with hypotheses and previous research (Brennan & Shaw, Reference Brennan and Shaw2013; Jennings & Reingle, Reference Jennings and Reingle2012; Moffitt, Reference Moffitt2018), a group characterized by consistently low childhood conduct problems was identified. The LD group (approximately 35% of the sample) displayed low levels of conduct problems in kindergarten that decreased through grade 7. Also consistent with hypotheses, multiple “early-starting” conduct problem trajectory groups were identified, including groups that followed both persistent and decreasing pathways. First, in line with Moffitt's (Reference Moffitt1993) taxonomy and much of the research on developmental trajectories of antisocial behavior (see Jennings & Reingle, Reference Jennings and Reingle2012, for a review), a group characterized by HS conduct problems was identified. The HS group comprised approximately 22% of the sample and exhibited high levels of conduct problems in kindergarten that remained stable through grade 7. Second, the largest group identified, the MD group (approximately 39% of the sample), displayed initially moderate levels of conduct problems that steadily decreased throughout childhood.
A third, unanticipated group of “early starters” was identified in this study. The EHI group comprised approximately 4% of the sample, and displayed the highest levels of conduct problems in kindergarten, which increased through grade 7. Such a group has not consistently emerged in the literature (Jennings & Reingle, Reference Jennings and Reingle2012), but may reflect the fact that children at high risk for conduct problems were overrepresented in the present sample. Of note, the CPPRG (2007, 2011) previously found that children in the top 3rd percentile of initial screen scores were particularly likely to develop externalizing disorders between grades 3 and 12 if they did not receive the Fast Track preventive intervention. These findings lend support to the existence of a small but extremely antisocial group of “early starters” in the Fast Track sample, whose conduct problems exacerbated over time.
Predictors of trajectory group membership
In this study, family SES and initial screen scores were the only significant predictors of trajectory group membership. In terms of SES, individuals from economically disadvantaged families were more likely to belong to the EHI and HS groups than the LD or MD groups, which is in line with Moffitt's (Reference Moffitt1993) original hypotheses as well as the current evidence base regarding individuals with EOP (or LCP) conduct problems (Moffitt et al., Reference Moffitt, Arseneault, Jaffee, Kim-Cohen, Koenen, Odgers and Viding2008). However, family SES was not differentially associated with MD and LD group membership. With respect to initial levels of risk, individuals with the highest kindergarten screen scores were most likely to belong to the EHI group, followed by the HS, MD, and LD groups. This suggests that early measures of risk – such as the multiple-gate screening procedure used in the Fast Track project (see Lochman & CPPRG, Reference Lochman1995) – can be relatively good indicators of the developmental course of conduct problems throughout childhood.
Child sex did not emerge as a significant predictor of trajectory group membership. This is notable, since some have contended that females follow different trajectories of antisocial behavior than males (e.g., Denno, Reference Denno1994; Elliot, Reference Elliot1994; Silverthorn & Frick, Reference Silverthorn and Frick1999; as discussed by Fontaine, Carbonneau, Vitaro, Barker, & Tremblay, Reference Fontaine, Carbonneau, Vitaro, Barker and Tremblay2009; and Brennan & Shaw, Reference Brennan and Shaw2013). In the most recent review of the literature on this issue, Brennan and Shaw (Reference Brennan and Shaw2013) specifically examined evidence relevant to early-starting pathways of conduct problems in females. They concluded that “males and females follow similar developmental trajectories”; however, the authors also noted that “a larger proportion of males tended to follow an early-starting persistent pathway” (p. 49). In this study, being male (vs. female) was not differentially associated with trajectory group membership. These findings might be explained by the composition of the present sample, which included a high proportion (59%) of males and females identified to be at high risk for conduct problems in kindergarten.
Age 25 psychosocial outcomes
In general, early-onset-persistent conduct problems were associated with the poorest psychosocial functioning at age 25. Members of the EHI and HS trajectory groups displayed more antisocial behaviour, lower rates of employment, and poorer well-being than those in the MD and LD trajectory groups. In direct contrast, membership in the LD group was associated with the greatest psychosocial adjustment at age 25. Compared to those in the other conduct problem groups, individuals in the LD group displayed the lowest levels of psychopathology and the greatest general well-being in adulthood. Individuals who displayed MD conduct problems had a more complicated picture at age 25. While they displayed relatively positive adjustment in certain domains, they nevertheless displayed more psychosocial problems at age 25 than the LD group. Importantly, these findings cannot be explained by trajectory group differences on baseline family SES or initial screen scores, as these predictors were included as covariates in the outcome analyses.
These findings are generally consistent with the existing evidence base. For example, in a meta-analysis of 13 studies examining psychosocial outcomes associated with conduct problem trajectories, Bevilacqua, Hale, Barker, and Viner (Reference Bevilacqua, Hale, Barker and Viner2018) concluded that EOP, AO, and CL trajectories were all linked with poorer longer-term outcomes than the Low trajectory; however, they found “a consistent hierarchy of risk” among these conduct problem groups, with the EOP group being associated with the worst outcomes, followed by the AO group, and then the CL group (p. 11). A similar hierarchy of risk was observed in the present study: EOP conduct problems (i.e., displayed by the EHI and HS groups) were associated with the worst psychosocial outcomes, but early-onset-declining conduct problems (i.e., displayed by the MD group) were also associated with some problems in adulthood. This hierarchy was evident amongst the two EOP groups as well, with the EHI group exhibiting more psychopathology (ADHD, depression), more adult PPO convictions, and lower employment at 25 than the HS group. Another notable finding is that membership in the EHI and HS groups was associated with more antisocial behavior in adulthood, whereas membership in the MD group was not. Rather, the relative maladjustment of those in the MD group was more likely to take the form of elevated internalizing problems, ADHD, and lower well-being at age 25. Similar findings regarding adult internalizing problems among those on the early-onset-declining (or CL) trajectory have been reported elsewhere (e.g., Kjeldsen et al., Reference Kjeldsen, Nilsen, Gustaven, Shipstein and Melkevik2016; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008; Reef et al., Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2010; Sentse et al., Reference Sentse, Kretschmer, de Haan and Prinzie2017).
This suggests that early-starting conduct problems can pose a risk for later maladjustment, even when there is apparent recovery from antisocial behavior. In line with developmental cascade theory (Masten & Cicchetti, Reference Masten and Cicchetti2010), displaying conduct problems at a critical transition point such as school entry might set a “snowball effect” in motion, leading to other psychosocial consequences. For example, the dual failure model suggests that early conduct problems give rise to academic difficulties and peer rejection, which increases the risk for depression (Capaldi, Reference Capaldi1990, Reference Capaldi1991; Patterson & Capaldi, Reference Patterson, Capaldi, Rolf, Masten, Cicchetti, Nuchterlein and Weintraub1990). Therefore, it may be that individuals on the early-onset-declining pathway experience conduct problems severe enough to interfere on some level with the early development of social-emotional and academic competencies, potentially putting them at continued risk for maladjustment – particularly emotional problems – despite improvement in behavior over time (Jones, Greenberg, & Crowley, Reference Jones, Greenberg and Crowley2015; Masten et al., Reference Masten, Roisman, Long, Burt, Obradovic, Riley and Tellegen2005; Moilanen, Shaw, & Maxwell, Reference Moilanen, Shaw and Maxwell2010).
It is also possible that children with declining conduct problems continue to display fundamental difficulties with self-regulation throughout childhood and into adolescence and adulthood, but that their challenges manifest differently throughout development (i.e., display heterotypic continuity; Cicchetti & Rogosch, Reference Cicchetti and Rogosch1996) given the presence of certain environmental moderators. As one example, within the family context, it is well established that coercive family processes facilitate the maintenance of child conduct problems (see Patterson, Reference Patterson1982). In families that display this interaction style, parents and children mutually reinforce the escalation of negative behavior in each other. Perhaps in the homes of children on the early-onset-declining pathway, child dysregulation (e.g., in the form of initial acting out behavior) is met with a different parental response (e.g., psychological control, criticism, and/or modeling of withdrawal or avoidance; e.g., Dadds & Roth, Reference Dadds, Roth, Vasey and Dadds2001; Schleider & Weisz, Reference Schleider and Weisz2017), leading to a family process through which early conduct problems are not reinforced but children are nevertheless put at risk for later internalizing problems. In this study, individuals in the MD (vs. LD) trajectory group had higher rates of ADHD at age 25, which suggests that self-regulation (e.g., of attention, emotion, and/or impulses) continued to be a significant challenge for some on this trajectory (Barkley, Reference Barkley2010). In any case, given the higher rates of psychopathology in MD group at age 25, it makes sense that these individuals would experience a poorer sense of well-being in adulthood.
It is notable that no significant differences were found between trajectory groups on the risky sexual behavior or substance use outcomes at age 25. To our knowledge, only one study has investigated sexual risk as an adult outcome of childhood conduct problem trajectories. Odgers et al. (Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008) found that females (but not males) on the LCP trajectory were more likely to receive herpes type 2 diagnoses at age 32 than those on the Low trajectory (Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008). Thus, the null findings on these previously unexamined RSB variables are not surprising. In contrast, there is considerable evidence that individuals with EOP conduct problems are at increased risk for substance use problems in adulthood (e.g., Kretschmer et al., Reference Kretschmer, Hickman, Doerner, Emond, Lewis, MacLeod and Heron2014; Odgers, Caspi, et al., Reference Odgers, Caspi, Broadbent, Dickson, Hancox, Harrington and Moffitt2007; Odgers et al., Reference Odgers, Moffitt, Broadbent, Dickson, Hancox, Harrington and Caspi2008; Reef, Diamontopoulou, van Meurs, Verhulst, & van der Ende, Reference Reef, Diamontopoulou, van Meurs, Verhulst and van der Ende2011). In the present study, base rates of substance use were relatively high at age 25, ranging from 10.1% for heavy marijuana use to 52.0% for any substance problem. It may be that substance use was too prevalent at age 25 in this sample to detect significant differences among trajectory groups. This is consistent with epidemiological evidence that rates of substance use and substance use disorders tend to peak in young adulthood and decline thereafter (e.g., Jackson & Sartor, Reference Jackson, Sartor and Sher2016; Lee, McDowell, & Sher, Reference Lee, McDowell, Sher, Sloboda, Petras, Robertson and Hingson2019).
Strengths and limitations
This study had several strengths. First, the sample was mixed-sex and racially diverse. Given that the primary aim of the present study was to add to the research base on CL conduct problems, the use of an disproportionately high-risk sample was also advantageous, since it increased the probability of identifying multiple subgroups of “early starters.” Second, the present study used a group-based trajectory modeling technique, LCGA, to identify childhood conduct problem trajectories. Third, this study examined a broad range of psychosocial outcomes at age 25, across five domains of functioning (i.e., psychopathology, substance use, risky sexual behavior, antisocial behavior, and adaptive outcomes). Few existing studies utilizing group-based trajectory modeling have examined psychosocial outcomes beyond the age of 21, particularly in U.S. samples (see Bevilacqua et al., Reference Bevilacqua, Hale, Barker and Viner2018). Moreover, unlike existing studies that have relied exclusively on self-report (e.g., Kretschmer et al., Reference Kretschmer, Hickman, Doerner, Emond, Lewis, MacLeod and Heron2014; Sentse et al., Reference Sentse, Kretschmer, de Haan and Prinzie2017), bias was reduced in the assessment of adult outcomes with the use of official records and multiple informants.
Nevertheless, the findings need to be interpreted in light of several limitations. The present study measured childhood conduct problems using the parent-reported CBCL Externalizing scale from kindergarten to grade 7. Although the sole use of parent reports allowed for consistency of raters across time points, it limited the ability to assess the pervasiveness of childhood conduct problems throughout childhood (i.e., across home and school settings). Furthermore, in the outcome analyses, power to detect significant effects was limited by sample size and potential differential attrition, especially with regard to outcomes at age 25. This was particularly an issue in pairwise class comparisons involving the smallest childhood conduct problem group, the EHI group. While descriptive data suggested that trajectory group membership was differentially associated with age 25 outcomes in expected directions, not all apparent group differences were supported in follow-up analyses. Notably, participants with missing data on adult convictions (i.e., for drug, violent, and PPO crimes) tended to have higher initial screen scores. This limits the extent to which the results regarding criminality at age 25 may generalize to children with high early levels of risk for conduct problems. The use of a disproportionately high-risk sample also restricts the generalizability of the present findings. As mentioned above, the current sample included a proportion of children (59%) who were identified as being at high risk for conduct problems at the beginning of kindergarten based on teacher and parent ratings. The remainder of the sample (41%) was selected to represent the population-normative range of kindergarten conduct problems. Since all children were recruited from neighborhoods with higher than average rates of crime and poverty, however, the entire sample could be characterized as high risk. Therefore, although the present findings undoubtedly contribute to the evidence base on early starters, they may not be directly comparable to results from other studies. In particular, the likelihood of identifying a small, early-onset-increasing trajectory (i.e., the EHI group) would be much lower in population-based or normative community samples. Moreover, participants in this study were likely at a generally heightened risk for maladjustment in adulthood given their home and neighborhood environments. That said, this does not explain the differential risk demonstrated in this study posed by different childhood conduct problem trajectories.
Conclusions and future directions
This study provides further evidence for heterogeneity among early starters. Three different early-starting trajectory groups were identified in this disproportionately high-risk sample, including EHI, HS, and MD groups. Notably, not only did most “early starters” follow the MD pathway (i.e., approximately 60% of EHI, HS, and MD individuals), the MD group was the largest overall (i.e., 39% of the entire sample). This supports the contention that a declining trajectory of childhood conduct problems not only exists, but it is relatively common (Fairchild et al., Reference Fairchild, van Goozen, Calder and Goodyer2013). In the outcome analyses, individuals in the EHI and HS groups generally had the poorest psychosocial functioning at age 25, while those in the LD group were relatively well-adjusted. Some unexpected differences were found between the two EOP groups, with the EHI group faring worse than the HS group on certain outcomes. Moreover, individuals in the MD group were more likely to display psychosocial problems at age 25 than those who displayed consistently low conduct problems. These findings indicate that childhood conduct problems increase risk for adverse adult outcomes, even when conduct problems decline throughout childhood. However, the degree and type of long-term risk is related to the severity of conduct problems throughout childhood.
Moving forward, research should continue to examine the developmental outcomes associated with different childhood conduct problem trajectories. As stated above, very few studies utilizing group-based modeling have examined psychosocial outcomes beyond the age of 21, so longitudinal research that spans childhood to adulthood is particularly needed (Bevilacqua et al., Reference Bevilacqua, Hale, Barker and Viner2018). Once some consistency has been established in the differential outcomes of childhood conduct problem trajectories, research should then turn to investigating the mechanisms by which these different pathways incur risk for later maladjustment. Ideally, such research would illuminate the developmental processes involved in different trajectories of early-starting conduct problems. For example, future research should seek to identify which developmental cascades are set in motion with declining childhood conduct problems such that they pose a risk for some psychosocial problems (e.g., internalizing problems, ADHD) but not others (e.g., antisocial behavior) in adulthood. It will be important for future researchers to move beyond the investigation of predictors that distinguish different pathways of early-starting conduct problems, as these efforts have been not led to clinically meaningful insights (Moffitt et al., Reference Moffitt, Arseneault, Jaffee, Kim-Cohen, Koenen, Odgers and Viding2008). Rather, there is a need to investigate the transactional effects of childhood conduct problem trajectories and established risk (e.g., genetic vulnerability, neurobiological dysfunction, temperament, emotional dysregulation, ADHD symptoms, family processes, deviant peer affiliations, neighborhood violence) and protective (e.g., positive parenting, emotion socialization, scholastic achievement, prosocial peer relationships) factors over time (see Beauchaine & McNulty, Reference Beauchaine and McNulty2013; Losel & Farrington, Reference Losel and Farrington2012). Ultimately, it will be important to determine whether the developmental processes involved with declining childhood conduct problems are unique from those involved with persistent childhood conduct problems, or simply more circumscribed. Empirical answers to these questions would allow for the identification of more individualized treatment targets for "early starters," which could enhance the efficacy and cost-effectiveness of interventions.
Acknowledgements
This work used data from the Fast Track project (for additional information concerning Fast Track, see http://www.fasttrackproject.org). We are grateful to the members of the Conduct Problems Prevention Research Group (in alphabetical order, Karen L. Bierman, Pennsylvania State University; John D. Coie, Duke University; D. Max Crowley, Pennsylvania State University; Kenneth A. Dodge, Duke University; Mark T. Greenberg, Pennsylvania State University; John E. Lochman, University of Alabama; Robert J. McMahon, Simon Fraser University and B.C. Children's Hospital Research Institute, and Ellen E. Pinderhughes, Tufts University) for providing the data and for additional involvement.
The Fast Track project has been supported by National Institute of Mental Health (NIMH) Grants R18 MH48043, R18 MH50951, R18 MH50952, R18 MH50953, K05MH00797, and K05MH01027; National Institute on Drug Abuse (NIDA) Grants DA016903, K05DA15226, RC1DA028248, and P30DA023026; National Institute of Child Health and Human Development Grant R01 HD093651; and Department of Education Grant S184U30002. The Center for Substance Abuse Prevention also provided support through a memorandum of agreement with the NIMH. Additional support for this study was provided by a B.C. Children's Hospital Research Institute Investigator Grant Award and a Canada Foundation for Innovation award to Robert J. McMahon, as well as a Canadian Institudes of Health Research (CIHR) Frederick Banting and Charles Best Canada Graduate Scholarship-Master's to Maeve Cyr.
We are grateful for the collaboration of the Durham Public Schools, the Metropolitan Nashville Public Schools, the Bellefonte Area Schools, the Tyrone Area Schools, the Mifflin County Schools, the Highline Public Schools, and the Seattle Public Schools. We appreciate the hard work and dedication of the many staff members who implemented the project, collected the evaluation data, and assisted with data management and analyses.







